20-F: Annual and transition report of foreign private issuers pursuant to Section 13 or 15(d)
Published on June 16, 2015
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
_________________
FORM 20-F
________________
________________
|
¨
|
REGISTRATION STATEMENT PURSUANT TO SECTION 12(b) or (g) OF THE SECURITIES EXCHANGE ACT OF 1934
|
OR
|
x
|
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE FISCAL YEAR ENDED FEBRUARY 28, 2015
|
OR
|
¨
|
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
|
OR
|
¨
|
SHELL COMPANY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
|
Commission file number: 001-35776
_________________
Acasti Pharma Inc.
(Exact name of Registrant as specified in its charter)
_________________
N/A
(Translation of Registrant’s name into English)
Québec, Canada
(Jurisdiction of incorporation or organization)
545, Promenade du Centropolis, Suite 100, Laval, Québec H7T 0A3
(Address of principal executive office)
Jean-Daniel Bélanger
545, Promenade du Centropolis, Suite 100
Laval, Québec H7T 0A3
Tel: 450-687-2262
Fax: 450-687-2272
(Name, Telephone, Email and/or Facsimile number and Address of Company Contact Person)
Securities registered or to be registered pursuant to Section 12(b) of the Act.
|
Title of each class
|
Name of each exchange on which registered
|
|
Common Shares, no par value
|
The NASDAQ Capital Market
|
Securities registered or to be registered pursuant to Section 12(g) of the Act.
Not applicable
Securities for which there is a reporting obligation pursuant to Section 15(d) of the Act.
None
_____________________
Indicate the number of outstanding shares of each of the issuer’s classes of capital or common stock as of the close of the period covered by the annual report.
106,444,012 Common Shares issued and outstanding as of May 27, 2015.
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
If this report is an annual or transition report, indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ¨ No ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, or a non-accelerated filer. See definition of “accelerated filer and large accelerated filer” in Rule 12b-2 of the Exchange Act. (Check one):
Large accelerated filer ¨ Accelerated filer ¨ Non-accelerated filer x
Indicate by check mark which basis of accounting the registrant has used to prepare the financial statements included in this filing:
|
U.S. GAAP ¨
|
International Financial Reporting Standards as
issued by the International Accounting Standards Board x
|
Other ¨
|
If “Other” has been checked in response to the previous question, indicate by check mark which financial statement item the registrant has elected to follow.
Item 17 ¨ Item 18 ¨
If this is an annual report, indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No x
TABLE OF CONTENTS
|
PAGE
|
|
|
PART I
|
|
|
SELECTED QUARTERLY FINANCIAL DATA
|
47
|
|
PART II
|
|
|
PART III
|
|
INTRODUCTION AND USE OF CERTAIN TERMS
As used in this annual report on Form 20-F, or the Annual Report, unless the context otherwise requires, references to “Acasti”, “Acasti Pharma”, “Corporation”, “it”, “its”, “we”, “our”, “us” or similar terms refer to Acasti Pharma Inc., references to “Neptune” refer to Acasti’s parent company, Neptune Technologies & Bioressources Inc., and references to “NeuroBioPharm” refer to Acasti’s sister company, NeuroBioPharm Inc.
Market data and certain industry data and forecasts included in this Annual Report were obtained from internal company surveys, market research, publicly available information, reports of governmental agencies and industry publications and surveys. We have relied upon industry publications as our primary sources for third-party industry data and forecasts. Industry surveys, publications and forecasts generally state that the information contained therein has been obtained from sources believed to be reliable, but that the accuracy and completeness of such information is not guaranteed. We have not independently verified any of the data from third-party sources, nor have we ascertained the underlying economic assumptions relied upon therein. Similarly, internal surveys, industry forecasts and market research, which we believe to be reliable based upon management’s knowledge of the industry, have not been independently verified. Forecasts are particularly likely to be inaccurate, especially over long periods of time. In addition, we do not know what assumptions regarding general economic growth were used in preparing the forecasts cited in this Annual Report. While we are not aware of any misstatements regarding Acasti’s industry data presented herein, our estimates involve risks and uncertainties and are subject to change based on various factors, including those discussed under “Risk Factors” in this Annual Report. While we believe our internal business research is reliable and market definitions are appropriate, neither such research nor definitions have been verified by any independent source. This Annual Report may only be used for the purpose for which it has been published.
Financial Information
All financial information is presented in accordance with International Financial Reporting Standards, or IFRS, as issued by the International Accounting Standards Board, or IASB, other than certain non-IFRS financial measures which are defined under “Reconciliation of the Adjusted Earnings Before Interest, Taxes, Depreciation and Amortization (Adjusted EBITDA)”, in our Management’s Analysis of the financial situation and Operating Results, or MD&A below.
In this Annual Report, all references to “CAD” or “$” are to Canadian Dollars unless expressly otherwise stated.
Exchange Rate Table
The following table sets forth the average exchange rate for one Canadian dollar expressed in terms of one U.S. dollar for each of the last five fiscal years. The average rate is calculated using the average of the exchange rates on the last day of each month during the period.
|
Average
|
||||
|
2010
|
0.9671 | |||
|
2011
|
1.0151 | |||
|
2012
|
1.0008 | |||
|
2013
|
0.9903 | |||
|
2014
|
0.9555 | |||
|
2015
|
0.8003 | |||
The following table sets forth the high and low exchange rates for each month during the previous six months.
|
Low
|
High
|
|||||||
|
December 2014
|
0.8589 | 0.8815 | ||||||
|
January 2015
|
0.7863 | 0.8527 | ||||||
|
February 2015
|
0.7915 | 0.8063 | ||||||
|
March 2015
|
0.7811 | 0.8039 | ||||||
|
April 2015
|
0.7929 | 0.8365 | ||||||
|
May 2015
|
0.8010 | 0.8368 | ||||||
|
June 2015 (up to June 15)
|
0.7968 | 0.8152 | ||||||
The exchange rates are based upon the noon buying rate as quoted by the Bank of Canada. At June 15, 2015, the exchange rate for one Canadian dollar expressed in terms of one U.S. dollar, as quoted by The Bank of Canada Eastern Time, equaled $0.8115.
1
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report contains certain information that may constitute forward-looking statements within the meaning of U.S. federal securities laws, which we refer to in this Annual Report as forward-looking information. Forward-looking information can be identified by the use of terms such as “may”, “will”, “should”, “expect”, “plan”, “anticipate”, “believe”, “intend”, “estimate”, “predict”, “potential”, “continue” or other similar expressions concerning matters that are not statements about the present or historical facts. Forward-looking information in this Annual Report includes, but is not limited to, information or statements about:
|
|
·
|
Acasti’s ability to conduct all required clinical and nonclinical trials for CaPre®, including the timing and results of those clinical trials;
|
|
|
·
|
Acasti’s ability to commercialize and distribute CaPre® and ONEMIA® in the United States and elsewhere;
|
|
|
·
|
Acasti’s estimates of the size of the potential markets for CaPre® and ONEMIA® and the rate and degree of market acceptance of CaPre® and ONEMIA®;
|
|
|
·
|
the benefits of CaPre® and ONEMIA® as compared to other products in the pharmaceutical and medical food markets, respectively;
|
|
|
·
|
Acasti’s ability to maintain and defend its intellectual property rights;
|
|
|
·
|
Acasti’s ability to maintain its supply of raw materials, including krill oil, from its parent company;
|
|
|
·
|
Acasti’s ability to secure a third-party supplier to provide Acasti, as needed, with raw materials to supplement its operations, including raw krill oil (“RKO”), used to manufacture CaPre® and ONEMIA®;
|
|
|
·
|
Acasti’s ability to secure and maintain a third-party to manufacture CaPre® whose manufacturing processes and facilities are in compliance with current good manufacturing practices (“cGMP”);
|
|
|
·
|
Acasti’s ability to obtain and maintain regulatory approval of CaPre®, and the labeling requirements that would apply under any approval Acasti may obtain;
|
|
|
·
|
regulatory developments affecting the pharmaceutical and medical food markets in the United States and elsewhere;
|
|
|
·
|
the size and growth of the potential markets for CaPre® and ONEMIA® and Acasti’s ability to serve those markets;
|
|
|
·
|
the rate and degree of market acceptance of CaPre®, if it reaches commercialization;
|
|
|
·
|
the success of competing products that are or become available; and
|
|
|
·
|
Acasti’s expectations regarding its financial performance, including its revenues, research and development, expenses, gross margins, liquidity, capital resources and capital expenditures.
|
Although the forward-looking information in this Annual Report is based upon what Acasti believes are reasonable assumptions, no person should place undue reliance on such information since actual results may vary materially from the forward-looking information.
In addition, the forward-looking information in this Annual Report is subject to a number of known and unknown risks, uncertainties and other factors, including those described in this Annual Report under the heading “Risk Factors”, many of which are beyond the Corporation’s control, that could cause the Corporation’s actual results and developments to differ materially from those that are disclosed in or implied by the forward-looking information, including, without limitation:
|
|
·
|
whether the current and future clinical trials by the Corporation will be successful;
|
|
|
·
|
whether CaPre® and ONEMIA® can be successfully commercialized;
|
|
|
·
|
the Corporation’s reliance on third parties for the manufacture, supply and distribution of its products and for the supply of raw materials, including the ability to find a third party to supply RKO in sufficient quantities and quality and to produce CaPre® under cGMP standards;
|
2
|
|
·
|
the Corporation’s reliance on a limited number of distributors for ONEMIA® and its ability to secure distribution arrangements for CaPre® if it reaches commercialization;
|
|
|
·
|
the Corporation’s ability to manage future growth effectively;
|
|
|
·
|
the Corporation’s ability to achieve profitability;
|
|
|
·
|
the Corporation’s ability to secure future financing from Neptune or other third party sources on favorable terms or at all;
|
|
|
·
|
the Corporation’s ability to gain acceptance of its products in its markets;
|
|
|
·
|
the Corporation’s ability to attract, hire and retain key management and scientific personnel;
|
|
|
·
|
the Corporation’s ability to achieve its publicly announced milestones on time;
|
|
|
·
|
the Corporation’s ability to successfully defend any product liability lawsuits that may be brought against it;
|
|
|
·
|
intense competition from other companies in the pharmaceutical and medical food industries;
|
|
|
·
|
the Corporation’s ability to secure and defend its intellectual property rights and to avoid infringing upon the intellectual property rights of third parties; and
|
|
|
·
|
the Corporation’s status as a foreign private issuer/emerging growth company.
|
Consequently, all the forward-looking information in this Annual Report is qualified by this cautionary statement and there can be no guarantee that the results or developments that the Corporation anticipates will be realized or, even if substantially realized, that they will have the expected consequences or effects on the Corporation’s business, financial condition or results of operations. Accordingly, you should not place undue reliance on the forward-looking information. Except as required by applicable law, Acasti does not undertake to update or amend any forward-looking information, whether as a result of new information, future events or otherwise. All forward-looking information is made as of the date of this Annual Report.
3
PART I
|
Item 1.
|
Identity of Directors, Senior Management and Advisers
|
Not applicable.
|
Item 2.
|
Offer Statistics and Expected Timetable
|
Not applicable.
|
Item 3.
|
Key Information
|
|
A.
|
Selected Financial Data
|
The following information should be read in conjunction with our MD&A and our audited consolidated financial statements and the related notes, which are prepared in accordance with IFRS as issued by the IASB. The selected financial information includes financial information derived from the annual audited consolidated financial statements. Our historical results from any prior period are not necessarily indicative of results to be expected for any future period.
The following table is a summary of selected consolidated financial information of the Corporation for each of the five most recently completed fiscal years in accordance with IFRS as issued by the IASB.
|
February 28, 2015
|
February 28, 2014
|
February 28, 2013
|
February 29, 2012
|
February 28, 2011
|
||||||||||||||||
|
Revenue from sales
|
$ | 270,615 | $ | 500,875 | $ | 724,196 | $ | 10,415 | $ | — | ||||||||||
|
Results from operating activities (1)
|
$ | (12,394,461 | ) | $ | (10,799,706 | ) | $ | (6,979,733 | ) | $ | (6,512,842 | ) | $ | (3,118,515 | ) | |||||
|
Net loss and total comprehensive loss (1)
|
$ | (1,654,724 | ) | $ | (11,611,649 | ) | $ | (6,892,360 | ) | $ | (6,500,933 | ) | $ | (3,008,226 | ) | |||||
|
Basic and diluted loss per share
|
$ | (0.02 | ) | $ | (0.14 | ) | $ | (0.09 | ) | $ | (0.10 | ) | $ | (0.06 | ) | |||||
|
Total assets
|
$ | 37,208,105 | $ | 45,631,803 | $ | 12,170,048 | $ | 15,728,860 | $ | 10,830,771 | ||||||||||
|
Total liabilities
|
$ | 3,979,786 | $ | 12,352,303 | $ | 2,446,372 | $ | 1,259,518 | $ | 5,125,935 | ||||||||||
|
Share capital
|
61,627,743 | 61,027,307 | 28,922,710 | 28,614,550 | 12,174,901 | |||||||||||||||
|
Warrants and rights
|
– | 406,687 | 406,687 | 313,315 | — | |||||||||||||||
|
Weighted average number of shares outstanding
|
106,177,039 | 84,368,933 | 72,754,436 | 67,231,636 | 50,772,550 | |||||||||||||||
|
Dividends declared per share
|
— | — | — | — | — | |||||||||||||||
|
B.
|
Capitalization and Indebtedness
|
Not applicable.
|
C.
|
Reasons for the Offer and Use of Proceeds
|
Not applicable.
|
D.
|
Risk Factors
|
Investing in the Common Shares involves a high degree of risk. Prospective and current investors should carefully consider the following risks and uncertainties, together with all other information in this Annual Report, as well as the Corporation’s financial statements and related notes and MD&A. Any of the risk factors described below could adversely affect Acasti’s business, financial condition or results of operations. The market price of the Common Shares could decline significantly if one or more of these risks or uncertainties actually occur. The risks below are not the only ones Acasti faces. Additional risks that Acasti currently does not know about or that Acasti currently believes to be immaterial may also impair its business. Certain statements below are forward-looking information. See “Special Note Regarding Forward-Looking Statements”.
4
Risks Related to Product Development, Regulatory Approval and Commercialization
The Corporation’s prospects currently depend entirely on the success of CaPre®, which is still in clinical development, and the Corporation may not be able to generate revenues from CaPre®.
The Corporation has no prescription drug products that have been approved by the FDA, Health Canada or any similar regulatory authority. The Corporation’s only prescription drug candidate is CaPre®, for which the Corporation has not yet filed an NDA, and for which the Corporation must still initiate Phase III clinical trials, undergo further development activities and seek and receive regulatory approval prior to commercial launch, which the Corporation does not anticipate will occur until the Corporation’s fiscal year beginning in 2018 at the earliest. The Corporation does not have any other prescription drug candidates in development and, therefore, the Corporation’s business prospects currently depend entirely on the successful development, regulatory approval and commercialization of CaPre®, which may never occur. Most prescription drug candidates never reach the clinical development stage and even those that do reach clinical development have only a small chance of successfully completing clinical development and gaining regulatory approval. If the Corporation is unable to successfully commercialize CaPre® for the prevention and treatment of hypertriglyceridemia or severe hypertriglyceridemia, it may never generate meaningful revenues. In addition, if CaPre® reaches commercialization and there is low market demand for CaPre® or the market for CaPre® develops less rapidly than the Corporation anticipates, the Corporation may not have the ability to shift its resources to the development of alternative products.
The Corporation may not be able to obtain required regulatory approvals for CaPre®.
The research, testing, manufacturing, labeling, packaging, storage, approval, sale, marketing, advertising and promotion, pricing, export, import and distribution of prescription drug products are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries and those regulations differ from country to country. Acasti is not permitted to market CaPre® in the United States until it receives approval of an NDA from the FDA and similar restrictions apply in other countries. In the United States, the FDA generally requires the completion of preclinical testing and clinical trials of each drug to establish its safety and efficacy and extensive pharmaceutical development to ensure its quality before an NDA is approved. Regulatory authorities in other jurisdictions impose similar requirements. Of the large number of drugs in development, only a small percentage result in the submission of an NDA to the FDA and even fewer are approved for commercialization. To date, the Corporation has not submitted an NDA for CaPre® to the FDA or comparable applications to other regulatory authorities. If the Corporation’s development efforts for CaPre®, including its planned Phase III clinical trials, are not successful for the prevention and treatment of hypertriglyceridemia or severe hypertriglyceridemia, and regulatory approval is not obtained in a timely fashion or at all, the Corporation’s business will be materially adversely affected.
The receipt of required regulatory approvals for CaPre® is uncertain and subject to a number of risks, including the following:
|
|
·
|
the FDA or comparable foreign regulatory authorities or IRBs may disagree with the design or implementation of the Corporation’s clinical trials;
|
|
|
·
|
the Corporation may not be able to provide acceptable evidence of the safety and efficacy of CaPre®;
|
|
|
·
|
the results of the Corporation’s clinical trials may not meet the level of statistical or clinical significance required by the FDA or other regulatory agencies for marketing approval;
|
|
|
·
|
the dosing of CaPre® in a particular clinical trial may not be at an optimal level;
|
|
|
·
|
patients in the Corporation’s clinical trials may suffer adverse effects for reasons that may or may not be related to CaPre®;
|
|
|
·
|
the data collected from the Corporation’s clinical trials may not be sufficient to support the submission of an NDA for CaPre® or to obtain regulatory approval for CaPre® in the United States or elsewhere;
|
|
|
·
|
the FDA or comparable foreign regulatory authorities may not approve the manufacturing processes or facilities of third-party manufacturers with which the Corporation contracts for clinical and commercial supplies; and
|
|
|
·
|
the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering the Corporation’s clinical data insufficient for approval.
|
5
The FDA and other regulators have substantial discretion in the approval process and may refuse to accept any application or may decide that the Corporation’s data is insufficient for approval and require additional clinical trials, or preclinical or other studies. In addition, varying interpretations of the data obtained from preclinical studies and clinical trials could delay, limit or prevent regulatory approval of CaPre®. In addition, the process of obtaining regulatory approvals is expensive, often takes many years, if approval is obtained at all, and can vary substantially based upon, among other things, the type, complexity and novelty of the prescription drug candidates involved, the jurisdiction in which regulatory approval is sought and the substantial discretion of the regulatory authorities. Changes in the regulatory approval policy during the development period, changes in or the enactment of additional statutes or regulations, or changes in regulatory review for a submitted product application may cause delays in the approval or rejection of an application. If regulatory approval is obtained in one jurisdiction, that does not necessarily mean that CaPre® will receive regulatory approval in all jurisdictions in which the Corporation may seek approval. The failure to obtain approval for CaPre® in one or more jurisdictions may negatively impact the Corporation’s ability to obtain approval in a different jurisdiction. A failure to obtain regulatory marketing approval for CaPre® in any indication would prevent the Corporation from commercializing CaPre®, and the Corporation’s ability to generate revenue would be materially impaired.
The Corporation may be unable to develop alternative product candidates.
To date, the Corporation has not commercialized any prescription drug candidates and does not have any other compounds in clinical trials, nonclinical testing, lead optimization or lead identification stages besides CaPre®. The Corporation cannot be certain that CaPre® will prove to be sufficiently effective and safe to meet applicable regulatory standards for any indication. If the Corporation fails to successfully commercialize CaPre® as a treatment for hypertriglyceridemia and severe hypertriglyceridemia, or any other indication, whether as a stand-alone therapy or in combination with other treatments, the Corporation would have to develop, acquire or license alternative product candidates or drug compounds to expand its product candidate pipeline beyond CaPre®. In such a scenario, the Corporation may not be able to identify, and acquire product candidates that prove to be successful products, or to acquire them on terms that are acceptable to the Corporation.
Even if the Corporation receives regulatory approval for CaPre®, the Corporation still may not be able to successfully commercialize it and the revenue that the Corporation generates from its sales, if any, may be limited.
The commercial success of CaPre® in any indication for which the Corporation obtains marketing approval from the FDA or other regulatory authorities will depend upon its acceptance by the medical community, including physicians, patients and health insurance providers. The degree of market acceptance of CaPre® will depend on a number of factors, including:
|
|
·
|
demonstration of clinical safety and efficacy of prescription omega-3 products generally;
|
|
|
·
|
relative convenience, pill burden and ease of administration;
|
|
|
·
|
the prevalence and severity of any adverse side effects;
|
|
|
·
|
the willingness of physicians to prescribe CaPre® and of the target patient population to try new therapies;
|
|
|
·
|
efficacy of CaPre® compared to competing products, including omega-3 dietary supplements;
|
|
|
·
|
the introduction of any new products, including generic prescription omega-3 products, that may in the future become available to treat indications for which CaPre® may be approved;
|
|
|
·
|
new procedures or methods of treatment that may reduce the incidences of any of the indications for which CaPre® shows utility;
|
|
|
·
|
pricing;
|
|
|
·
|
the inclusion of prescription omega-3 products in applicable treatment guidelines;
|
|
|
·
|
the effectiveness of the Corporation’s or any future collaborators’ sales and marketing strategies;
|
|
|
·
|
limitations or warnings contained in FDA-approved labeling;
|
|
|
·
|
the Corporation’s ability to obtain and maintain sufficient third-party coverage or reimbursement from government health care programs, including Medicare and Medicaid, private health insurers and other third-party payors; and
|
|
|
·
|
the willingness of patients to pay out-of-pocket in the absence of third-party coverage or reimbursement.
|
6
In addition, even if the Corporation obtains regulatory approvals, the timing or scope or conditions of any approvals may prohibit or reduce the Corporation’s ability to commercialize CaPre® successfully. For example, if the approval process takes too long, the Corporation may miss market opportunities and give other companies the ability to develop competing products or establish market dominance. Any regulatory approval the Corporation ultimately obtains may be limited or subject to restrictions or post-approval commitments that render CaPre® not commercially viable. For example, regulatory authorities may not approve the price the Corporation intends to charge for CaPre®, may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve CaPre® with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that indication. Any of the foregoing scenarios could have a material adverse effect on the commercial prospects for CaPre®. If CaPre® is approved, but does not achieve an adequate level of acceptance by physicians, health insurance providers and patients, the Corporation may not generate sufficient revenue and the Corporation may not be able to ever achieve profitability.
The Corporation faces competition from other biotechnology and pharmaceutical companies and its operating results will suffer if the Corporation fails to compete effectively.
The biotechnology and pharmaceutical industries are intensely competitive and subject to rapid and significant technological change. The Corporation’s potential competitors both in the United States and globally include large, well-established pharmaceutical companies, specialty pharmaceutical sales and marketing companies and specialized cardiovascular treatment companies. Many of these competitors have substantially greater name recognition, commercial infrastructures and financial, technical and personnel resources than the Corporation. These companies include GlaxoSmithKline plc, which currently markets Lovaza, a prescription omega-3 for patients with severe hypertriglyceridemia, and Abbott Laboratories, which currently markets Tricor and Trilipix (both fibrates) and Niaspan (niacin) for treatment of severe hypertriglyceridemia and high triglycerides, Amarin Corporation, which currently markets Vascepa, an ethyl-ester form of EPA, for the treatment of patients with severe hypertriglyceridemia and AstraZeneca which announced on May 6, 2014 that the FDA had approved EPANOVA (omega-3-carboxylic acids) as an adjunct to diet to reduce triglyceride levels in adults with severe hypertriglyceridaemia. In addition, Acasti is aware of other pharmaceutical companies (e.g Matinas Biopharma) that are developing products that, if approved, would compete with CaPre®. CaPre® may also compete with omega-3 dietary supplements that are available without a prescription. These established competitors and others may invest heavily to quickly discover and develop novel compounds that could make CaPre® obsolete or uneconomical. CaPre® may need to demonstrate compelling comparative advantages in efficacy, convenience, tolerability and safety to be commercially successful. Other competitive factors, including generic drug competition, could force the Corporation to lower prices or could result in reduced sales. In addition, new products developed by others could emerge as competitors to CaPre®. If the Corporation is not able to compete effectively against its current and future competitors, its business will not grow and its financial condition and operations will suffer.
CaPre®, if approved, would be subject to competition from products for which no prescription is required.
If approved by applicable regulatory authorities, CaPre® will be a prescription-only omega-3. Mixtures of omega-3 fatty acids are naturally occurring substances in various foods, including fatty fish. Omega-3 fatty acids are also marketed by others as dietary supplements. Dietary supplements may generally be marketed without a lengthy FDA premarket review and approval process and are not subject to prescription. However, unlike prescription drug products, manufacturers of dietary supplements may not make therapeutic claims for their products; dietary supplements may be marketed with claims describing how the product affects the structure or function of the body without premarket approval, but may not expressly or implicitly represent that the dietary supplement will diagnose, cure, mitigate, treat, or prevent disease. The Corporation believes the pharmaceutical-grade purity of CaPre® has a superior therapeutic profile to naturally occurring omega-3 fatty acids and the omega-3 in commercially available dietary supplements. However, the Corporation cannot be certain that physicians or consumers will view CaPre® as superior. To the extent the price of CaPre® is significantly higher than the prices of commercially available omega-3 fatty acids marketed by other companies as dietary supplements, physicians may recommend these commercial alternatives instead of CaPre® or patients may elect on their own to take commercially available non-prescription omega-3 fatty acids. Either of these outcomes may adversely impact the Corporation’s results of operations by limiting how the Corporation prices CaPre® and limiting the revenue the Corporation receives from the sale of CaPre®.
Even if the Corporation obtains marketing approval for CaPre®, the Corporation will be subject to ongoing obligations and continued regulatory review, which may result in significant additional expense.
Even if the Corporation obtains U.S. regulatory approval for CaPre® for the prevention and treatment of hypertriglyceridemia or severe hypertriglyceridemia, which would not occur until the Corporation successfully completes Phase III clinical trials, the FDA may still impose significant restrictions on its indicated uses or marketing or the conditions of approval, or impose ongoing requirements for potentially costly and time-consuming post-approval studies, including Phase IV clinical trials or clinical outcome studies, and post-market surveillance to monitor the safety and efficacy of CaPre®. Even if the Corporation secures U.S. regulatory approval, the Corporation would continue to be subject to ongoing regulatory requirements related to CaPre® governing manufacturing, labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, recordkeeping and reporting of adverse events and other post-market information. These requirements include registration with the FDA, as well as continued compliance with cGCPs, for any clinical trials that the Corporation conducts post-approval. In addition, manufacturers of drug products and their facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with cGMP, requirements relating to quality control, quality assurance and corresponding maintenance of records and documents.
7
If the Corporation or a regulatory agency discovers previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, problems with the facility where the product is manufactured, or the Corporation or its manufacturers fail to comply with applicable regulatory requirements, the Corporation may be subject to the following administrative or judicial sanctions:
|
|
·
|
restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market, or voluntary or mandatory product recalls;
|
|
|
·
|
issuance of warning letters or untitled letters;
|
|
|
·
|
clinical holds;
|
|
|
·
|
injunctions or the imposition of civil or criminal penalties or monetary fines;
|
|
|
·
|
suspension or withdrawal of regulatory approval;
|
|
|
·
|
suspension of any ongoing clinical trials;
|
|
|
·
|
refusal to approve pending applications or supplements to approved applications filed by the Corporation, or suspension or revocation of product license approvals;
|
|
|
·
|
suspension or imposition of restrictions on operations, including costly new manufacturing requirements; or
|
|
|
·
|
product seizure or detention or refusal to permit the import or export of product.
|
The occurrence of any event or penalty described above may inhibit the Corporation’s ability to commercialize CaPre® and generate revenue. Adverse regulatory action, whether pre- or post-approval, can also potentially lead to product liability claims and increase the Corporation’s product liability exposure. See “ Government Regulation”.
Recently enacted and future legislation may increase the difficulty and cost for the Corporation to obtain marketing approval of and commercialize CaPre® and affect the prices the Corporation may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval for CaPre®, restrict or regulate post-approval activities and affect the Corporation’s ability to profitably sell CaPre®. Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. The Corporation does not know whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of CaPre®, if any, may be. In addition, increased scrutiny by the U.S. Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject the Corporation to more stringent product labeling and post-marketing testing and other requirements.
In the United States, the Medicare Modernization Act, or MMA, changed the way Medicare covers and pays for pharmaceutical products. The legislation expanded Medicare coverage for drug purchases by the elderly and introduced a new reimbursement methodology based on average sales prices for drugs. In addition, this legislation authorized Medicare Part D prescription drug plans to use formularies where they can limit the number of drugs that will be covered in any therapeutic class. As a result of this legislation and the expansion of federal coverage of drug products, the Corporation expects that there will be additional pressure to contain and reduce costs. These cost reduction initiatives and other provisions of this legislation could decrease the coverage and price that the Corporation receives for CaPre® and could seriously harm its business. While the MMA applies only to drug benefits for Medicare beneficiaries, private health insurance companies often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates, and any reduction in reimbursement that results from the MMA may result in a similar reduction in payments from private health insurance companies.
8
In March 2010, President Obama signed into law the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act of 2010 or, collectively, the Health Care Reform Law, a sweeping law intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms. Effective October 1, 2010, the Health Care Reform Law revised the definition of “average manufacturer price” for reporting purposes, which could increase the amount of Medicaid drug rebates to states. Further, the new law imposed a significant annual fee on companies that manufacture or import branded prescription drug products. Substantial new provisions affecting compliance have also been enacted, which may possibly require the Corporation to modify its business practices with healthcare practitioners.
Despite initiatives to invalidate the Health Care Reform Law, the U.S. Supreme Court has upheld certain key aspects of the legislation, including the requirement that all individuals maintain health insurance coverage or pay a penalty, referred to as the individual mandate. Although there are legal challenges to the Health Care Reform Law in lower courts on other grounds, at this time it appears the implementation of the Health Care Reform Law will continue. The Corporation will not know the full effects of the Health Care Reform Law until applicable federal and state agencies issue regulations or guidance under the new law. Although it is too early to determine the effect of the Health Care Reform Law, the new law appears likely to continue the pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase the Corporation’s regulatory burdens and operating costs. The Corporation expects that additional federal healthcare reform measures will be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, and in turn could significantly reduce the projected value of certain development projects and reduce the Corporation’s ability to achieve profitability.
If the Corporation markets CaPre® in a manner that violates healthcare fraud and abuse laws, or if the Corporation violates government price reporting laws, the Corporation may be subject to civil or criminal penalties.
In addition to FDA restrictions on marketing of pharmaceutical products, several other types of federal and state healthcare fraud and abuse laws have been applied in recent years to restrict certain marketing practices in the pharmaceutical industry. These laws include the U.S. Anti-Kickback Statute, U.S. False Claims Act and similar state laws. Because of the breadth of these laws and the narrowness of the safe harbors, it is possible that some of the Corporation’s business activities could be subject to challenge under one or more of these laws.
The U.S. Anti-Kickback Statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving remuneration to induce, or in return for, purchasing, leasing, ordering or arranging for the purchase, lease or order of any healthcare item or service reimbursable under Medicare, Medicaid or other federally financed healthcare programs. This statute has been interpreted broadly to apply to arrangements between pharmaceutical manufacturers on the one hand and prescribers, dispensers, purchasers and formulary managers on the other. Although there are several statutory exemptions and regulatory safe harbors protecting certain common activities from prosecution, the exemptions and safe harbors are drawn narrowly, and practices that involve remuneration intended to induce prescribing, purchasing or recommending drugs reimbursable under federal healthcare programs may be subject to scrutiny if they do not qualify for an exemption or safe harbor. The Corporation’s practices may not, in all cases, meet all of the criteria for safe harbor protection from anti-kickback liability. Moreover, recent health care reform legislation has strengthened these laws. For example, the Health Care Reform Law, among other things, amends the intent requirement of the U.S. Anti-Kickback Statute and criminal health care fraud statutes; a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. In addition, the Health Care Reform Law provides that the government may assert that a claim including items or services resulting from a violation of the U.S. Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the U.S. False Claims Act. Federal false claims laws prohibit any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government or knowingly making, or causing to be made, a false statement to get a false claim paid.
Over the past few years, a number of pharmaceutical and other healthcare companies have been prosecuted under these laws for a variety of alleged promotional and marketing activities, such as: allegedly providing free trips, free goods, sham consulting fees and grants and other monetary benefits to prescribers; reporting to pricing services inflated average wholesale prices that were then used by federal programs to set reimbursement rates; engaging in off-label promotion that caused claims to be submitted to Medicaid for non-covered, off-label uses; and submitting inflated best price information to the Medicaid Rebate Program to reduce liability for Medicaid rebates. Most states also have statutes or regulations similar to the U.S. Anti-Kickback Statute and the U.S. False Claims Act, which apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payor. Sanctions under these federal and state laws may include civil monetary penalties, exclusion of a manufacturer’s products from reimbursement under government programs, criminal fines and imprisonment. Settlements of government litigation may include Corporate Integrity Agreements with commitments for monitoring, training, and reporting designed to prevent future violations.
9
Third-party coverage and reimbursement and health care cost containment initiatives and treatment guidelines may constrain the Corporation’s future revenues.
The Corporation’s ability to successfully market CaPre® will depend in part on the level of reimbursement that government health administration authorities, private health coverage insurers and other organizations provide for the cost of the Corporation’s products and related treatments. Countries in which CaPre® may in the future be sold through reimbursement schemes under national health insurance programs frequently require that manufacturers and sellers of pharmaceutical products obtain governmental approval of initial prices and any subsequent price increases. In certain countries, including the United States, government-funded and private medical care plans can exert significant indirect pressure on prices. The Corporation may not be able to sell CaPre® profitably if its prices are not approved or coverage and reimbursement is unavailable or limited in scope. Increasingly, third-party payors attempt to contain health care costs in ways that are likely to impact the Corporation’s development of products including:
|
|
·
|
not approving the prices charged for health care products;
|
|
|
·
|
limiting both coverage and the amount of reimbursement for new therapeutic products;
|
|
|
·
|
denying or limiting coverage for products that are approved by the regulatory agencies but are considered to be experimental or investigational by third-party payors; and
|
|
|
·
|
refusing to provide coverage when an approved product is used in a way that has not received regulatory marketing approval.
|
Termination or suspension of, or delays in the commencement or completion of, any necessary future studies of CaPre® for any indications could occur.
The commencement and completion of clinical and non-clinical studies for CaPre® can be delayed for a number of reasons, including delays related to:
|
|
·
|
the FDA, Health Canada or similar regulatory authorities not granting permission to proceed and placing the clinical study on hold;
|
|
|
·
|
subjects failing to enroll or remain in the Corporation’s trials at the rate the Corporation expects;
|
|
|
·
|
a facility manufacturing CaPre® being ordered by the FDA or other government or regulatory authorities to temporarily or permanently shut down due to violations of cGMP requirements or other applicable requirements, or cross-contaminations of product candidates in the manufacturing process;
|
|
|
·
|
any changes to the Corporation’s manufacturing process that may be necessary or desired;
|
|
|
·
|
subjects choosing an alternative treatment for the indications for which the Corporation is developing CaPre®, or participating in competing clinical studies;
|
|
|
·
|
subjects experiencing severe or unexpected drug-related adverse effects;
|
|
|
·
|
reports from clinical testing on similar technologies and products raising safety and/or efficacy concerns;
|
|
|
·
|
third-party clinical investigators losing their license or permits necessary to perform the Corporation’s clinical trials, not performing the Corporation’s clinical trials on their anticipated schedule or employing methods not consistent with the clinical trial protocol, cGMP requirements, or other third parties not performing data collection and analysis in a timely or accurate manner;
|
|
|
·
|
inspections of clinical study sites by the FDA, Health Canada or similar regulatory authorities or IRBs finding regulatory violations that require the Corporation to undertake corrective action, result in suspension or termination of one or more sites or the imposition of a clinical hold on the entire study, or that prohibit the Corporation from using some or all of the data in support of its marketing applications;
|
|
|
·
|
third-party contractors becoming debarred or suspended or otherwise penalized by the FDA, Health Canada or other government or regulatory authorities for violations of regulatory requirements, in which case the Corporation may need to find a substitute contractor, and the Corporation may not be able to use some or any of the data produced by such contractors in support of its marketing applications;
|
10
|
|
·
|
one or more IRBs refusing to approve, suspending or terminating the study at an investigational site, precluding enrollment of additional subjects, or withdrawing its approval of the trial; reaching agreement on acceptable terms with prospective CRO and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites;
|
|
|
·
|
deviations of the clinical sites from trial protocols or dropping out of a trial;
|
|
|
·
|
the addition of new clinical trial sites; and
|
|
|
·
|
the inability of the CRO to execute any clinical trials for any reason.
|
Product development costs for CaPre® will increase if the Corporation has delays in testing or approval or if the Corporation needs to perform more or larger clinical studies than planned. Additionally, changes in regulatory requirements and policies may occur and the Corporation may need to amend study protocols to reflect these changes. Amendments may require the Corporation to resubmit its study protocols to the FDA, Health Canada or similar regulatory authorities or IRBs for re-examination, which may impact the costs, timing or successful completion of that study. Any delays in completing the Corporation’s clinical trials will increase its costs, slow down its development and approval process and jeopardize its ability to commence sales of CaPre® and generate revenues. Any of these occurrences may have a material adverse effect on the Corporation’s business, financial condition and prospects.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The results of preclinical studies and early clinical trials may not be predictive of the results of later-stage clinical trials. For example, the positive preliminary results generated to date in the Corporation’s TRIFECTA Phase II clinical trial for CaPre® do not ensure that the final Phase II results or later clinical trials will produce similar results. The Corporation cannot assure you that the FDA will view the results as the Corporation does or that any future trials of CaPre® for other indications will achieve positive results. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through preclinical studies and initial clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. Any future clinical trial results for CaPre® may not be successful.
A number of factors could contribute to a lack of favorable safety and efficacy results for CaPre® for other indications. For example, such trials could result in increased variability due to varying site characteristics, such as local standards of care, differences in evaluation period, and due to varying patient characteristics including demographic factors and health status. There can be no assurance that the Corporation’s clinical trials will demonstrate sufficient safety and efficacy for the FDA to approve CaPre® for the prevention and treatment of hypertriglyceridemia and severe hypertriglyceridemia, or any other indication that the Corporation may consider in any additional NDA submissions for CaPre®.
In addition, clinical trials and nonclinical studies performed by research organizations and other independent third parties may yield negative results regarding the effect of omega-3 fatty acids on cardiometabolic disorders and specifically hypertriglyceridemia and severe hypertriglyceridemia. For example, in May 2013, the New England Journal of Medicine published results on a study in which it concluded that a daily treatment of omega-3 fatty acids did not reduce the risk of cardiovascular events. The clinical trial consisted of the enrollment of 12,513 patients who were followed by a network of 860 general practitioners in Italy. Patients were randomly assigned to omega-3 fatty acids (1g daily) or placebo. Researchers reported that omega-3 fatty acid supplements did not reduce death from heart disease or heart attacks or strokes in the group and concluded that the intake of omega-3 fatty acids does not have any specific advantage in a population that is considered at high risk of cardiovascular disease. The New England Journal of Medicine study along with other future studies yielding similar results could have a negative impact on consumer perception and market acceptance of the efficacy of omega-3 fatty acids on cardiometabolic disorders, specifically the beneficial effect on triglyceride and cholesterol levels, and such impact may a material adverse effect on the Corporation’s business.
The Corporation relies on third parties to conduct its clinical trials for CaPre®.
The Corporation has entered into agreements with a CRO to provide monitors for and to manage data for its ongoing clinical trials. The Corporation relies heavily on these parties for execution of clinical studies for CaPre® and controls only certain aspects of their activities. Nevertheless, the Corporation is responsible for ensuring that each of its studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards, and the Corporation’s reliance on CROs would not relieve it of its regulatory responsibilities. The Corporation and its CROs are required to comply with cGCPs, which are regulations and guidelines enforced by the FDA, Health Canada and comparable foreign regulatory authorities for any products in clinical development. The FDA enforces these cGCP regulations through periodic inspections of trial sponsors, principal investigators and trial sites. If the Corporation or its CROs fail to comply with applicable cGCPs, the clinical data generated in the Corporation’s clinical trials may be deemed unreliable and the FDA, Health Canada or comparable foreign regulatory authorities may require the Corporation to perform additional clinical trials before approving the Corporation’s marketing applications. The Corporation cannot assure you that, upon inspection, the FDA will determine that any of the Corporation’s clinical trials comply with cGCPs. In addition, the Corporation’s clinical trials must be conducted with products produced under cGMP regulations and require a large number of test subjects. The Corporation’s failure or the failure of its CROs to comply with these regulations may require the Corporation to repeat clinical trials, which would delay the regulatory approval process and could also subject the Corporation to enforcement action up to and including civil and criminal penalties.
11
If any of the Corporation’s relationships with these third-party CROs terminate, the Corporation may not be able to enter into arrangements with alternative CROs. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to the Corporation’s clinical protocols, regulatory requirements or for other reasons, any such clinical trials may be extended, delayed or terminated, and the Corporation may not be able to obtain regulatory approval for or successfully commercialize CaPre®.
The Corporation’s supply of krill oil for commercial supply and clinical trials is dependent upon relationships with Neptune and other third party manufacturers and key suppliers
The Corporation depends on krill oil sourced from third parties for the production of ONEMIA™ and CaPre®. The Corporation’s reliance on third party suppliers of krill oil involves several risks, including potential fluctuations in supply and reduced control over production costs, delivery schedules and the quality of available krill oil. Until November 2012, Acasti purchased all of its supply of krill oil from its parent company, Neptune. Acasti is currently acquiring its krill oil from Neptune and through purchases in the open market in order to meet production requirements for ONEMIA™, and is also relying on a third party to provide manufacturing services for the production of CaPre® in accordance with cGMP regulations imposed by the FDA. Furthermore, the Corporation will have to source additional quantities of krill oil for the continued production of ONEMIA™ and its planned Phase III clinical trial for CaPre®, and, if regulatory approval is obtained, larger quantities for the commercialization and distribution of CaPre® than the Corporation is currently able to source.
Acasti may not be able to acquire krill oil in sufficient quantities from Neptune, in which case, Acasti may need to seek alternative suppliers of krill oil and may be required to pay higher prices for krill oil (in comparison to what it currently pays to Neptune). Further, any alternative supply of krill oil may not be of comparable quality to that previously provided by Neptune which may impact the efficacy, or the markets’ perception of the efficacy, of ONEMIA™ and CaPre®. Disruption to the Corporation’s required quantities and quality of krill oil supplies would have a material adverse effect on Acasti’s business and results of operations.
The Corporation relies on third parties for the manufacturing, production and supply of CaPre® and ONEMIA® and may be adversely affected if those third parties are unable or unwilling to fulfill their obligations.
The production of pharmaceutical products requires significant expertise and capital investment, including the development of advanced manufacturing techniques and process controls. Acasti does not own or operate manufacturing facilities for the production of CaPre® and ONEMIA®, nor does it have plans to develop its own manufacturing operations in the foreseeable future. Accordingly, the Corporation needs to rely on one or more third party manufacturers to produce and supply its required drug product for its nonclinical research and clinical trials for CaPre® and its commercial sales of ONEMIA®. The Corporation’s reliance on third-parties to produce CaPre® and ONEMIA® exposes Acasti to a number of risks. For example, Acasti may be subject to delays in or suspension of the production of CaPre® and ONEMIA® if a third-party manufacturer:
|
|
·
|
becomes unavailable for any reason, including as a result of the failure to comply with current good manufacturing practices, or cGMP, regulations;
|
|
|
·
|
experiences manufacturing problems or other operational failures, such as equipment failures or unplanned facility shutdowns required to comply with cGMP or damage from any event, including fire, flood, earthquake, business restructuring or insolvency; or
|
|
|
·
|
fails or refuses to perform its contractual obligations under its agreement with the Corporation, such as failing or refusing to deliver the quantities requested on a timely basis.
|
If the Corporation’s third-party manufacturers fail to achieve and maintain high manufacturing standards in compliance with cGMP regulations, Acasti may be subject to sanctions, including fines, product recalls or seizures, injunctions, total or partial suspension of production, civil penalties, withdrawals of previously granted regulatory approvals, and criminal prosecution. Any of these penalties could delay the initiation of the Corporation’s planned Phase III clinical trial for CaPre®, which could have a material adverse effect on Acasti’s business prospects and result of operations.
12
The Corporation may be subject to Product Liability Claims and Recalls of its Products.
Drug development involves the testing of experimental drugs on human subjects. These studies subject the Corporation to liability risks relating to personal injury or, in extreme cases, death to participants as a result of an unexpected adverse reaction to the tested drug. Furthermore, the administration of these experimental drugs to humans after marketing clearance is obtained can result in product liability claims which may result from claims made directly by consumers or by regulatory agencies, pharmaceutical companies or others. There can be no assurance that insurance will be adequate or will continue to be available on terms acceptable to the Corporation. Insurance will generally not protect the Corporation against negligence.
The obligation to pay any product liability claim in excess of whatever insurance the Corporation is able to acquire, or the recall of any of its products, could have a material adverse effect on the business, financial condition and future prospects of the Corporation.
Risks Relating to the Corporation’s Intellectual Property Rights
It is difficult and costly to protect Acasti’s intellectual property rights, and Acasti cannot ensure the protection of these rights.
The Corporation's activities depend, in part, on its ability to (i) obtain and maintain patents, trade secret protection and operate without infringing the intellectual proprietary rights of third parties, (ii) successfully defend these patents (including patents owned by or licensed to the Corporation) against third-party challenges, and (iii) successfully enforce these patents against third party competitors. There is no assurance that the Corporation will be granted such patents and/or proprietary technology or that such granted patents and/or proprietary technology will not be circumvented through the adoption of a competitive, though non-infringing, process or product. The patent positions of pharmaceutical companies can be highly uncertain and involve complex legal, scientific and factual questions for which important legal principles remain unresolved. Changes in either the patent laws or in interpretations of patent laws may diminish the value of the Corporation’s intellectual property. Accordingly, the Corporation cannot predict the breadth of claims that may be allowable or enforceable in its patents (including patents owned by or licensed to the Corporation). Failure to protect the Corporation's existing and future intellectual property rights could seriously harm its business and prospects and may result in the loss of its ability to exclude others from using the Corporation's technology or its own right to use the technologies. If the Corporation does not adequately ensure the right to use certain technologies, it may have to pay others for the right to use their intellectual property, pay damages for infringement or misappropriation and/or be enjoined from using such intellectual property. The Corporation’s patents do not guarantee the right to use the technologies if other parties own intellectual property rights that are necessary in order to use such technologies. The Corporation's and Neptune’s patent position is subject to complex factual and legal issues that may give rise to uncertainty as to the validity, scope and enforceability of a particular patent.
In any case, there can be no assurance that:
|
|
·
|
any rights under Canadian, U.S. or foreign patents owned by the Corporation or other patents that Neptune and other third parties license to the Corporation will not be curtailed;
|
|
|
·
|
the Corporation was the first inventor of inventions covered by its issued patents or pending applications or that the Corporation was the first to file patent applications for such inventions;
|
|
|
·
|
the Corporation’s pending or future patent applications will be issued with the breadth of claim coverage sought by the Corporation, or be issued at all;
|
|
|
·
|
the Corporation’s competitors will not independently develop or patent technologies that are substantially equivalent or superior to the Corporation's technologies;
|
|
|
·
|
any of the Corporation's trade secrets will not be learned independently by its competitors; or
|
|
|
·
|
the steps the Corporation takes to protect its intellectual property will be adequate.
|
In addition, effective patent, trademark, copyright and trade secret protection may be unavailable, limited or not sought in certain foreign countries.
13
The Corporation also seeks to protect its proprietary intellectual property, including intellectual property that may not be patented or patentable, in part by confidentiality agreements and, if applicable, inventors' rights agreements with its strategic partners and employees. There can be no assurance that these agreements will not be breached, that the Corporation will have adequate remedies for any breach or that such persons or institutions will not assert rights to intellectual property arising out of these relationships. The cost of enforcing the Corporation's patent rights or defending rights against infringement charges by other patent holders may be significant and could limit operations. The Corporation intends to vigorously enforce and protect its intellectual property.
The degree of future protection for the Corporation’s proprietary rights is uncertain, because legal means afford only limited protection and may not adequately protect the Corporation’s rights, permit it to gain or keep its competitive advantage, or provide it with any competitive advantage at all. The Corporation cannot be certain that any patent application owned by a third party will not have priority over patent applications filed or in-licensed by the Corporation, or that the Corporation or its licensor will not be involved in interference, opposition or invalidity proceedings before U.S., Canadian or foreign patent offices.
The Corporation depends on Neptune to protect a significant portion of its proprietary rights that derive from the Corporation’s license agreement with Neptune. Neptune may be primarily or wholly responsible for the maintenance of patents and prosecution of the licensed patent applications relating to important areas of the Corporation’s business. If Neptune fails to adequately maintain, prosecute or protect these patents or patent applications, the Corporation may have the right to take further action on its own to protect its technology. However, the Corporation may not be successful or have adequate resources to do so. Any failure by Neptune or by the Corporation to protect its intellectual property rights could significantly harm the Corporation’s business and prospects.
The Corporation also relies on trade secrets to protect its technology, especially in cases when the Corporation believes patent protection is not appropriate or obtainable. However, trade secrets are difficult to protect. If the Corporation cannot maintain the confidentiality of its proprietary and licensed technology and other confidential information, the Corporation’s ability and that of its licensor to receive patent protection and its ability to protect valuable information owned or licensed by the Corporation may be imperiled. Enforcing a claim that a third-party entity illegally obtained and is using any of the Corporation’s trade secrets is expensive and time consuming, and the outcome is unpredictable. Moreover, the Corporation’s competitors may independently develop equivalent knowledge, methods and know-how. If the Corporation fails to obtain or maintain patent protection or trade secret protection for CaPre®, ONEMIA® or the Corporation’s technologies, third parties could use the Corporation’s proprietary information, which could impair its ability to compete in the market and adversely affect its ability to generate future revenues and attain profitability.
CaPre® is covered by patents that are not owned by the Corporation but are instead licensed to the Corporation by Neptune.
In addition to its proprietary patent applications, the Corporation has an exclusive worldwide license under certain patents and know-how to develop and commercialize CaPre® within a specified field of use pursuant to a license agreement with Neptune. The limitation on the Corporation’s field of use may prevent it from developing and commercializing CaPre® in other fields. Additionally, the Corporation’s license is subject to termination for breach of its terms, and therefore its rights may only be available to it for as long as Neptune agrees that the Corporation’s development and commercialization activities are sufficient to meet the terms of the license. If this license is terminated for any reason and the Corporation is not able to negotiate another agreement with Neptune for use of its patents and know-how, the Corporation will not be able to manufacture and market CaPre®, which would have a material adverse effect on its business and financial condition. See “Acasti’s Business – Intellectual Property”.
CaPre® may infringe the intellectual property rights of others, which could increase the Corporation’s costs and delay or prevent the Corporation’s development and commercialization efforts.
The Corporation’s success depends in part on avoiding infringement of the proprietary technologies of others. The pharmaceutical industry has been characterized by frequent litigation regarding patent and other intellectual property rights. Identification of third party patent rights that may be relevant to the Corporation’s proprietary or licensed technology is difficult because patent searching is imperfect due to differences in terminology among patents, incomplete databases and the difficulty in assessing the meaning of patent claims. Additionally, because patent applications are maintained in secrecy until the application is published, the Corporation may be unaware of third-party patents that may be infringed by the development and commercialization of CaPre® or any other future prescription drug candidate. There may be certain issued patents and patent applications claiming subject matter that the Corporation’s licensor or the Corporation may be required to license in order to research, develop or commercialize CaPre®, and the Corporation cannot be certain whether such patents and patent applications would be available to license on commercially reasonable terms, or at all. Any claims of patent infringement asserted by third parties would be time-consuming and may:
|
|
·
|
result in costly litigation;
|
|
|
·
|
divert the time and attention of the Corporation’s technical personnel and management;
|
14
|
|
·
|
cause product development or commercialization delays, including delays in clinical trials for CaPre®;
|
|
|
·
|
prevent the Corporation from commercializing CaPre® until the asserted patent expires or is held finally invalid or not infringed in a court of law;
|
|
|
·
|
require the Corporation to cease or modify its use of the technology and/or develop non-infringing technology; or
|
|
|
·
|
require the Corporation to enter into royalty or licensing agreements.
|
Others may hold proprietary rights that could prevent CaPre® from being marketed. Any patent-related legal action against the Corporation claiming damages and seeking to enjoin commercial activities relating to CaPre® or the Corporation’s processes could subject the Corporation to potential liability for damages and require the Corporation to obtain a license to continue to manufacture or market CaPre® or any other future prescription drug candidates. The Corporation cannot predict whether the Corporation would prevail in any such actions or that any license required under any of these patents would be made available on commercially acceptable terms, if at all. In addition, the Corporation cannot be sure that it could redesign CaPre® or any other future product candidates or processes to avoid infringement, if necessary. Accordingly, an adverse determination in a judicial or administrative proceeding, or the failure to obtain necessary licenses, could prevent the Corporation from developing and commercializing CaPre® or any other future product candidate, which could harm the Corporation’s business, financial condition and operating results.
A number of companies, including several major pharmaceutical companies, have conducted research on pharmaceutical uses of omega-3 fatty acids, which has resulted in the filing of many patent applications related to this research. The Corporation is aware of third-party U.S., Canadian or other foreign patents that contain broad claims related to methods of using these general types of compounds, which may be construed to include potential uses of CaPre® or any future product candidates. If the Corporation were to challenge the validity of these or any other issued U.S, Canadian or other foreign patents in court, the Corporation would need to overcome a statutory presumption of validity that attaches to every U.S. and Canadian patent. This means that, in order to prevail, the Corporation would have to present clear and convincing evidence as to the invalidity of the other party’s patent’s claims. If the Corporation were to challenge the validity of any issued U.S. patent in an administrative trial before the Patent Trial and Appeal Board in the USPTO, the Corporation would have to prove that the claims are unpatentable by a preponderance of the evidence. There is no assurance that a jury and/or court would find in the Corporation’s favor on questions of infringement, validity or enforceability.
General Risks Related to the Corporation
The Corporation may never become profitable or be able to sustain profitability.
The Corporation is a clinical-stage biopharmaceutical company with a limited operating history. The likelihood of success of the Corporation’s business plan must be considered in light of the problems, expenses, difficulties, complications and delays frequently encountered in connection with developing and expanding early-stage businesses and the regulatory and competitive environment in which the Corporation operates. Biopharmaceutical product development is a highly speculative undertaking, involves a substantial degree of risk and is a capital-intensive business. Therefore, the Corporation expects to incur expenses without any meaningful corresponding revenues unless and until it is able to obtain regulatory approval and subsequently sell CaPre® in significant quantities. The Corporation has been engaged in developing CaPre® since 2008. To date, the Corporation has not generated any revenue from CaPre®, and it may never be able to obtain regulatory approval for the marketing of CaPre® in any indication. Further, even if the Corporation is able to commercialize CaPre® or any other product candidate, there can be no assurance that the Corporation will generate significant revenues or ever achieve profitability. The Corporation’s net loss for the fiscal year ended February 28, 2015 was approximately $1.7 million. As of February 28, 2015, the Corporation had an accumulated deficit of approximately $33.3 million.
If the Corporation obtains FDA approval, it expects that its expenses will increase as it prepares for the commercial launch of CaPre®. The Corporation also expects that its research and development expenses will continue to increase in the event it pursues FDA approval for CaPre® for other indications. As a result, the Corporation expects to continue to incur substantial losses for the foreseeable future, and these losses may be increasing. The Corporation is uncertain about when or if it will be able to achieve or sustain profitability. If the Corporation achieves profitability in the future, it may not be able to sustain profitability in subsequent periods. Failure to become and remain profitable would impair the Corporation’s ability to sustain operations and adversely affect the price of the Common Shares and its ability to raise capital.
The Corporation may not be able to maintain its operations and research and development without additional funding.
The Corporation will require substantial additional funds to conduct further research and development, scheduled clinical testing, regulatory approvals and the commercialization of CaPre®. In addition to completing nonclinical and clinical trials, the Corporations expects that additional time and capital will be required to complete the filing of a NDA to obtain FDA approval for CaPre® in the United States and to complete marketing and other pre-commercialization activities. To date, the Corporation has financed its operations through public offering and private placement of common shares, proceeds from exercises of warrants, rights and options and research tax credits. The Corporation’s cash and short term investments were approximately $18.3 million as of February 28, 2015. Depending on the status of regulatory approval or, if approved, commercialization of CaPre®, the Corporation will most likely require additional capital to fund its operating needs. To achieve the objectives of its business plan, the Corporation plans to establish strategic alliances, raise the necessary capital and make sales. The Corporation may also seek additional funding for these purposes through public or private equity or debt financing, joint venture arrangements, and collaborative arrangements with other pharmaceutical companies, and/or from other sources.
15
The Corporation has incurred operating losses and negative cash flows from operations since inception. If the Corporation is unable to secure sufficient capital to fund its operations, it may be forced to enter into strategic collaborations that could require the Corporation to share commercial rights to CaPre® with third parties in ways that the Corporation currently does not intend or on terms that may not be favorable to the Corporation. There can be no assurance that any additional funding from any other third party will be available on acceptable terms or at all to enable the Corporation to continue and complete the research and development of CaPre®. The failure to obtain additional financing on favourable terms, or at all, could have a material adverse effect on Acasti’s business, financial condition and results of operations.
In order to establish the Corporation’s sales and marketing infrastructure, the Corporation will need to expand the size of its organization, and the Corporation may experience difficulties in managing this growth.
As of February 28, 2015, the Corporation had seven employees in Canada, six of whom have biology, chemistry, biochemistry or microbiology credentials and one administrative staff with a pharmaceutical industry background. As the Corporation’s development and commercialization plans and strategies develop, the Corporation expects that it will need to expand the size of its employee base for managerial, operational, sales, marketing, financial and other resources. Future growth would impose significant added responsibilities on members of management, including the need to identify, recruit, maintain, motivate and integrate additional employees. In addition, the Corporation’s management may have to divert a disproportionate amount of its attention away from the Corporation’s day-to-day activities and devote a substantial amount of time to managing these growth activities. The Corporation’s future financial performance and its ability to commercialize CaPre® and any other future product candidates and its ability to compete effectively will depend, in part, on the Corporation’s ability to effectively manage any future growth.
If the Corporation is not successful in attracting and retaining highly qualified personnel, the Corporation may not be able to successfully implement its business strategy.
The Corporation’s ability to compete in the highly competitive pharmaceuticals industry depends in large part upon its ability to attract and retain highly qualified managerial, scientific and medical personnel. Competition for skilled personnel in the Corporation’s market is intense and competition for experienced scientists may limit the Corporation’s ability to hire and retain highly qualified personnel on acceptable terms. The Corporation is highly dependent on its management, scientific and medical personnel. The Corporation’s management team has substantial knowledge in many different aspects of drug development and commercialization. Despite the Corporation’s efforts to retain valuable employees, members of its management, scientific and medical teams may terminate their employment with the Corporation on short notice or, potentially, without any notice at all. The loss of the services of any of the Corporation’s executive officers or other key employees could potentially harm its business, operating results or financial condition. The Corporation’s success may also depend on its ability to attract, retain and motivate highly skilled junior, mid-level, and senior managers and scientific personnel.
Other pharmaceutical companies with which the Corporation competes for qualified personnel have greater financial and other resources, different risk profiles, and a longer history in the industry than the Corporation does. They also may provide more diverse opportunities and better chances for career advancement. Some of these characteristics may be more appealing to high-quality candidates than what the Corporation has to offer. If the Corporation is unable to continue to attract and retain high-quality personnel, the rate and success at which the Corporation can develop and commercialize product candidates would be limited.
If product liability lawsuits are brought against the Corporation, it may incur substantial liabilities and may be required to cease the sale, marketing and distribution of its products.
The Corporation faces a potential risk of product liability as a result of its sales, marketing and distribution activities relating to ONEMIA® and any future commercialization of CaPre® or any other future product. For example, the Corporation may be sued if any product it develops allegedly causes injury or is found to be otherwise unsuitable during product testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability and a breach of warranties. Claims could also be asserted under U.S. state or Canadian provincial or other foreign consumer protection legislation. If the Corporation cannot successfully defend itself against product liability claims, it may incur substantial liabilities or be required to cease the sale, marketing and distribution of its products. Even successful defense against product liability claims would require significant financial and management resources. Regardless of the merits or eventual outcome, liability claims may result in:
16
|
|
·
|
decreased demand for ONEMIA®, CaPre® or any future products that the Corporation may develop;
|
|
|
·
|
injury to the Corporation’s reputation;
|
|
|
·
|
withdrawal of clinical trial participants;
|
|
|
·
|
costs to defend the related litigation;
|
|
|
·
|
a diversion of management’s time and the Corporation’s resources;
|
|
|
·
|
substantial monetary awards to consumers, trial participants or patients;
|
|
|
·
|
product recalls, withdrawals or labeling, marketing or promotional restrictions;
|
|
|
·
|
loss of revenue;
|
|
|
·
|
the inability to commercialize CaPre®;
|
|
|
·
|
the inability to continue the sale, marketing and distribution of ONEMIA®; and
|
|
|
·
|
a decline in the price of the Common Shares.
|
If the Corporation is unable to obtain and retain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims, the commercialization of products it develops could be hindered or prevented. The Corporation currently carries product liability insurance in the amount of $5.0 million in the aggregate. In addition, the Corporation currently carries liability insurance covering its clinical trials in the amount of $5.0 million in the aggregate. Although the Corporation maintains such insurance, any claim that may be brought against the Corporation could result in a court judgment or settlement in an amount that is not covered, in whole or in part, by the Corporation’s insurance or that is in excess of the limits of the Corporation’s insurance coverage. The Corporation’s insurance policies also have various exclusions, and the Corporation may be subject to a product liability claim for which it has no coverage. In the event of a successful product liability claim against it, the Corporation may have to pay from its own resources any amounts awarded by a court or negotiated in a settlement that exceed its coverage limitations or that is not covered by the Corporation’s insurance, and the Corporation may not have, or be able to obtain, sufficient capital to pay such amounts.
The Corporation may acquire businesses or products or form strategic alliances in the future and the Corporation may not realize the benefits of such acquisitions.
The Corporation may acquire additional businesses or products, form strategic alliances or create joint ventures with third parties that the Corporation believes will complement or augment its existing business. If the Corporation acquires businesses with promising markets or technologies, it may not be able to realize the benefit of acquiring such businesses if the Corporation is unable to successfully integrate them with its existing operations and company culture. The Corporation may encounter numerous difficulties in developing, manufacturing and marketing any new products resulting from a strategic alliance or acquisition that delay or prevent the Corporation from realizing their expected benefits.
The Corporation may not achieve its publicly announced milestones on time.
From time to time, the Corporation publicly announces the timing of certain events it expects to occur, such as the anticipated timing of results from its clinical trials. These statements are forward-looking and are based on the best estimate of management at the time relating to the occurrence of such events. However, the actual timing of such events may differ from what has been publicly disclosed. The timing of events such as completion of a clinical trial, discovery of a new product candidate, filing of an application to obtain regulatory approval, beginning of commercialization of certain products, or announcement of additional clinical trials for a product candidate may ultimately vary from what is publicly disclosed. For example, the Corporation cannot provide assurances that the TRIFECTA Phase II clinical trial and the PK trial in Canada will be completed on schedule or at all, that it will conduct Phase III clinical trial for CaPre®, that it will make regulatory submissions or receive regulatory approvals as planned, or that it will be able to adhere to plans for the scale-up of manufacturing and launch of any of its products. These variations in timing may occur as a result of different events, including the nature of the results obtained during a clinical trial or during a research phase, problems with a supplier or a distribution partner or any other event having the effect of delaying the publicly announced timeline. The Corporation undertakes no obligation to update or revise any forward-looking information, whether as a result of new information, future events or otherwise, except as otherwise required by law. Any variation in the timing of previously announced milestones could have a material adverse effect on the Corporation’s business plan, financial condition or operating results and the trading price of the Common Shares.
17
Neptune could lose its control of Acasti
Neptune currently owns approximately 48% of Acasti’s outstanding common shares, seven members of Neptune’s Board of Directors are also members of Acasti’s Board of Directors, and Neptune’s Chief Financial Officer is also the interim Chief Executive Officer of Acasti. As a result, Neptune exercises control over Acasti as of February 28, 2015. However, if all outstanding warrants, call options and restrictive share units of Acasti were to be exercised, Neptune’s ownership interest in Acasti’s common shares would fall to approximately 35%. If Neptune’s ownership of Acasti’s common shares declines, Neptune may lose its ability to elect members of its Board of Directors to Acasti’s Board of Directors and to otherwise exercise control over Acasti. A loss of Neptune’s control over Acasti, could, among other things result in:
|
|
·
|
investors and analysts placing a different, and possibly lower, value on the Common Shares to reflect a lower degree of exposure by Neptune to Acasti’s krill oil-based pharmaceutical business;
|
|
|
·
|
Acasti making decisions in connection with the development and commercialization of Acasti’s products with less or no involvement and approval from Neptune; and
|
|
|
·
|
a different presentation of Neptune’s financial statements as it relates to Acasti, including assets and any future revenues generated by Acasti would not be directly included in Neptune’s consolidated financial statements.
|
Neptune does not expect to provide material capital to Acasti in the short term and therefore, its ownership interest in Acasti may continue to decline.
If we fail to maintain the requirements for continued listing on NASDAQ, our common shares could be delisted from trading on NASDAQ, which would materially adversely affect the liquidity of our common shares, the price of our common shares, and our ability to raise additional capital.
Failure to meet the applicable continued listing requirements of NASDAQ could result in our common shares being delisted from NASDAQ. On November 7, 2014, we received a first notification from NASDAQ informing us that we failed to maintain a minimum closing bid price on NASDAQ of at least US$1.00 per share for our common shares for 30 consecutive business days, as we are required to do under NASDAQ Marketplace Rule 4450(a)(5) (the “Minimum Bid Price Rule”). We were given 180 days (the “Initial Compliance Period”), or until May 6, 2015, to regain compliance by having the bid price of our common shares close at $1.00 per share or more for a minimum of 10 consecutive business days prior to the end of the Initial Compliance Period. On May 11, 2015, NASDAQ granted Acasti an additional 180-day period (the “Second Compliance Period”), or until November 2, 2015, to regain compliance. As part of the conditions to receive its extension, Acasti provided NASDAQ with written notice of its intention to cure the minimum bid price deficiency during the Second Compliance Period by effecting a share consolidation, if necessary. While we may explore various actions to meet the Minimum Bid Price Rule there is no guarantee that any such action will be successful in bringing us into, or maintaining, compliance.
If we fail to satisfy Nasdaq’s continued listing requirements, our common shares could be delisted from NASDAQ, in which case we may transfer to the NASDAQ Capital Market, which generally has lower financial requirements for initial listing or, if we fail to meet its listing requirements, the over‐the‐counter bulletin board. However, there can be no assurance that our common shares will be eligible for trading on any such alternative exchanges or markets in the United States.
If we are delisted from NASDAQ it would materially reduce the liquidity of our common shares, lower the price of our common shares, and impair our ability to raise financing.
In order to comply with NASDAQ’s Minimum Bid Price Rule we may, subject to regulatory approvals (including from the TSXV), implement a share consolidation, which could require shareholder approval and adversely affect our common share price and its liquidity.
Subject to regulatory approvals (including from the TSXV), we may implement a share consolidation in order to comply with the Minimum Bid Price Rule. The exact number of shares of the Corporation to be consolidated, if at all required or necessary, would be determined by our board of directors and may be subject to shareholder approval.
While such share consolidation could bring us back into compliance with the listing requirements of NASDAQ, there can be no assurance that any increase in the market price of our common shares resulting from a share consolidation, if implemented, would be sustainable. There are numerous factors and contingencies that would affect such price, including the market conditions for our common shares at the time, our reported results of operations in future periods and general economic, geopolitical, stock market and industry conditions. Accordingly, the total market capitalization of our common shares after a share consolidation may be lower than the total market capitalization before such share consolidation and, in the future, the market price of our common shares might not exceed or remain higher than the market price prior to such share consolidation. There can be no assurance that a share consolidation would result in a per share market price that attracts institutional investors or investment funds, or that such price would satisfy the investing guidelines of institutional investors or investment funds. As a result, the trading liquidity of our common shares might not improve as a result of a share consolidation. Furthermore, the liquidity of our common shares could be adversely affected by the reduced number of our common shares that would be outstanding after the share consolidation.
18
Risks Related to the Corporation’s Status as a Foreign Private Issuer/Emerging Growth Company
As a foreign private issuer, the Corporation is subject to different U.S. securities laws and regulations than a domestic U.S. issuer, which may limit the information publicly available to the Corporation’s U.S. shareholders.
The Corporation is a foreign private issuer under applicable U.S. federal securities laws, and therefore, it is not required to comply with all the periodic disclosure and current reporting requirements of the U.S. Securities and Exchange Act of 1934, as amended (the “Exchange Act”). As a result, the Corporation does not file the same reports that a U.S. domestic issuer would file with the SEC, although the Corporation is required to file with or furnish to the SEC the continuous disclosure documents that the Corporation is required to file in Canada under Canadian securities laws. In addition, the Corporation’s officers, directors and principal shareholders are exempt from the reporting and short-swing profit recovery provisions of Section 16 of the Exchange Act. Therefore, the Corporation’s shareholders may not know on as timely a basis when the Corporation’s officers, directors and principal shareholders purchase or sell common shares as the reporting periods under the corresponding Canadian insider reporting requirements are longer. In addition, as a foreign private issuer, the Corporation is exempt from the proxy rules under the Exchange Act.
The Corporation may lose its foreign private issuer status in the future, which could result in significant additional costs and expenses to the Corporation.
The Corporation may in the future lose its foreign private issuer status if a majority of the Common Shares are held in the United States and it fails to meet the additional requirements necessary to avoid loss of foreign private issuer status. The regulatory and compliance costs to the Corporation under U.S. federal securities laws as a U.S. domestic issuer would be significantly more than the costs the Corporation incurs as a Canadian foreign private issuer. If the Corporation is not a foreign private issuer, it would not be eligible to use foreign issuer forms and would be required to file periodic and current reports and registration statements on U.S. domestic issuer forms with the SEC, which are more detailed and extensive than the forms available to a foreign private issuer. In addition, the Corporation may lose the ability to rely upon exemptions from NASDAQ corporate governance requirements that are available to foreign private issuers. If the Corporation loses foreign private issuer status, compliance with more enhanced disclosure requirements and other U.S. securities laws may increase our legal and financial compliance costs, make some activities more difficult and time-consuming, increase demand on our systems and resources and divert management’s attention from other business concerns, all of which could have a material adverse effect on our business, financial condition and results of operations.
Currently, the Corporation does not satisfy the eligibility criteria to use MJDS to conduct public securities offerings and to meet its periodic disclosure requirements in the United States. As a result, if the Company conducts future public securities offerings in the United States, it may have do so without the use of MJDS, which could involve additional time and cost.
As an “emerging growth company”, Acasti is exempt from the requirement to comply with the auditor attestation requirements of the Sarbanes-Oxley Act.
Acasti is an “emerging growth company”, as defined in the U.S. Jumpstart Our Business Start-ups Act, and intends to avail itself of the exemption provided to emerging growth companies from the auditor attestation requirements of Section 404(b) of the Sarbanes-Oxley Act of 2002. Therefore, Acasti’s internal controls over financial reporting will not receive the level of review provided by the process relating to the auditor attestation included in annual reports of issuers that are not using an exemption. In addition, Acasti cannot predict if investors will find the Common Shares less attractive because it relies on this exemption. If some investors find the Common Shares less attractive as a result, there may be a less active trading market for the Common Shares and trading price for the Common Shares may be negatively affected.
U.S. investors may be unable to enforce certain judgments.
The Corporation is a company existing under the Business Corporations Act (Québec). The majority of the Corporation’s directors and officers are residents of Canada, and substantially all of the Corporation’s assets are located outside the United States. As a result, it may be difficult to effect service within the United States upon the Corporation or upon its directors and officers. Execution by U.S. courts of any judgment obtained against the Corporation or any of its directors or officers in U.S. courts may be limited to the assets of such companies or such persons, as the case may be, located in the United States. It may also be difficult for holders of securities who reside in the United States to realize in the United States upon judgments of U.S. courts predicated upon civil liability and the civil liability of the Corporation’s directors and executive officers under the U.S. federal securities laws. The Corporation has been advised that a judgment of a U.S. court predicated solely upon civil liability under U.S. federal securities laws or the securities or “blue sky” laws of any state within the United States, would likely be enforceable in Canada if the United States court in which the judgment was obtained has a basis for jurisdiction in the matter that would be recognized by a Canadian court for the same purposes. However, there may be doubt as to the enforceability in Canada against these non-U.S. entities or their controlling persons, directors and officers who are not residents of the United States, in original actions or in actions for enforcement of judgments of U.S. courts, of liabilities predicated solely upon U.S. federal or state securities laws.
19
The Corporation has not made a determination as to whether it was a passive foreign investment company, or PFIC, for the taxable year ended February 28, 2015 or whether it will be a PFIC for the current taxable year. The PFIC classification is fundamentally factual in nature, determined annually and subject to change.
The Corporation has not made a determination as to whether it was a PFIC for the taxable year ended February 28, 2015 or whether it will be a PFIC for the current taxable year ending February 28, 2016. Whether the Corporation is a PFIC depends on complex U.S. federal income tax rules whose application to the Corporation is uncertain, and, since the PFIC status of the Corporation will depend upon the composition of its income and assets and the fair market value of its assets from time to time and generally cannot be determined until the end of a taxable year, there can be no assurance that the Corporation will not be a PFIC for the current or subsequent taxable years. If the Corporation is a PFIC or if it were to become a PFIC in future taxable years while a U.S. Holder (defined as a beneficial owner of Common Shares that, for U.S. federal income tax purposes, is (a) an individual who is a citizen or resident of the U.S., (b) a corporation, or other entity classified as a corporation for U.S. federal income tax purposes, that is created or organized in or under the laws of the U.S., any state in the U.S. or the District of Columbia, (c) an estate if the income of such estate is subject to U.S. federal income tax regardless of the source of such income, or (d) a trust if (i) such trust has validly elected to be treated as a U.S. person for U.S. federal income tax purposes or (ii) a U.S. court is able to exercise primary supervision over the administration of such trust and one or more U.S. persons have the authority to control all substantial decisions of such trust) holds Common Shares, such U.S. Holder would generally be subject to adverse U.S. federal income tax consequences, including the treatment of gain realized on the sale of Common Shares as ordinary (rather than capital gain) income, potential interest charges on those gains and certain other distributions made by the Corporation and ineligibility for the preferential tax rates on dividends paid by qualified foreign corporations generally available to certain non-corporate U.S. Holders.
Each U.S. purchaser is urged to consult its own tax advisor with respect to the U.S. federal, state, local and non-U.S. tax consequences of the acquisition, ownership, and disposition of the Common Shares as may be applicable to that purchaser’s particular circumstances.
|
Item 4.
|
Information on the Company
|
|
A.
|
History and Development of the Company
|
We were incorporated on February 1, 2002 under Part 1A of the Companies Act (Québec) under the name “9113-0310 Québec Inc”. On August 7, 2008, pursuant to a Certificate of Amendment, we changed our name to “Acasti Pharma Inc.”, our share capital, the provisions regarding the restrictions on securities transfers and the borrowing powers of the Corporation. On November 7, 2008, pursuant to a Certificate of Amendment, we further revised our provisions regarding our borrowing powers. We became a reporting issuer in the Province of Québec on November 17, 2008. On February 14, 2011, the Business Corporations Act (Québec) came into effect and replaced the Companies Act (Québec). We are now governed by the Business Corporations Act (Québec).
Our head office and registered office is located at 545 Promenade du Centropolis, Suite 100, Laval, Québec H7T 0A3, and the phone number of our head and registered office is (450) 687-2262. Our website address is http://www.acastipharma.com. We do not incorporate the information on or accessible through our website into this Annual Report, and you should not consider any information on, or that can be accessed through, our website as part of this Annual Report. Our registered agent in the United States is CT Corporation System, 111 Eighth Avenue, New York, NY 10011.
The following is a summary of significant events related to our development and our business that have occurred in the last three completed fiscal years.
Fiscal Year Ended February 28, 2013
On January 7, 2013, the Common Shares were listed for trading on the NASDAQ under the ticker symbol “ACST”.
20
On November 8, 2012, Neptune reported an explosion and fire destroyed its production plant located in Sherbrooke, Québec, Canada. Acasti announced that its day-to-day operations and business were not interrupted as a result of this tragic event and that all CaPre® materials required for its two Phase II clinical trials had already been produced and stored in other facilities outside Neptune’s affected plant. See “Risk Factors - Risks Related to Product Development, Regulatory Approval and Commercialization - The Corporation’s supply of krill oil for commercial supply and clinical trials is dependent upon relationships with Neptune and other third party manufacturers and key suppliers.”
On December 4, 2012, the Corporation announced that it entered into a prepayment agreement with Neptune pursuant to which the Corporation exercised its option to prepay all future royalties under the license granted by Neptune to Acasti. The value of the prepayment, determined with the assistance of outside valuations specialists, using the pre-established formula set forth in the license agreement, amounts to approximately $15.5 million, which Acasti will pay through the issuance of 6,750,000 Common Shares, issuable at a price of $2.30 per share, upon the exercise of a warrant delivered to Neptune. The prepayment and the issuance of the Common Shares to Neptune are subject to the final approval of the TSXV and the approval of the disinterested shareholders of the Corporation at its next annual meeting, which is scheduled to occur on June 27, 2013.
Fiscal Year Ended February 28, 2014
On March 19, 2013, the Corporation announced encouraging preliminary data of its “Randomized, Open-Label, Dose-Ranging, Multi-Center Trial to assess the Safety and efficacy of CaPre® in the treatment of mild-to-high hypertriglyceridemia”. Data from 157 patients who completed four weeks of treatment with 0.5, 1, 2 or 4 grams of CaPre® per day were assessed and CaPre® achieved a clinically important and statistically significant triglyceride reduction of up to 23% (p<0.05) as compared to standard of care. The results of this preliminary analysis suggested that CaPre® could be used as a safe and effective alternative for the treatment of patients with triglyceride levels ranging from 200 to 500 mg/dL.
On May 22, 2013, the Corporation announced that patient recruitment for the COLT trial had been completed. Acasti continued to make good progress on its two Phase II clinical trials, the COLT trial and the TRIFECTA trial.
On June 27, 2013, the Corporation held its Annual and Special Meeting of the shareholders, where the shareholders of the Corporation voted in favour of all items put forth at the meeting. All of the existing director nominees were re-elected and three new directors, Mr. Valier Boivin, Mr. Jean-Claude Debard and Mr. Harlan W. Waksal, were elected.
On July 15, 2013, the Corporation announced that it had received the approval of both the shareholders and the TSX Venture Exchange to become royalty free by paying in advance all future royalties owed under the license agreement through the issuance of shares to Neptune. The value of this royalty prepayment, which was confirmed by an independent valuation expert using the pre-established prepayment formula set forth in the license agreement, was approximately $15.5 million and was paid through the issuance of 6,750,000 Acasti Class A common shares to Neptune. The prepayment increased Neptune’s equity participation in Acasti from approximately 57% to approximately 60%. Being royalty free allows Acasti to preserve cash of at least $700,000 annually which was the current minimum royalty due under the license agreement.
On July 31, 2013, the Corporation announced that it had signed an agreement with a world leader in natural based specialty chemicals for the manufacturing of CaPre® clinical material in expectation of upcoming PK and phase III clinical trials in the United States and to substantiate its upcoming submission of an IND filing. Specialized krill oil raw material will first be produced by a North American company using Neptune’s proprietary production process. It will then be sent to the specialty chemicals manufacturer for further processing, including purification and formulation into CaPre® under cGMP guidelines. The Corporation also announced its intention to initiate discussions to manufacture CaPre® at full plant scale, should regulatory approval for commercialization in the United States be obtained
On August 13, 2013 the Corporation announced positive results for its Phase II randomized, open-label, dose-ranging, multi-center trial designed to assess the safety and efficacy of its investigational new drug candidate CaPre® in the treatment of mild to severe hypertriglyceridemia. CaPre® was found to be safe and effective with significant mean triglyceride reductions above 20% after 8 weeks of treatment with both daily doses of 4g and 2g. No serious adverse events were reported, indicating that CaPre® is safe and tolerable at all doses tested.
On October 2, 2013, the Corporation announced the conclusion of a settlement with respondents Rimfrost, resolving the ITC investigation related to infringement of Neptune’s composition of matter patents. As part of the settlement, Neptune granted a world-wide, non-exclusive, royalty-bearing licence to these settling respondents, allowing them to market and sell nutraceutical products containing components extracted from krill. The respondents in question also agreed to pay Neptune an additional royalty amount for the manufacture and sale of krill products prior to the effective license commencement date. Neptune also agreed to dismiss a related patent infringement case against Rimfrost filed in March of 2013. Moreover, Neptune signed a strategic non-exclusive krill oil manufacturing and supply agreement with Rimfrost giving Neptune the right to purchase, at a preferred price, up to 800 metric tons of krill oil during the first three-year term of the renewable agreement. Under the agreement, Neptune has agreed to purchase certain minimum quantities of commodity grade krill oil from Rimfrost in 2013 and 2014, which purchases may be deferred to the following calendar years.
21
On October 29, 2013, the Corporation announced that the USPTO had allowed Acasti’s composition and use patent application entitled Concentration Therapeutic Phospholipid Compositions, publication number US20110160161. The patent relates to concentrated therapeutic phospholipid omega-3 compositions and covers methods for treating or preventing diseases associated with cardiovascular diseases, metabolic syndrome, inflammation, neurodevelopmental diseases, and neurodegenerative diseases. The Corporation was granted a corresponding patent in South Africa, which is enforceable and valid until October 29, 2029.
On November 5, 2013, the Corporation announced that it had welcomed to its Board of Directors Reed V. Tuckson M.D., Managing Director of the health and medical care consulting business Tuckson Health Connections LLC. This appointment increased the number of board members to six, four of whom are independent directors.
On November 11, 2013, the Corporation announced the submission of an Investigational New Drug Application to the FDA to initiate a PK trial of CaPre® in the United States. This proposed PK trial is the first step in the Corporation’s U.S. clinical strategy to initiate PK and Phase III trials of CaPre® in the United States.
On November 26, 2013, the Corporation announced that it had commenced an underwritten public offering of units of the Corporation, each Unit consisting of one Common Share and one Common Share purchase warrant of the Corporation. The offering was conducted in the United States pursuant to the effective shelf registration statement filed with the U.S. Securities and Exchange Commission, or the SEC, and in Canada pursuant to a final short form base prospectus filed with the securities regulatory authorities in the Provinces of Quebec, Ontario, Manitoba, Alberta and British Columbia. On November 27, 2013, the Corporation announced that it had priced the underwritten public offering of 16,000,000 units of Acasti at a price of US$1.25 per Unit. Each of the Common Share purchase warrant entitled the holder to purchase one Common Share at exercise price of US$1.50 per warrant share. On December 3, 2013, the Corporation announced the closing of the public offering and the exercise by the underwriters, prior to the closing, of the over-allotment option which was exercised in full to purchase an additional 2,400,000 Units. The public offering resulted in a total 18,400,000 units being issued for gross proceeds of approximately US$23 million.
On December 16, 2013, the administrative law judge presiding over the pending ITC investigation involving Neptune, Acasti, Enzymotec granted the parties’ joint motion to stay the proceedings for thirty days. The motion to stay was filed because the parties had agreed to a settlement term sheet with the hope of concluding a binding settlement agreement before the expiration of the stay. Neptune has entered into a settlement agreement with all the other respondents named in the ITC investigation and motions to terminate the investigation as to those respondents have been submitted.
On December 17, 2013, the Corporation announced that it had concluded a settlement and license agreement with Aker. As part of the settlement, Neptune granted a world-wide, non-exclusive, royalty-bearing license to Aker to market and sell nutraceutical products in the licensed countries. Pursuant to the terms of the settlement, royalty levels hinge on the outcome of the review proceedings being conducted before the USPTO regarding Neptune’s 351 Patent. Aker also agreed to pay a non-refundable one-time payment to Neptune for the manufacture and sale of krill products prior to the effective USPTO decision date.
On December 19, 2013, the Corporation announced that it had appointed Jerald J. Wenker, President and COO of Dermalogica, a leading professional skin care company, as special advisor to the Board of Directors. Mr. Wenker accepted the nomination for election to serve on the Board of Directors at the Annual Meeting to be held in 2014, subject to shareholder approval.
On January 9, 2014, the Corporation announced that the FDA had cleared its Investigational New Drug submission to imitate a PK trial of CaPre® in the United States after having found no objections with the PK trial design, protocol, or safety profile of CaPre®. Following this clearance, the Corporation engaged Quintiles, the world’s largest provider of biopharmaceutical development and commercial outsourcing services, to conduct its PK study.
On February 7, 2014, the Corporation announced the closing of a private placement of CAD$2,150,000 of units of the Corporation at a price of CAD$1.33 per unit, each unit consisting of one Common Share and one Common Share purchase warrant of the Corporation. Each of these warrants entitles its holder to purchase on Common Share at an exercise price of CAD$1.60. All of the units were issued to the Fiera Capital QSSP II Investment Fund Inc. under the Quebec Stock Savings Plan II, and could not be qualified under the Quebec Stock savings Plan II and subscribed for by the Fund under the Corporation’s public offering completed on December 3, 2012.
On February 14, 2014, the Corporation announced that it had not been able to arrive at a final settlement agreement with Enzymotec that would resolve the ITC investigation into the infringement of Neptune’s composition of matter patents, and related federal court matters. Despite the presiding administrative law judge granting an extended stay through February 5, 2014, no settlement could be achieved as the parties reached an impasse on certain fundamental settlement terms, including terms that had already been agreed to in the term sheet. As a result of this bottleneck, Neptune agreed to participate in the ITC’s mediation program in a final attempt to reach a mutually satisfactory agreement. Neptune and Enzymotec requested that the administrative law judge extend the stay for an additional 60 days and reschedule the ITC hearing until after the expiration of the stay.
22
Fiscal Year Ended February 28, 2015
On April 27, 2014, Acasti and Neptune announced that a patent infringement settlement and license agreement has been signed with Enzymotec that resolves the ITC’s investigation of infringement of Neptune’s composition of matter patents, related federal court actions initiated by Neptune against Enzymotec and its distributors and various patent review proceedings requested by Enzymotec. As part of the settlement, Neptune granted a world-wide, non-exclusive, royalty-bearing license to Enzymotec, allowing it to market and sell its nutraceutical products under Neptune’s ‘348 family of patents (US Patent No. 8,030,348 and all the continuations). Under the terms of the settlement agreement, royalty levels in the United States are dependent on the outcome of pending inter partes review proceedings before the USPTO regarding certain claims of Neptune’s ‘351 composition of matter patent (US Patent No. 8,278,351). Furthermore, royalty levels in Australia are dependent on a potential request by Enzymotec to the APO for a post-grant review of certain claims of Neptune’s allowed composition of matter patent application (AU2002322233). Enzymotec also agreed to pay Neptune a non-refundable one-time upfront settlement payment.
On April 28, 2014, Acasti announced the resignation of Mr. Henri Harland as President and Chief Executive Officer of Acasti. Mr. Harland’s mandate as a Director of Acasti was terminated at the Annual Shareholders’ meeting held on June 19, 2014. Following Mr. Harland’s resignation, Acasti was managed on an interim basis by Mr. André Godin, the then Chief Financial Officer of Neptune.
On May 29, 2014, Henri Harland, the former President and Chief Executive Officer of the Corporation filed a lawsuit against the Corporation, Neptune and NeuroBioPharm in connection with his departure as President and Chief Executive Officer of each of Neptune, Acasti and NeuroBioPharm. Among other things, Mr. Harland alleged that his resignation occurred as a result of a constructive dismissal and is seeking approximately $8.5 million in damages, interest and costs. In addition, Mr. Harland is seeking from Neptune, Acasti and NeuroBioPharm, as applicable, the issuance of 500,000 shares of each of Neptune, Acasti and NeuroBioPharm as well as two blocks of 1,000,000 call options each on the shares held by Neptune in Acasti and NeuroBioPharm. As a result of the lawsuit, Mr. Harland was requested to resign as Director of the Corporation. The following day, Neptune and its subsidiaries jointly announced that they believed the claim as formulated was without merit or cause, they will vigorously defend the lawsuit and will take any steps necessary to protect their interests. On December 11, 2014 Neptune, Acasti and NeuroBioPharm filed their defence and counterclaim alleging inter alia that Mr. Harland’s contract is null and void and that he is owed nothing following his resignation. Should the Court determine that the contract is nonetheless valid, the Defendants’ position, as stated in the defence and counterclaim, is that there was also enough evidence discovered after Mr. Harland’s resignation that would have justified a dismissal for cause and that again, nothing is owed to the plaintiff. No trial date has been set. As of May 27, 2015, no agreement has been reached and an estimate of its financial effect cannot be made.
On June 16, 2014, Acasti announced the resignation of Xavier Harland as Chief Financial Officer of Acasti, whose functions were managed on an interim basis by Mr. André Godin, the then Chief Financial Officer of Neptune.
On June 20, 2014, Acasti announced changes to its board of directors following its Annual and Special Meeting held on June 19, 2014. Shareholders re-elected Dr. Ronald Denis, Valier Boivin, Dr. Reed V. Tuckson and Dr. Harlan W. Waksal. Three new directors were elected, namely Mr. Pierre Fitzgibbon, Mr. Adrian Montgomery and Mr. Jerald J. Wenker. See “Directors and Officers”.
On July 9, 2014, the Corporation announced the completion of two trials, the Phase II double-blind, placebo-controlled (TRIFECTA) study and the PK trial. Further, in September 2014, Acasti announced the successful top-line results for its TRIFECTA trial assessing the safety and efficacy of CaPre® for the treatment of patients with hypertriglyceridemia as wel as the top-line results for its PK trial evaluating the bioavailability and safety of CaPre® on healthy individuals taking single and multiple daily oral doses. See “Acasti’s Business - Clinical and Nonclinical Research - Clinical”.
On November 7, 2014 Acasti received notification from the NASDAQ Listing Qualifications Department for failing to maintain a minimum bid price of US$1.00 per share for 30 consecutive business days. This notification had no immediate effect on the listing of Acasti’s shares as the Corporation had 180 calendar days to regain compliance. On May 11, 2015, Acasti received notification from NASDAQ that it was eligible for an additional 180 calendar days to regain compliance. To regain compliance, Acasti’s shares must close at US$1.00 per share or more for a minimum of ten (10) consecutive business days. The Corporation is evaluating all available options to resolve the deficiency and regain compliance with the minimum bid price rule. See “Risk Factors - General Risks Related to the Corporation”.
23
In September 2014, Dr. Harlan W. Waksal, M.D. resigned as Executive Vice-President of the Corporation. He remains as director on the Corporation’s Board of Directors.
Recent Developments
On March 2, 2015, the Corporation announced that it had received the full data for its Phase II double blind, placebo controlled (TRIFECTA) trial which confirms and supports the positive Phase II TRIFECTA results announced in September 2014, on the safety and efficacy of CaPre® in the treatment of patients with hypertriglyceridemia. See “Acasti’s Business - Clinical and Nonclinical Research - Clinical - TRIFECTA Trial”.
On March 23, 2015, Acasti announced that the Patent Trial and Appeal Board (PTAB) of the USPTO issued a favourable decision, confirming the validity of certain claims in Neptune’s ‘351 patent (U.S. Patent: 8,278,351) and triggering royalty payments to Neptune. See “Acasti’s Business - Intellectual Property - Settlement and License Agreements”.
On March 25, 2015, Acasti announced that that the Chinese Patent Office has granted Acasti a composition and use patent. See “Acasti’s Business - Intellectual Property - Patents”.
On April 29, 2015, Acasti announced the departure of Mr. André Godin from the Corporation. Following Mr. Godin’s departure, an executive search was initiated to fulfill his functions with Acasti.
On June 1, 2015, Acasti announced the grant of an aggregate of 559,000 incentive stock options under the Corporation's Stock Option Plan for its officers and management team. Each option will vest annually over a period of three years and will entitle its holder to purchase one common share of Acasti at a price of $0.45 until June 1, 2022.
|
B.
|
Business Overview
|
Acasti is an emerging biopharmaceutical company focused on the research, development and commercialization of new krill oil-based forms of omega-3 phospholipid therapies for the treatment and prevention of certain cardiometabolic disorders, in particular abnormalities in blood lipids, also known as dyslipidemia. Krill is a major source of phospholipids and polyunsaturated fatty acids (“PUFAs”), mainly eicosapentaenoic acid (“EPA”) and docosahexaenoic acid (“DHA”), which are two types of omega-3 fatty acids well known to be beneficial for human health.
CaPre®, currently Acasti’s only prescription drug candidate, is a highly purified omega-3 phospholipid concentrate derived from krill oil and is being developed to help prevent and treat hypertriglyceridemia, which is a condition characterized by abnormally high levels of triglycerides in the bloodstream.CaPre® (predominantly EPA and DHA) is a mixture of phospholipid conjugates and free fatty acids. This form of EPA and DHA may offer better bioavailability compared to omega-3 ethyl esters (such as Lovaza®) that require additional digestive steps which may negatively affect and slow down the absorption of EPA and DHA and their transport in the bloodstream. See “Acasti’s Products - Overview”.
CaPre® is designed to be used as an adjunctive therapy with positive lifestyle changes and administered either alone or with other treatment regiments such as statins (a class of drug used to reduce cholesterol levels) and potentially for use by statin-intolerant or statin-resistant patients. CaPre® is being developed for the treatment of patients with very high triglycerides with levels over 500 mg/dL (“severe hypertriglyceridemia”) and eventually for patients with high triglycerides with levels ranging from 200 to 499 mg/dL (“mild to moderate hypertriglyceridemia”). In addition to targeting the reduction of triglyceride levels, clinical data collected and reviewed by the Corporation to date has indicated that CaPre® may also normalize blood lipids by increasing high density lipoprotein (“HDL-C”) (good cholesterol) and reducing non-high density lipoprotein (“non-HDL-C”), which includes all cholesterol contained in the bloodstream except HDL-C. In addition, clinical data collected by Acasti to date indicates that CaPre® has no significant deleterious effect on low density lipoprotein (“LDL-C”) (bad cholesterol) levels. See “Acasti’s Business - Acasti’s Products - CaPre®”.
ONEMIA®, a medical food and currently Acasti’s only commercialized product, is a purified omega-3 phospholipid concentrate derived from krill oil with lower levels of phospholipids, EPA and DHA content than CaPre®. Based on nonclinical studies conducted by Acasti, supported by clinical testing conducted on Neptune Krill Oil (NKO®), Acasti believes ONEMIA® to be safe and effective for the dietary management of omega-3 phospholipid deficiency related to abnormal lipid profiles and cardiometabolic disorders. See “Acasti’s Business - Acasti’s Products - ONEMIA®”.
24
Business Strategy
Key elements of Acasti’s strategy to commercialize therapies for dyslipidemia and other cardiometabolic disorders include: (i) completing its clinical program as per FDA recommendations and guidelines such as initiating a Phase III clinical trial and filing a New Drug Application (“NDA”) to obtain regulatory approval for CaPre® in the United States (initially for the treatment of severe hypertriglyceridemia and thereafter for the treatment of mild to moderate hypertriglyceridemia); (ii) strengthening Acasti’s patent portfolio and other means of protecting intellectual property exclusivity; (iii) pursuing distribution partnerships to commercialize CaPre® in the United States and elsewhere; and (iv) continuing to generate awareness of ONEMIA® throughout the medical community in an effort to build a market foundation for CaPre®. Acasti may also pursue strategic opportunities including licensing or similar transactions, joint ventures, partnerships, strategic alliances or alternative financing transactions to provide sources of capital for Acasti. However, no assurance can be given as to when or whether Acasti will pursue any such strategic opportunities.
Treatments for Cardiometabolic Disorders – Acasti’s Market
Lipid Disorders and Cardiovascular Disease
Heart attacks, strokes and other cardiovascular events represent the leading cause of death and disability among men and women in the United States. According to the 2011 At-A-Glance Report from the U.S. Center for Disease Control, more than 1 out of every 3 adults in the United States (approximately 83 million) currently lives with one or more types of cardiovascular disease; an estimated 935,000 heart attacks and 795,000 strokes occur in the United States each year; and an estimated 71 million adults in the United States have high cholesterol (i.e., high levels of LDL-C). Having abnormally high levels of lipids or lipoproteins, such as cholesterol and triglycerides, which are fats carried in the bloodstream, is an important risk factor for cardiovascular disease.
According to the American Heart Association, the prevalence of hypertriglyceridemia is increasing in the United States and globally, correlating to the increasing incidence of obesity and diabetes. Market participants, including the American Heart Association, have estimated that one-third of the population in the United States has elevated levels of triglycerides, including over 40 million people diagnosed with mild to moderate hypertriglyceridemia and over 4 million people diagnosed with severe hypertriglyceridemia. According to The American Heart Association Scientific Statement on Triglycerides and Cardiovascular Disease (2011), triglyceride levels provide important information as a marker associated with the risk for heart disease and stroke, especially when an individual also has low HDL-C and elevated levels of LDL-C. Lowering triglyceride levels is one of the primary goals to reduce a patient’s risk of atherosclerotic cardiovascular disease. Hypertriglyceridemia is due to both genetic and environmental factors, including obesity, sedentary lifestyle and high-calorie diets. Hypertriglyceridemia is also associated with comorbid conditions such as chronic renal failure, pancreatitis, nephrotic syndrome and diabetes.
Patients with type 2 diabetes are more susceptible to cardiovascular disease. Cardiovascular disease may be preventable in some patients with appropriate treatment of lipid abnormalities. Diabetic dyslipidemia most commonly manifests as elevated triglycerides and low levels of HDL-C, with a predominance of small, dense LDL-C particles amid relatively normal LDL-C levels. Non-HDL-C reduction is a key secondary goal of therapy under the National Cholesterol Education Program Adult Treatment Panel III national lipid treatment guidelines and, according to the American Diabetes Association and the American College of Cardiology, has been emphasized as a major goal of therapy in the consensus guidelines for lipoprotein management in patients with cardiometabolic risk. Acasti believes, based in part on a study published by Blaha MJ et al. in The Journal of Clinical Lipidology in 2008, that non-HDL-C levels may be a better indicator than LDL-C for the prediction of cardiovascular events and that non-HDL-C reduction has many other compelling advantages over LDL-C and other traditional lipid parameters. Studies have established the clinical utility of non-HDL-C as a comprehensive measure of atherogenic lipoproteins. In diabetic patients, non-HDL-C levels may be a stronger predictor of cardiovascular disease than LDL-C levels or triglycerides because it correlates highly with atherogenic lipoproteins. Target goals for LDL-C levels and non-HDL-C levels in patients with diabetes are < 100 and < 130 mg/dL, respectively. Failure to consider the importance of non-HDL-C in type 2 diabetes may result in undertreatment of patients with diabetes.
Red blood cells are made of a molecule called haemoglobin that glucose adheres to in the bloodstream. The more glucose in the blood, the more it will adhere to haemoglobin to make a glycosylated haemoglobin molecule, called haemoglobin A1C (or HbA1c). HbA1c is measured primarily to identify the average plasma glucose concentration over prolonged periods of time. This serves as a marker for average blood glucose levels over the previous months prior to the measurement.
A National Health and Nutrition Examination Survey analysis of dyslipidemia in the United States in 2010 indicated that while LDL-C levels have actually declined since its last analysis, the percentage of patients with hypertriglyceridemia has risen by 6% along with the dramatic increases in obesity. The National Cholesterol Education Program (“NCEP”) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol recommends that the first priority for the management of hypertriglyceridemia is triglyceride reduction to decrease the risk of pancreatitis. In addition, severe hypertriglyceridemia is also associated with a markedly increased risk for cardiovascular disease and a recent report released by the NCEP Expert Panel has claimed that elevated triglyceride levels can be regarded as an independent risk factor for cardiovascular disease-related events such as myocardial infarction, ischemic heart disease and ischemic stroke.
25
In a subgroup analysis of the Japan EPA Lipid Intervention Study, in 2005, in which 18,645 hypercholesterolemic patients randomly received EPA plus a statin or statin control, patients with baseline triglycerides >150 mg/dL and HDL-C <40 mg/dL receiving EPA plus a statin (7,503 patients) had a 19% reduced risk of cardiovascular disease compared to a statin alone (7,478 patients; P=0.048). In addition, in 2001, the Italian Group for the Study of the Survival of Myocardial Infarction (GISSI) trial randomly assigned 11,324 survivors of recent myocardial infarction to receive omega-3 PUFAs (1 gram per day), vitamin E (300 mg per day), both, or neither (the control group) for 3.5 years. Among the patients who received omega-3 PUFAs alone, as compared to the control group, there was a 15% reduction in the composite primary end point of death, nonfatal myocardial infarction, or nonfatal stroke (p<0.02) and a 20% reduction in the rate of death from any cause (p<0.01). The reduction in risk of sudden death was statistically significant beginning at the four month stage of treatment. A similarly significant, although more delayed, pattern after six to eight months of treatment was observed for cardiovascular, cardiac and coronary deaths.
A meta-analysis by Sarwar et al. in 2007 included 29 prospective studies and was the largest and most comprehensive epidemiological assessment of the association between triglyceride levels and cardiovascular disease risk in Western populations (262,525 participants; 10,158 cases). A combined analysis of the 29 studies yielded an adjusted odds ratio of 1.72 (72% higher risk) for the patients with triglyceride levels greater than or equal to 200 mg/dL compared to those with normal triglyceride levels. The conclusion of the study is that there are moderately strong associations between triglyceride levels and cardiovascular disease risk. In addition, there are two outcome trials ongoing (REDUCE-IT and STRENGTH) designed to evaluate long-term benefit of lowering triglycerides with prescription omega-3 fatty acids on cardiovascular risks.
Several omega-3 fatty acid products derived from fish oil are currently being marketed and sold in the United States and elsewhere. Some consist of supplements that are commercialized for human health maintenance while others are prescription omega-3 fatty acids that are designed as treatments for severe hypertriglyceridemia.
Available Prescription Drugs
The rise in obesity over the last 20 years has led to a parallel increase in triglyceride levels among the population and awareness of medical and health practitioners about the critical role that high triglyceride levels, particularly together with abnormal levels of LDL-C, HDL-C and non HDL-C (which is collectively referred to as dyslipidemia), have as a predictor of cardiovascular events. Accordingly, the introduction of new prescription drugs and drug therapies to lower the risk of cardiovascular events by addressing dyslipidemia has become a priority. The initial treatment recommendation for patients with dyslipidemia is typically a lifestyle change (diet and increased exercise). Dyslipidemia is also treated with statins, which account for a large portion of prescriptions for dyslipidemia. However, statins alone are primarily used for reducing LDL-C and appear to have only modest effects on triglyceride levels. Recognizing that statins alone are not effective triglyceride lowering drugs, the NCEP panel recommends the use of more focused therapies to lower triglyceride levels in patients with severe hypertriglyceridemia. The first-line drug therapy in patients with severe hypertriglyceridemia is often a prescription omega-3 fatty acid or fibrates, but clinical tests have shown that fibrates may also induce side effects.
According to an investigation published by the American Medical Association in 2009, fewer than 4% of adults in the United States with hypertriglyceridemia receive prescription medication to lower their triglyceride levels, representing a significant unmet medical need. Many available treatment options have limitations in the treatment of hypertriglyceridemia which Acasti believes CaPre® can address. The use of fibrates, for example, has been shown to raise the risk of abnormal increases in liver enzymes and creatinine (a marker of kidney function) and, when combined with a statin, rhabdomyolysis (muscle breakdown). Based on the results of the COLT trial and other data collected by the Corporation, the Corporation does not believe that CaPre® produces such side effects. Furthermore, Acasti believes that CaPre® in combination with statins could become a standard of care in patients with mixed dyslipidemia because of its once per day dosing convenience. See “Acasti’s Business - Clinical and Nonclinical Research - Clinical - COLT Trial”.
There are several marketed prescription omega-3 fatty acids (such as Lovaza, Vascepa, Epanova, Omtryg and some generic of Lovaza) currently approved for treatment of dyslipidemia in the United States (in severe hypertriglyceridemia) and elsewhere. According to the Frost Sullivan 2012 Global Overview of the EPA and DHA Omega-3 Ingredients Markets, the global revenue for the marine and algae EPA/DHA omega-3 ingredients market in 2011 was approximately $1.8 billion. Lovaza and Omacor, which are sold in the United States and Europe, respectively, are omega-3 ethyl-esters derived from fish oil comprised of EPA and DHA and are indicated for the treatment of severe hypertriglyceridemia in twice-daily doses of two 1-gram capsules or once-a-day dose of four 1-gram capsules. In addition, Vascepa and Epadel are two approved omega-3 ethyl-esters derived from fish oil comprised of EPA that are sold in the United States and Japan, respectively. A market research report published by Amadee & Company Inc. estimates that the total prescription omega-3 market generated over $2 billion in sales worldwide in 2012. Acasti believes that there will be increased growth in the prescription omega-3 market based on the expected introduction, and resulting increased promotion and awareness, of new prescription omega-3 products, as well as the emergence of new clinical data regarding the efficacy of omega-3s in the treatment and prevention of cardiometabolic disorders. Other disorders that potentially benefit from the use of prescription omega 3 fatty acids include osteopenia/osteoporosis, depression, sleep disorders associated with depression and pain and inflammation.
26
The cardioprotective efficacy of omega-3 fatty acids is well-established. Omega-3 products have anti-thrombotic and anti-inflammatory effects that have proven to inhibit atherosclerosis in animal models as well as reduce the rate of adverse cardiovascular events in humans. Omega-3 fatty acids, particularly those with concentrated levels of EPA and DHA, have been demonstrated in multiple clinical trials to lower concentrations of triglycerides and non-HDL in the bloodstream. In a study published in the American Journal of Clinical Nutrition in 2009, it was proposed that the omega-3 index be considered a potential risk factor for coronary heart disease mortality, especially sudden cardiac death.
Medical Foods
Medical foods are at the intersection of functional food and prescription drugs. Medical foods are regulated by the FDA and intended for specific dietary management of a disease with “distinctive nutritional requirements” under the supervision of a physician and contain ingredients that are generally recognized as safe (“GRAS”) or are otherwise considered acceptable for use. No market pre-authorization by the FDA or other similar international agencies is needed for medical foods to be commercialized in the United States or elsewhere.
The majority of U.S. medical food products on the market are for metabolic diseases. Protein-based medical foods are the most common. Nutrients such as omega-3s, isoflavones, vitamin D, chelated zinc, flavonoids (e.g., baicalin, catechin, pterostilbene), chromium picolinate, phytosterols and L-arginine are other leading ingredients used in this developing category, along with other vitamins and minerals such as pyridoxine, thiamine and folic acid, which are being used in combination. Acasti believes ONEMIA® is the only medical food that offers a high concentration of krill oil-derived omega-3 fatty acids.
Manufacturers are bringing more medical foods to market that address metabolic processes. In 2006, Limbrel (flavocoxid), the first medical food for the management of osteoarthritis, was launched. Axona was designated by the FDA in 2009 as a medical food, targeting metabolic deficiencies associated with Alzheimer’s disease; the well-researched VSL #3, a probiotic for ulcerative colitis and the ileal pouch, was introduced to the market in 2002; and NiteBite, a snack bar for the nutritional management of hyperglycemia, has been marketed since 1996.
Acasti’s Products
Overview
Acasti believes its krill oil-based form of omega-3 phospholipid therapies have advantages over omega-3 products that are derived from fish oil. EPA and DHA in krill oil are mainly carried by phospholipids, while EPA and DHA derived from fish oil are mainly carried by triglycerides. Acasti believes that omega-3 phospholipids provide for better absorption and assimilation of EPA and DHA into the bloodstream compared to some other omega-3 sources, including those derived from fish oil. CaPre® (predominantly EPA and DHA) is a mixture of phospholipid conjugates and free fatty acids. Except for Epanova® that is a mixture of EPA and DHA as FFA, all the other products are ethyl esters of EPA with or without DHA (“OM3:EE”). Because OM3:EE requires an additional de-esterification step during digestion by the carboxyl ester lipase, their bioavailability is negatively affected when compared to EPA and DHA conjugated to phospholipids or triglycerides
Once in the bloodstream, the target destinations for krill oil-based phospholipids also differ from fish oil-based omega-3 triglycerides. In addition, absorption of ethyl-ester forms of currently available prescription omega-3 fatty acids derived from fish oil requires the breakdown of fats by pancreatic enzymes that are produced in response to the consumption of high fat meals. As a low fat diet is typically a critical component for treatment of patients with severe hypertriglyceridemia, these ethyl-ester formulations have demonstrated lower absorption and bioavailability relative to those formulated as omega-3 phospholipids.
CaPre®
CaPre® is designed to be used as an adjunctive therapy with positive lifestyle changes and administered either alone or with other treatment regiments such as statins (a class of drug used to reduce cholesterol levels) and potentially for use by statin-intolerant or statin-resistant patients. CaPre® is being developed for the treatment of severe hypertriglyceridemia and eventually mild to moderate hypertriglyceridemia. In addition to targeting the reduction of triglyceride levels, clinical data collected by Acasti to date has indicated that CaPre® may also normalize blood lipids by increasing HDL-C (good cholesterol) and reducing non-HDL-C, which includes all cholesterol contained in the bloodstream except HDL-C. In addition, clinical data collected and reviewed by Acasti to date indicates that CaPre® has no significant deleterious effect on LDL-C (bad cholesterol) levels. Obtaining regulatory approval for the commercialization of CaPre® requires that safety is confirmed and it is effective at reducing triglycerides at a level that would medically benefit the patient. See “Acasti’s Business - Clinical and Nonclinical Research”.
27
ONEMIA®
ONEMIA®, a medical food and currently Acasti’s only commercialized product, is a purified omega-3 phospholipids concentrate derived from krill oil with lower levels of phospholipids, EPA and DHA content than CaPre®. The term “medical food” is defined in the United States Orphan Drug Act as a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation. Nonclinical studies conducted by the Corporation, supported by clinical testing conducted on Neptune Krill Oil (NKO®), have shown ONEMIA® to be safe and effective for the dietary management of omega-3 phospholipids deficiency and the related abnormal lipid profiles and cardiometabolic disorders. Phospholipid deficiency and abnormal lipid profiles can lead to a number of conditions, including hyperlipidemia (which generally manifests as high LDL-C and high triglycerides), atherosclerosis (the build-up of plaque on the inside of blood vessels), diabetes, rheumatoid arthritis, certain gastroenterology disorders and metabolic syndrome.
ONEMIA® was introduced in the U.S. market in 2011. In 2012, Acasti made its first sales of ONEMIA® to a medical food distributor in the United States, which has begun distribution of ONEMIA® through its network of dispensing physicians under its own brand name. ONEMIA® is also available behind-the-counter in some pharmacies. Acasti expects continued sales of ONEMIA® in the short-term to provide revenues that will contribute, in part, to the financing of Acasti’s research and development projects while continuing to generate awareness of ONEMIA® throughout the medical community in an effort to build a market foundation for CaPre®. During the fiscal years 2015, 2014 and 2013, Acasti generated revenues of approximately $271,000, $501,000 and $724,000, respectively, from sales of ONEMIA®.
Acasti continues to explore the benefit of combining ONEMIA® with a statin treatment. Nonclinical activities have been undertaken in order to determine whether or not ONEMIA® should be added to a statin treatment. The accumulated nonclinical data showed that it would be beneficial to explore in humans testing the positive results which were observed in animal testing to the effect that ONEMIA® may benefit patients taking statins dealing with complex and hard to manage lipid profiles.
Clinical and Nonclinical Research
Nonclinical
In preparation of its planned amendment of its Investigational New Drug (“IND”) application with the FDA to conduct a Phase III clinical trial and for its New Drug Application (“NDA”), Acasti carried out an extensive nonclinical program to demonstrate the safety of CaPre® in a defined set of studies required by the FDA. These studies were carried out by contract research organizations with Good Laboratory Practice certification and conducted on various species of animals recommended by the FDA to investigate the long term effects of CaPre® at doses of up to 10g HED over 13 weeks. In these studies, hematological, biochemical, coagulation and overall health parameters of CaPre® were evaluated and no toxic effects were observed in any of the segments of the studies. Once overall systemic toxicity was ruled out, Acasti’s studies focused on the potential toxic effects of CaPre® on vital systems, such as the cardiovascular, respiratory and central nervous system as evaluated by behavioural studies of the various species. These studies demonstrated that CaPre® did not have any adverse or toxic effects on any of the vital systems investigated, again up to doses well above the recommended clinical dose of CaPre®. To rule out any short term toxic effects of CaPre® on genes, genomic toxicity studies were undertaken on accepted cellular and animal models. These studies showed no toxic effects of CaPre® on any of the genetic markers indicative of potential gene altering toxic effects.
Acasti believes these studies clearly indicate that CaPre® was well-tolerated and showed no toxic effects on any of the physiological and vital systems of the tested animal subjects or their genes or molecules at doses well above the anticipated clinical therapeutic dose of 1.0g-4.0g daily.
Acasti is continuing its nonclinical studies to further investigate the potential therapeutic effects of CaPre® and ONEMIA® in the management of lipid disorders, in particular by studying their effects on the regulation of genes known to be implicated in the pathogenesis of atherosclerosis and lipid management. In parallel to its proposed Phase III clinical trial, Acasti intends to complete three sets of nonclinical studies.
28
The first set of studies, the developmental and reproductive toxicology (“Dart”), is designed to assess safety on male and female fertility, developmental toxicity (embryo-fetal development) and pre and postnatal development in rodents and non-rodents. The second set of studies, the CARCINO, will consist of carcinogenicity testing in both rats and mice to identify a tumorigenic potential in animals and to assess the relevant risk in humans. Carcinogenicity testing is usually required under the rules of the FDA prior to commercialization. Acasti believes that it will be necessary to complete the DART and CARCINO nonclinical studies prior to the filing of its NDA submission for CaPre® in the United States and expects to do so in the allocated time frame. The third set of studies, the long term animal toxicity studies, as defined by six month rodent and nine month non-rodent, will be conducted as a requirement to support clinical trials to be done during the same extent of time or to support NDA. In these studies, we investigate the effects of CaPre® on blood parameters (hematology, biochemistry, coagulation), urinanalysis, opthamological and ECG testing.
Clinical
The Phase II COLT and TRIFECTA clinical trials were initiated during the Corporation’s fiscal year ended February 29, 2012 under Canada’s Natural Health Product Directorate (“NHPD”) guidelines. The open-label COLT trial was completed during the second quarter of the 2014 fiscal year and the double-blind TRIFECTA trial was completed in the second quarter of fiscal 2015. Based on the positive results of the COLT trial, Acasti filed an IND submission with the FDA to conduct a pharmacokinetic (“PK”) study in the U.S. Acasti subsequently received approval to conduct the PK trial which was completed in the second quarter of fiscal 2015.
The COLT and TRIFECTA trials were conducted, by JSS Medical Research (“JSS”), a clinical research organization (“CRO”) specializing in the pharmaceutical, biotechnology, nutraceutical and medical device industries, which is both owned and managed by Dr. John Sampalis, brother of Dr. Tina Sampalis, previously President and Chief Global Strategy Officer of Acasti. JSS was selected by Acasti following a rigorous due diligence process conducted by the Corporation. Acasti’s board of directors appointed an external independent auditor, SNC Lavalin Pharma, to confirm and validate the clinical trials’ achievements, milestones and payments.
COLT Trial
The COLT trial, a randomized, open-label, dose-ranging, multi-center trial, was designed to assess the safety and efficacy of CaPre® in the treatment of patients with triglycerides levels between 2.28 and 10.0 mmol/L (200-877 mg/dL) (clinical trial.gov identifier NCT01516151). The primary objectives of the COLT trial were to evaluate the safety and efficacy of 0.5, 1.0, 2.0 and 4.0g of CaPre® per day in reducing fasting plasma triglycerides over 4 and 8 weeks as compared to the standard of care alone.
The secondary objectives of the COLT trial were to evaluate the effect of CaPre® on fasting plasma triglycerides in patients with triglycerides between 2.28 and 5.69 mmol/L (200-499 mg/dL) (mild to moderate hypertriglyceridemia); to evaluate the dose dependent effect on fasting plasma triglycerides in patients with triglycerides > 5.7 and <10 mmol/L (500-877 mg/dL); and to evaluate the effect of CaPre® on fasting plasma levels of LDL-C (direct measurement), HDL-C, non-HDL-C, hs-CRP and omega-3 index. Non-HDL-C is the total cholesterol minus the HDL-C.
The final results of the COLT trial indicated that CaPre® was safe and effective in reducing triglycerides in patients with mild to severe hypertriglyceridemia with significant mean (average) triglyceride reductions above 20% after 8 weeks of treatment with both daily doses of 4.0g and 2.0g. Demographics and baseline characteristics of the patient population were balanced in terms of age, race and gender. A total of 288 patients were enrolled and randomized and 270 patients completed the study, which exceeded the targeted number of evaluable patients. From this patient population, approximately 90% had mild to moderate hypertriglyceridemia.
CaPre® was safe and well tolerated. The proportion of patients treated with CaPre® that experienced one or more adverse events in the COLT trial was similar to that of the standard of care group (30.0% versus 34.5%, respectively). A substantial majority of adverse events were mild (82.3%) and no severe treatment-related adverse effects have been reported. Only one patient was discontinued from the study due to an adverse event of moderate intensity. It was noted that the rate of gastrointestinal side effects were higher in the CaPre® groups compared to standard of care alone and appeared to increase in a dose-related manner. However, none of the subjects participating in the study suffered from a serious adverse event. The report concludes that even at higher doses, CaPre® is safe and well tolerated with only transient and predominantly mild adverse events occurring at low rates.
The COLT trial met its primary objective showing CaPre® to be safe and effective in reducing triglycerides in patients with mild to severe hypertriglyceridemia. After only a 4-week treatment, CaPre® achieved a statistically significant triglyceride reduction as compared to standard of care alone. Standard of care could be any treatment physicians considered appropriate in a real-life clinical setting and included lifestyle modifications as well as lipid modifying agents, such as statins, ezetimibe and fibrates. Patients treated with 4.0g of CaPre® a day over 4 weeks reached a mean triglyceride decrease of 15.4% from baseline and a mean improvement of 18.0% over the standard of care. Results also showed increased benefits after 8 weeks of treatment, with patients on a daily dose of 4.0g of CaPre® registering a mean triglyceride decrease of 21.6% from baseline and a mean improvement of 14.4% over the standard of care. It is noteworthy that a mean triglyceride reduction of 7.1% was observed for the standard of care group at week 8, which may be explained by lipid lowering medication adjustments during the study, which was allowed to be administered in the standard of care group alone.
29
Moreover, after 8 weeks of treatment, patients treated with 1.0g for the first 4 weeks of treatment and 2.0g for the following 4 weeks, showed a statistically significant triglycerides mean improvement of 16.2% over the standard of care, corresponding to a 23.3% reduction for the 1.0-2.0g as compared to a 7.1% reduction for the standard of care. After a 8 week treatment, patients treated with 2.0g of CaPre® for the entire 8 weeks showed statistically significant triglycerides mean improvements of 14.8% over the standard of care, corresponding to a 22.0% reduction for the 2.0g as compared to a 7.1% reduction for the standard of care. Also, after 8 weeks of treatment, patients treated with 4.0g for the entire 8 weeks, showed statistically significant triglycerides, non-HDL-C and HbA1C mean improvements of, respectively, 14.4% and 9.8% and 15.0% as compared to standard of care. The 4.0g group mean improvements in (i) triglycerides of 14.4% corresponds to a reduction of 21.6% as compared to a reduction of a 7.1% for the standard of care group, (ii) non-HDL-C of 9.8% corresponds to a reduction of 12.0% as compared to a reduction of 2.3% for the standard of care group, and (iii) HbA1C of 15.0% corresponds to a reduction of 3.5% as compared to an increase of 11.5% for the standard of care group. In addition, all combined doses of CaPre® showed a statistically significant treatment effect on HDL-C levels, with an increase of 7.4% as compared to standard of care. Trends (p-value < 0.1) were also noted on patients treated with 4.0g of CaPre® for the entire 8-week treatment period with mean reduction of total cholesterol of 7.0% and increase of HDL-C levels of 7.7% as compared to the standard of care. Furthermore, after doubling the daily dosage of CaPre® after an initial period of 4 weeks, the results indicate a dose response relationship corresponding to a maintained and improved efficacy of CaPre® after an 8-week period. The efficacy of CaPre® at all doses in reducing triglyceride levels and increased effect with dose escalation suggests that CaPre® may be titrable, allowing physicians to adjust dosage in order to better manage patients’ medical needs. In addition, the results of the COLT trial indicate that CaPre® has no significant deleterious effect on LDL-C (bad cholesterol) levels.
Acasti presented the results of the COLT trial at two scientific forums, the National Lipid Association Scientific Session in Orlando in May 2014, and the 82nd Congress of European Atherosclerosis Society in Madrid in June 2014. Acasti also presented at the World Congress of Heart Disease in Boston in July 2014.
TRIFECTA Trial
The TRIFECTA trial (clinical trial gov identifier NCT01455844), a 12-week, randomized, placebo-controlled, double-blind, dose-ranging trial, is designed to assess the safety and efficacy of CaPre®, at a dose of 1.0 or 2.0g, on fasting plasma triglycerides as compared to a placebo in patients with mild to severe hypertriglyceridemia. A total of 387 patients were randomized and 365 patients completed the 12-week study, in line with the targeted number of evaluable patients. From this patient population, approximately 90% had mild to moderate hypertriglyceridemia with baseline triglycerides between 200 and 499 mg/dL (2.28 to 5.69 mmol/L). The remainder had very high baseline triglycerides between 500 and 877 mg/dL (> 5.7 and < 10 mmol/L). Approximately 30% of patients were on lipid lowering medications, such as statins, and approximately 10% were diabetic.
Similar to the COLT trial, the primary objective of the TRIFECTA trial is to evaluate the effect of CaPre® on fasting plasma triglycerides in patients with triglycerides between 2.28 and 10.0 mmol/L (200-877 mg/dL) and to assess the tolerability and safety of CaPre®. The secondary objectives of the TRIFECTA trial are to evaluate the effect of CaPre® on fasting plasma triglycerides in patients with triglycerides between 2.28 and 5.69 mmol/L (200-499 mg/dL); to evaluate the dose dependent effect on fasting plasma triglycerides in patients with triglycerides > 5.7 and <10 mmol/L (500-877 mg/dL); to evaluate the effect of CaPre® in patients with mild to moderate hypertriglyceridemia and severe hypertriglyceridemia on fasting plasma levels of LDL-C (direct measurement), and on fasting plasma levels of HDL-C, non-HDL-C, hs-CRP and omega-3 index.
On September 29, 2014, Acasti announced successful top-line results for its Phase II double blind, placebo controlled trial (TRIFECTA) assessing the safety and efficacy of CaPre® for the treatment of patients with hypertriglyceridemia. CaPre®, Acasti’s investigational new drug candidate, is composed of a patent-protected highly concentrated novel omega-3 phospholipid for the prevention and treatment of certain cardiometabolic disorders.
CaPre® successfully met the trial’s primary endpoint achieving a statistically significant (p < 0.001) mean placebo-adjusted decrease in triglycerides from baseline to week-12, with reductions of 36.4% for 1 gram and 38.6% for 2 grams.
Along with material triglyceride reductions, all key secondary endpoints were met. This is a notable achievement as the trial was not designed to show a statistical significance on any other lipid than triglycerides. Nevertheless, there was a statistically significant decrease in non-HDL-C versus placebo (p=0.038), with the 2 gram per day CaPre® group decreasing by 5.3% from baseline versus placebo over the 12-week period. Non-HDL is considered the most accurate risk marker for cardiovascular disease.
CaPre® was also shown to have a slight increase in HDL-C (good cholesterol) at both the 1 gram and 2 gram levels and decrease in LDL-C (bad cholesterol) at 2 grams. As well, there was a clinically meaningful mean placebo-adjusted reduction in VLDL-C of 10.9% and 13.5% at 1 gram and 2 gram daily doses of CaPre®, respectively. VLDL-C is considered a highly significant predictor of coronary artery disease.
30
Finally, a statistically significant dose response increase in the Omega-3 Index for patients on 1 gram and 2 grams of CaPre® versus placebo was noted. The Omega-3 Index reflects the percentage of EPA and DHA in red blood cell fatty acids. The risk of cardiovascular disease is considered to be lower as the Omega-3 Index increases.
CaPre® was found to be safe and well tolerated at all doses tested, with no serious adverse events that were considered treatment related. Out of 387 randomized patients, a total of 7 (1.8%) were discontinued as a result of adverse events, three were on placebo, two were on 1 gram of CaPre® and two were on 2 grams of CaPre®. The predominant incidence was gastrointestinal related, with no difference between CaPre® and placebo. The safety profiles of patients on CaPre® and placebo were similar.
On March 2, 2015, the Corporation announced that it had received the full data for its Phase II double blind, placebo controlled (TRIFECTA) trial which confirms and supports the positive Phase II TRIFECTA results announced in September 2014, on the safety and efficacy of CaPre® in the treatment of patients with hypertriglyceridemia. The TRIFECTA trial’s primary endpoint was met, with patients on 1 gram or 2 grams of CaPre® achieving a statistically significant mean placebo-adjusted decrease in triglycerides from baseline. In addition, benefits in other key cholesterol markers were announced, including slight increases in HDL-C (good cholesterol), no deleterious effect on LDL-C (bad cholesterol) and no safety concerns.
PK Trial
On November 11, 2013, the Corporation announced that it submitted an investigational new drug application to the FDA to initiate a PK trial of CaPre® in the United States. The PK trial was an open-label, randomized, multiple-dose, single-center, parallel-design study to evaluate blood profiles and bioavailability of omega-3 phospholipids on healthy volunteers taking single and multiple daily oral doses of 1.0g, 2.0g and 4.0g of CaPre®.
On January 9, 2014, the Corporation announced that the FDA granted Acasti approval to conduct its PK trial, having found no objections with the proposed PK trial design, protocol or safety profile of CaPre®. Acasti also announced that Quintiles, the world’s largest provider of biopharmaceutical development and commercial outsourcing services, has been hired to conduct the PK trial. On July 9, 2014, Acasti announced the completion of the PK trial.
On September 30, 2014, Acasti announced top-line results for its PK trial. The PK trial was an open-label, randomized, multiple-dose, single-center, parallel-design study in healthy volunteers. Forty-two male and female individuals, at least 18 years of age, were enrolled into three groups of 14 subjects who took 1, 2 or 4 grams of CaPre®, administered once a day 30 minutes after breakfast. The objectives of the study were to determine the pharmacokinetic profile and safety on Day 1 following a single oral dose and Day 14 following multiple oral doses of CaPre® on individuals pursuing a low-fat diet (therapeutic lifestyle changes diet). The effect of a high-fat meal on the bioavailability of CaPre® was also evaluated at Day 15. Blood samples were collected for assessment of EPA and DHA total lipids in plasma to derive the pharmacokinetic parameters.
CaPre® pharmacokinetics results appeared to be approximately dose proportional over the 1 to 4 gram a day dose range. Following a single daily dose, CaPre® reached steady state (EPA and DHA levels plateaued) within seven days of dosing. The bioavailability of CaPre® did not appear to be meaningfully affected by the fat content of the meal consumed prior to dose administration.
CaPre® was found to be safe and well tolerated at all doses tested, with all subjects completing the study. Three adverse events were reported and considered relating to CaPre®, all of which were mild. Full data and final clinical study report (“CSR”) is expected to come out by the end of fiscal 2015.
Next Steps
Acasti is now corresponding with the FDA to determine next steps in the clinical development of CaPre®, and obtain the required authorizations to proceed with such steps, including initiating a phase III clinical trial. Such correspondence is meant to allow the FDA to provide feedback on Acasti’s submissions and to answer specific questions on such submissions. Prior to a final response from the FDA, any exchange with them can take the form of written correspondence, discussions and potentially face-to-face meetings.
Acasti intends to conduct a phase III clinical trial in the United States, with potentially a few Canadian clinical trial sites, in a patient population with very high triglycerides (>500 mg/dL). This study would constitute the primary basis of an efficacy claim for CaPre® in an NDA submission for severe hypertriglyceridemia. Acasti is also evaluating the possibility of submitting a Special Protocol Assessment (“SPA”) to the FDA in order to form the basis for the design of its intended Phase III clinical trial. An SPA is a declaration from the FDA that the Phase III protocol trial design, clinical endpoints, and statistical analyses are acceptable to support regulatory approval. A request would be submitted for the protocol at least 90 days prior to the anticipated start of the Phase III clinical trial. See “Acasti’s Business - Government Regulation”.
31
In addition to conducting a Phase III clinical trial, Acasti expects that additional time and capital will be required to complete the filing of a NDA to obtain FDA approval for CaPre® in the United States before reaching commercialization, which may initially be only for the treatment of severe hypertriglyceridemia. The FDA may require Acasti to conduct additional clinical studies to obtain FDA approval in severe hypertriglyceridemia and for the treatment of mild to moderate hypertriglyceridemia which may include a cardiovascular outcomes study. See “Acasti’s Business - Government Regulation” and “Acasti’s Business - Sales and Marketing”.
Sales and Marketing
The Corporation has exclusive global commercial rights to CaPre®. The Corporation does not currently have in-house sales and marketing or distribution capabilities and the Corporation currently plans to seek an established commercial partner for the distribution of CaPre® if it reaches commercialization. In addition to completing a Phase III clinical trial and the long-term nonclinical studies, the Corporation expects that additional time and capital will be required to complete the filing of a NDA to obtain FDA approval for CaPre® in the United States and to complete marketing and other pre-commercialization activities before reaching commercialization, which may initially be only for the treatment of severe hypertriglyceridemia. The FDA may also require Acasti to conduct additional clinical studies to obtain FDA approval for the treatment of mild to moderate hypertriglyceridemia, which may include a cardiovascular outcomes study. The Corporation would focus initially on specialists, cardiologists and primary care physicians who comprise the top prescribers of lipid-regulating therapies as part of the sales and marketing strategy for CaPre®. See “Risk Factors - Risks Related to Product Development, Regulatory Approval and Commercialization”.
ONEMIA® is being distributed in the United States by Acasti to physicians, who then can either provide it to their patients directly or via a website by using a dedicated medical food access code. Acasti also makes ONEMIA® available via distributors and behind-the-counter in some pharmacies. In 2012, Acasti made its first sales of ONEMIA® to a medical food distributor in the United States, which has begun distribution through its network of dispensing physicians under its own brand name. Acasti intends to make ONEMIA® available via additional distributors and behind-the-counter in more pharmacies in the United States and to secure additional distribution partners to commercialize ONEMIA® outside of the United States. Revenues of Acasti for the fiscal years 2015, 2014 and 2013 were all derived from the sale of ONEMIA® and amounted to approximately $271,000, $501,000 and $724,000, respectively. During its fiscal year ended February 28, 2015, more than 83% of sales of ONEMIA® were made through Acasti’s distribution partner in the United States and the remaining 17% came from direct sales by Acasti.
Competition
The biopharmaceuticals industry is highly competitive. There are many public and private biopharmaceutical companies, universities, governmental agencies and other research organizations actively engaged in the research and development of products that may be similar to the Corporation’s products or address similar markets. It is probable that the number of companies seeking to develop products similar to the Corporation’s products will increase. Many of these and other existing or potential competitors have substantially greater financial, technical and human resources than the Corporation does and may be better equipped to develop, manufacture and market products. These companies may develop and introduce products and processes competitive with or superior to Acasti’s. In addition, other technologies or products may be developed that have an entirely different approach or means of accomplishing the intended purposes of Acasti’s products, which might render the Corporation’s technology and products non-competitive or obsolete. Acasti’s competitors in the United States and elsewhere include large, well-established pharmaceutical companies, specialty pharmaceutical sales and marketing companies and specialized cardiovascular treatment companies. These companies include GlaxoSmithKline plc, which currently markets Lovaza, a prescription omega-3 for patients with severe hypertriglyceridemia, Abbott Laboratories, which currently markets Tricor and Trilipix (both fibrates) and Niaspan (niacin) for treatment of severe hypertriglyceridemia, and Amarin Corporation, which currently markets Vascepa, an ethyl-ester form of EPA, for the treatment of patients with severe hypertriglyceridemia.
In March 2011, Pronova BioPharma Norge AS, which owns the patents for Lovaza, entered into an agreement with Apotex Corp. and Apotex Inc. to settle their patent litigation in the United States related to Lovaza. Pursuant to the terms of the settlement agreement, Pronova granted Apotex a license to enter the U.S. market with a generic version of Lovaza in the first quarter of 2015, or earlier, depending on circumstances. As a result, Acasti expects Apotex to compete against it as well. Other companies are also seeking to introduce generic versions of Lovaza.
In addition, Acasti is aware of other pharmaceutical companies that are developing products that, if approved, would compete with CaPre®. These include a free fatty acid form of omega-3 (comprised of 55% EPA and 20% DHA) being developed by Omthera Pharmaceuticals, which was acquired by London-based AstraZeneca PLC on July 18, 2013. On May 6, 2014, AstraZeneca announced that the FDA had approved its product as an adjunct to diet to reduce triglyceride levels in adults with severe hypertriglyceridaemia. Enzymotec Ltd. also recently submitted an IND application and requested an end of Phase II meeting in order to ultimately receive a SPA from the FDA and proceed to conduct a Phase III clinical trial for its phytosterol-omega-3 drug candidate. Acasti believes other emerging biopharmaceutical companies (eg. Matinas Biopharma) are also developing potential treatments for hypertriglyceridemia based on omega-3 fatty acids,. CaPre® may also face competition from omega-3 dietary supplements that are available without a prescription. See “Risk Factors - Risks Related to Product Development, Regulatory Approval and Commercialization - The Corporation faces competition from other biotechnology and pharmaceutical companies and its operating results will suffer if the Corporation fails to compete effectively.”
32
There are also competitors in the medical food market. , Pivotal Therapeutics announced positive results for its clinical trial of Vascazen, a medical food product being developed to improve patient lipid profiles and reduce cardiovascular disease risk factors.
Intellectual Property
Acasti intends to obtain, maintain and enforce patent protection for its products, formulations, methods and other proprietary technologies, preserve its trade secrets and operate without infringing on the proprietary rights of other parties.
Patents
Acasti owns the following portfolio of patents, filed in various jurisdictions worldwide, including the United States, Canada, China, Japan, Australia and Europe:
|
Patent Family Description
|
Description
|
WO (PCT)
Application Number
&
U.S. Patent
Number
|
Expiration Date of
the Patent Family
|
Number
of Patents
Worldwide
|
|
Concentrated Therapeutic Phospholipid Composition
|
Composition of Matter
|
WO2011050474 &
US8,586,567;
|
2028**
|
10*
(pending in approx. 40 countries)
|
|
|
*
|
Five Australian innovation patents are valid until 2018 and patent (ZL 201080059930.4) granted by the Chinese Patent Office is valid until 2030
|
On November 19, 2013, the United States Patent and Trademark Office granted Acasti a concentrated phospholipid composition patent (US8,586,567) covering concentrated therapeutic phospholipid compositions useful for treating or preventing diseases associated with cardiovascular disease, metabolic syndrome, inflammation and diseases associated therewith, neurodevelopmental diseases, and neurodegenerative diseases, comprising administering an effective amount of a concentrated therapeutic phospholipid composition. The patent is valid until 2028, covers specific omega-3 phospholipid compositions, synthetic and/or natural, regardless of the extraction process, suitable for human consumption. The patent protects Acasti’s phospholipid compositions, namely Capre® and Onemia®.
The corresponding US8,586,567 Acasti patent has also been granted in South Africa and Panama, and 5 innovation patents have been granted to Acasti in Australia (which innovation patents in Australia expire in 2018), while continuations have been filed in the US.
On March 25, 2015, Acasti announced that that the Chinese Patent Office had granted Acasti a composition and use patent. The Patent (ZL 201080059930.4), which is valid until 2030, relates to concentrated therapeutic phospholipid omega-3 compositions and covers methods for treating or preventing diseases associated with cardiovascular diseases, metabolic syndrome, inflammation, neurodevelopmental diseases, and neurodegenerative diseases.
To this day, Acasti’s patents and pending patent applications have not been opposed and/or challenged by third parties, in Canada, the United States and Europe. The patent is currently under opposition by BIO-MER Ltd. in New Zealand. Acasti intends on defending its patent and will file its Counter-Statement of Opposition in the next few months.
A patent is generally valid for 20 years from the date of first filing. Patent terms can vary slightly for other jurisdictions, with 20 years from filing being the norm. In certain jurisdictions exclusivity can be formally extended beyond the normal patent term to compensate for regulatory delays during the pre-market approval process.
33
Licensed Rights
In August 2008, Neptune granted to Acasti a license to rights on its intellectual property portfolio related to cardiovascular pharmaceutical applications. This license allows Acasti to exploit the subject intellectual property rights in order to develop novel active pharmaceutical ingredients (“APIs”) into commercial products for the medical food and the prescription drug markets. Acasti is responsible for carrying out the research and development of the APIs, as well as required regulatory submissions and approvals and intellectual property filings relating to the cardiovascular applications. The following table summarizes the patent applications related to Acasti’s license from Neptune.
|
Patent description
|
US Patent #
|
Expiration Date of the Patent
|
Holder
|
|
Composition of Matter
(natural phospholipids of marine origin containing flavonoids and polyunsaturated phospholipids and their uses)
|
US8,030,348 (1)
|
2022
|
Neptune
|
|
Method of Use for Dyslipidemia
(krill and/or marine extracts for prevention and/or treatment of cardiovascular diseases, arthritis, skin cancer, premenstrual syndrome, diabetes and transdermal transport)
|
US8,057,825
|
2022
|
Neptune
|
|
Method of Extraction
(Method of extracting lipids from marine and aquatic animal tissues)
|
US6,800,299
|
2019
|
Neptune
|
_________________
Note:
|
(1)
|
Three continuations also stem from U.S. Pat. 8,030,348 (U.S. Pat. 8,278,351; 8,680,080; and 8,383,675).
|
The license agreement provides that the products developed by Acasti must comply with the ranges specified in the license agreement pertaining to specific concentrations of phospholipids.
As a result of the royalty prepayment transaction entered into between Neptune and Acasti on December 4, 2012, Acasti is no longer required to pay any royalties to Neptune under the license agreement during its term for the use of the intellectual property under license.
Pursuant to the terms and conditions of the license agreement, Acasti is required, at Neptune’s option, to have its products, if any, manufactured by Neptune at prices determined according to different cost-plus rates for each of the product categories under the license. A copy of the license agreement is available on SEDAR at www.sedar.com
Acasti has also initiated its patent portfolio with the first application as a U.S. provisional of a composition and use patent. The invention is entitled “Concentrated Therapeutic Phospholipid Compositions (US20110160161)” and relates to concentrated therapeutic phospholipids compositions; methods for treating or preventing diseases associated with cardiovascular disease, metabolic syndrome, inflammation and diseases associated therewith, neurodevelopmental diseases, and neurodegenerative diseases, comprising administering an effective amount of a concentrated therapeutic phospholipids composition. Acasti’s patent application has been filed in more than 40 jurisdictions worldwide. On August 23, 2013, Acasti was granted its first patent in South Africa in the Concentrated Therapeutic Phospholipid Compositions family. The patent is in force and valid until October 29, 2029.
Settlement and License Agreements
On October 2, 2013, the Corporation announced the conclusion of a settlement with Rimfrost, resolving the ITC investigation related to infringement of Neptune’s composition of matter patents. As part of the settlement, Neptune granted a world-wide, non-exclusive, royalty-bearing licence to these settling respondents, allowing them to market and sell nutraceutical products containing components extracted from krill. The respondents in question also agreed to pay Neptune an additional royalty amount for the manufacture and sale of krill products prior to the effective license commencement date. Neptune also agreed to dismiss a related patent infringement case against Rimfrost filed in March of 2013.
On December 17, 2013 and April 27, 2014, the Corporation announced that it had successfully concluded a settlement and license agreement with Aker and Enzymotec, respectively. Neptune granted a world-wide, non-exclusive, royalty-bearing license to both parties to market and sell nutraceutical products in the licensed countries. Per the settlement, Aker agreed to pay Neptune an additional non-refundable payment for the manufacture and sale of krill products prior to the effective decision date of the U.S. Patent and Trademark Office (the “USPTO”). Further, Enzymotec agreed to pay Neptune a non-refundable one-time upfront settlement payment. Pursuant to the terms of these settlements, royalty levels in the US depended on the outcome of an inter partes review at the PTAB of certain claims from Neptune’s ‘351 patent. In light of the PTAB’s decision, Aker and Enzymotec will be obligated to make royalty payments to Neptune based on their sales of licensed krill oil products in the US. On December 17, 2013 and April 27, 2014, the Corporation announced that it had successfully concluded a settlement and license agreement with Aker and Enzymotec, respectively. Neptune granted a world-wide, non-exclusive, royalty-bearing license to both parties to market and sell nutraceutical products in the licensed countries. Per the settlement, Aker agreed to pay Neptune an additional non-refundable payment for the manufacture and sale of krill products prior to the effective USPTO decision date. Further, Enzymotec agreed to pay Neptune a non-refundable one-time upfront settlement payment. Pursuant to the terms of these settlements, royalty levels in the US were depended on the outcome of an inter partes review at the PTAB of certain claims from Neptune’s ‘351 patent. In light of the PTAB’s decision, Aker and Enzymotec will be obligated to make royalty payments to Neptune based on their sales of licensed krill oil products in the US.
34
On May 15, 2015, Neptune filed a Complaint in the United States District Court for the Southern District of New York against Aker Biomarine AS, Aker Biomarine Antarctic USA, Inc. and Aker Biomarine Antarctic AS. Neptune is requesting a judgement against the Defendants declaring, amongst other things, that they must pay ongoing royalties on sales of Krill Oil Based Products made on or after March 23, 2015.
Under the terms of the settlement agreement with Enzymotec, royalty obligations in Australia were similarly dependent on the outcome of a potential request with the Australian Patent Office for a review of certain claims of Neptune’s Australian composition of matter patent (AU 2002322233). Enzymotec decided to pursue a patent re-examination. On May 25, 2015, the Australian Patent Office confirmed that Neptune Australian patent is patentable.
Brand names and trademarks
Acasti has applied for worldwide trademark protection of CaPre® as well as for the trademark ONEMIA®, and is the owner of the trademark BREAKING DOWN THE WALLS OF CHOLESTEROL™ in Canada, the United States and the European Union. The trademark CaPre® is now registered in certain jurisdictions including the United States, Canada and Europe.
Trade Secrets
In addition, Acasti protects its optimization and extraction processes through industrial trade secrets and know-how.
Raw Materials, Manufacturing and Facility
The Corporation’s head office and operations are located at 545, Promenade Centropolis, suite 100, Laval, Québec, Canada, H7T 0A3. The Corporation leases its premises for approximately $6,500 per month.
Acasti uses krill oil as its primary raw material to produce CaPre® and ONEMIA®. There are two ocean regions where krill is generally harvested: the Southern Ocean (Antarctic krill Euphausia superba) and the Northern Pacific Ocean (Pacific krill Euphausia pacifica), mainly off the coasts of Japan and Canada. The total quantity of the krill species in these two oceans is estimated to be at least 500,000,000 metric tons. The World Health Organization estimates that approximately 271,000 metric tons of both krill species are harvested annually. From 2002 to 2011, between 105,000 to 212,000 metric tons originated from the Southern Ocean and, on average, 60,000 harvested metric tons originated from the Northern Pacific Ocean each year. The annual Antarctic krill catches represent an estimated 0.05% of the existing resource. Acasti’s products are derived from Antarctic krill.
According to the Commission for the Conservation of Antarctic Marine Living Resources, from 2008 to 2011, annual quotas for Antarctic krill have increased by 33%. Annual allowable quotas of 6.555 million metric tons for 2010 were increased to 8.695 million metric tons for 2011. In the areas currently being fished for krill, the Commission has established a combined annual catch suspension trigger level of 620,000 metric tons. If the trigger level is reached, the Commission may intervene to authorize additional krill harvesting and impose a striker control on fisheries. As a result, the Corporation believes that krill is an abundant and accessible resource with potential for long-term sustainable exploitation. The average market price for whole frozen krill is approximately US$900 per metric ton. See “Risk Factors - Risks Related to Product Development, Regulatory Approval and Commercialization.”
Acasti does not own its own manufacturing facility for the production of krill oil, CaPre® and ONEMIA® nor does it have plans to develop its own manufacturing facility in the foreseeable future. Acasti depends on third party suppliers and manufacturers for all of its required RKO and drug substance and products and, if approved for distribution by the FDA, Acasti expects to rely on cGMP- compliant third parties to manufacture NKPL66, encapsulate, bottle and package clinical supplies of CaPre®.
The Corporation entered into contractual agreements with a third party for the manufacturing, in accordance with cGMP regulations imposed by the FDA, of CaPre® clinical material for the purposes of Acasti’s upcoming clinical trials. See “Risk Factors – Risks Related to Product Development, Regulatory Approval and Commercialization – The Corporation’s supply of krill oil for commercial supply and clinical trials is dependent upon relationships with Neptune and other third party manufacturers and key suppliers” and “Risk Factors - Risks Related to Product Development, Regulatory Approval and Commercialization - The Corporation relies on third parties for the manufacturing, production and supply of CaPre® and ONEMIA® and may be adversely affected if those third parties are unable or unwilling to fulfill their obligations.”
35
Employees, Specialized Skills and Knowledge
Acasti’s management consists of professionals experienced in business development, finance and science. The Acasti research team includes scientists with expertise in pharmaceutical development, chemistry, manufacturing and controls, nonclinical and clinical studies, pharmacology, regulatory affairs, quality assurance/quality control, intellectual property and strategic alliances. As of February 28, 2015, the Corporation employed seven people in Canada, six of whom have biology, chemistry, biochemistry or microbiology credentials, and one administrative staff with a pharmaceutical industry background. Acasti generally requires all of its employees to enter into an invention assignment, non-disclosure and non-compete agreement. The Corporation relies, in part, on the administrative and other staff of its parent company, Neptune, and also relies on consultants from time to time. The Corporation’s employees are not covered by any collective bargaining agreement or represented by a trade union. The Corporation places special emphasis on training for its personnel.
Litigation
Due to the fact that a significant portion of the Corporation’s intellectual property rights are licensed to it by Neptune, the Corporation relies on Neptune to protect a significant portion of the intellectual property rights that it uses under such license. Neptune is engaged in a number of legal actions related to its intellectual property.
Henri Harland
On May 29, 2014, Henri Harland, former President and Chief Executive Officer of the Corporation filed a lawsuit against the Corporation, Neptune and NeuroBioPharm Inc. (“NeuroBioPharm”) in connection with his departure as President and Chief Executive Officer of each of Neptune, Acasti and NeuroBioPharm. Among other things, Mr. Harland alleged that his resignation occurred as a result of a constructive dismissal and is seeking approximately $8.5 million in damages, interest and costs. In addition, Mr. Harland is seeking from Neptune, Acasti and NeuroBioPharm, as applicable, the issuance of 500,000 shares of each of Neptune, Acasti and NeuroBioPharm as well as two blocks of 1,000,000 call options on shares held by Neptune in Acasti and NeuroBioPharm. As a result of the lawsuit, Mr. Harland was requested to resign as Director of the Corporation. On December 11, 2014, Neptune, Acasti and NeuroBioPharm filed their defense and counterclaim alleging inter alia that Mr. Harland’s contract is null and void and that he is owed nothing following his resignation. Should the Court determine that the contract is nonetheless valid, the Defendants’ position, as stated in the defense and counterclaim, is that there was also enough evidence discovered after Mr. Harland’s resignation that would have justified a dismissal for cause and that again, nothing is owed to the plaintiff. No trial date has been set. As of May 27, 2015, no agreement has been reached and an estimate of its financial effect cannot be made.
Government Regulation
United States Drug Development
Government authorities in the United States, at the federal, state and local level, and in other countries extensively regulate, among other things, the research, development, testing, manufacture, quality control, approval, labeling, packaging, storage, record-keeping, promotion, advertising, distribution, post-approval monitoring and reporting, marketing and export and import of drug products such as CaPre®. Generally, before a new drug can be marketed, considerable data demonstrating its quality, safety and efficacy must be obtained, organized into a format specific to each regulatory authority, submitted for review and approved by the regulatory authority.
FDA Regulatory Process
In the United States, the FDA regulates drugs under the Federal Food, Drug and Cosmetic Act and its implementing regulations. Drugs are also subject to other federal, state and local statutes and regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state and local statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable requirements at any time during the product development or approval process, or after approval, may subject an applicant to administrative or judicial sanctions. These sanctions could include, among other actions, the FDA’s refusal to approve pending applications, withdrawal of an approval, a “clinical hold” on investigations intended to support FDA approval, warning letters, product recalls or withdrawals from the market, product seizures, total or partial suspension of production or distribution injunctions, fines, refusals of government contracts, debarment from government programs, restitution, disgorgement, civil or criminal penalties, or entry of consent decrees and integrity agreements. Any agency or judicial enforcement action could have a material adverse effect on Acasti.
36
In order to be marketed in the United States, CaPre® must be approved by the FDA through the NDA process. The process required before a drug may be marketed in the United States generally involves the following:
|
|
·
|
completion of extensive nonclinical (animal) and formulation studies in accordance with applicable regulations, including the FDA’s Good Laboratory Practice (“GLP”) regulations;
|
|
|
·
|
submission of an IND, which must become effective before human clinical trials may begin in the United States;
|
|
|
·
|
performance of adequate and well-controlled clinical trials in accordance with the applicable IND and other clinical study-related regulations, such as current Good Clinical Practices, to establish the safety and efficacy of the proposed drug for its proposed indication;
|
|
|
·
|
submission of an NDA for a new drug;
|
|
|
·
|
satisfactory completion of an FDA pre-approval inspection of the manufacturing facility or facilities where the drug is produced to assess compliance with cGMP to assure that the facilities, methods and controls are adequate to preserve the drug’s identity, strength, quality and purity;
|
|
|
·
|
satisfactory completion of potential FDA audit of the nonclinical and/or clinical trial sites that generated the data in support of the NDA; and
|
|
|
·
|
FDA review and approval of the NDA prior to any commercial marketing or sale of the drug in the United States.
|
The data required to support an NDA is generated in two distinct development stages: nonclinical and clinical. The nonclinical development stage generally involves synthesizing or otherwise producing the active component, developing the formulation and determining the manufacturing process, as well as carrying out non-human toxicology, pharmacology and drug metabolism studies in the laboratory, which support subsequent clinical testing. The sponsor must submit the results of the nonclinical tests, together with manufacturing information, analytical data, any available clinical data or literature and a proposed clinical protocol, to the FDA as part of the IND, which is a request for authorization from the FDA to administer an investigational drug product to humans. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA raises concerns or questions regarding the proposed clinical trials. The FDA may also place the IND on clinical hold within that 30-day time period. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. A clinical hold may be imposed at any time before or during a clinical trial due to safety concerns or non-compliance. Accordingly, the Corporation cannot be sure that submission of an IND will result in the FDA allowing clinical trials to begin, or that, once begun, issues will not arise that could cause the trial to be suspended or terminated.
The clinical stage of development involves the administration of the investigational drug to healthy volunteers or patients under the supervision of qualified investigators, generally physicians not employed by or under the trial sponsor’s control, in accordance with cGCPs, which include the requirement that all research subjects provide their informed consent for their participation in any clinical trial. Clinical trials are conducted under protocols detailing, among other things, the objectives of the clinical trial, dosing procedures, subject selection and exclusion criteria, data collection, and the parameters to be used to monitor subject safety and assess the investigational drug’s efficacy. Each protocol, and any subsequent amendments to the protocol or new investigator’s information, must be submitted to the FDA as part of the IND. Further, each clinical trial must be reviewed and approved by an independent institutional review board (“IRB”) at or servicing each institution at which the clinical trial will be conducted. An IRB is charged with protecting the welfare and rights of trial participants and considers such items as whether the risks to individuals participating in the clinical trials are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the informed consent form that must be provided to each clinical trial subject or its legal representative. There are also requirements governing the reporting of ongoing clinical trials and completed clinical trial results to public registries, as well as reporting of safety information under the IND.
37
Clinical studies are generally conducted in three sequential phases that may overlap, known as Phase I, Phase II and Phase III clinical trials. Phase I generally involves a small number of healthy volunteers who are initially exposed to a single dose and then multiple doses of the investigational drug. The primary purpose of these studies is to assess the metabolism, pharmacologic action, side effect tolerability and safety of the drug. Phase II trials typically involve studies in disease-affected patients to determine the dose required to produce the desired benefits. At the same time, safety and further pharmacokinetic and pharmacodynamic information is collected, as well as identification of possible adverse effects and safety risks and preliminary evaluation of efficacy. Phase III clinical trials generally involve large numbers of patients at multiple sites, often in multiple countries (from several hundred to several thousand subjects) and are designed to provide the data necessary to demonstrate the effectiveness of the product for its intended use, its safety in use, and to establish the overall benefit/risk relationship of the product and provide an adequate basis for product approval. Phase III clinical trials should, if possible, include comparisons with placebo and may include a comparison to approved therapies. The duration of treatment is often extended to mimic the actual use of a product during marketing. Generally, two adequate and well-controlled Phase III clinical trials are required by the FDA for approval of an NDA (Pivotal Studies).
Progress reports detailing the results of the clinical trials must be submitted at least annually to the FDA. In addition, written IND safety reports must be submitted to the FDA and the investigators for serious and unexpected adverse events or any finding from tests in laboratory animals that suggests a significant risk for human subjects. The FDA, the IRB, or the sponsor may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research subjects or patients are being exposed to an unacceptable health risk. Additionally, some clinical trials are overseen by an independent group of qualified experts organized by the clinical trial sponsor, known as a data safety monitoring board or committee. This group provides oversight and will determine whether or not a trial may move forward at designated check points based on review of interim data from the study. A clinical trial may be terminated or suspended based on evolving business objectives and/or competitive climate.
The manufacturing process must be capable of consistently producing quality batches of the investigational drug and, among other things, must develop methods for testing the identity, strength, quality and purity of the final drug product. The sponsor must develop appropriate labeling that sets forth the conditions of intended use. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the drug candidate does not undergo unacceptable deterioration over its shelf life.
Post-approval studies, sometimes referred to as Phase IV clinical trials, may be conducted after initial marketing approval. These studies are used to gain additional experience from the treatment of patients in the intended therapeutic indication. In certain instances, the FDA may mandate the performance of Phase IV studies as part of a post-approval commitment, such as pediatric studies.
NDA and FDA Review Process
Nonclinical and clinical information is filed with the FDA in an NDA along with proposed labeling. The NDA is a request for approval to market the drug and must contain proof of safety, purity, potency and efficacy, which is demonstrated by extensive nonclinical and clinical testing. Data may come from company-sponsored clinical trials intended to test the safety and effectiveness of a use of a product, or from a number of alternative sources, including studies initiated by investigators. To support marketing approval, the data submitted must be sufficient in quality and quantity to establish the safety and effectiveness of the investigational drug product to the satisfaction of the FDA.
The submission of an NDA is subject to the payment of substantial user fees; a waiver of such fees may be obtained under certain limited circumstances. FDA approval of an NDA must be obtained before marketing a drug in the United States. In addition, under the Pediatric Research Equity Act, an NDA or supplement to an NDA must contain data to assess the safety and effectiveness of the drug for the claimed indications in all relevant pediatric subpopulations and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The FDA may grant deferrals for submission of data or full or partial waivers.
The FDA reviews all NDAs submitted before it accepts them for filing and may request additional information. The FDA must make a decision on accepting an NDA for filing within 60 days of receipt. Once the submission is accepted for filing, the FDA begins an in-depth review of the NDA. Under the goals and policies agreed to by the FDA under the Prescription Drug User Fee Act (“PDUFA”) the FDA has ten months from the filing date in which to complete its initial review of a standard NDA and respond to the applicant. This review typically takes 12 months from the date the NDA is submitted to the FDA including the screening which takes a period of 60 days. The FDA does not always meet its PDUFA goal dates for standard NDAs, and the review process is often significantly extended by FDA requests for additional information or clarification.
After the NDA submission is accepted for filing, the FDA reviews the NDA to determine, among other things, whether the proposed product is safe and effective for its intended use, and whether the product is being manufactured in accordance with cGMP to assure and preserve the product’s identity, strength, quality and purity. The FDA will likely re-analyze the clinical trial data, which could result in extensive discussions with the FDA.
Before approving an NDA, the FDA will conduct a pre-approval inspection of the manufacturing facilities for the new product to determine whether they comply with cGMP. The FDA will not approve the product unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. In addition, before approving an NDA, the FDA may also audit data from clinical trials to ensure compliance with cGCP requirements. After the FDA evaluates the application, manufacturing process and manufacturing facilities, it will issue a Complete Response Letter (“CRL”). A CRL indicates that the review cycle of the application is complete and whether the application is approved and, when applicable, the CRL describes the specific deficiencies in the NDA and may require additional clinical data and/or an additional Phase III clinical trial(s), and/or other significant and time-consuming requirements related to clinical trials, nonclinical studies or manufacturing. The applicant may either resubmit the NDA, addressing all of the deficiencies identified in the letter, or withdraw the application. Even if such data and information is submitted, the FDA may ultimately decide that the NDA does not satisfy the criteria for approval. Data obtained from clinical trials are not always conclusive and the FDA may interpret data differently than the Corporation interprets the same data.
38
There is no assurance that the FDA will ultimately approve a drug product for marketing in the United States and the Corporation may encounter significant difficulties or costs during the review process. If a product receives marketing approval, the approval may be significantly limited to specific diseases and dosages or the indications for use may otherwise be limited, which could restrict the commercial value of the product. Further, the FDA may require that certain contraindications, warnings or precautions be included in the product labeling, may condition the approval of the NDA on other changes to the proposed labeling, or may require a Risk Evaluation and Mitigation Strategy (REMS), which could limit the Corporation’s ability to market the drug once approved. The FDA may also require the development of adequate controls and specifications, or a commitment to conduct post-market testing or clinical trials and surveillance to monitor the effects of approved products.
U.S. Post-Marketing Requirements
Following approval of a new product, a pharmaceutical company and the approved product are subject to continuing regulation by the FDA, including, among other things, monitoring and recordkeeping activities, reporting to the applicable regulatory authorities of adverse experiences with the product, providing the regulatory authorities with updated safety and efficacy information, product sampling and distribution requirements, and complying with promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, restrictions on promoting drugs for uses or in patient populations that are not described in the drug's approved labeling (“off-label use”), limitations on industry-sponsored scientific and educational activities, and requirements for promotional activities involving the internet. Although physicians may prescribe legally available drugs for off-label uses, manufacturers and distributors may not market or promote such off-label uses. Modifications or enhancements to the product or its labeling or changes of the site of manufacture are often subject to the approval of the FDA and other regulators, which may or may not be received or may result in a lengthy review process. In some cases, these changes will require the submission of clinical data and the payment of a user fee.
U.S. Patent Term Restoration and Marketing Exclusivity
Depending upon the timing, duration and specifics of the FDA approval of Acasti’s prescription drug candidates, some of Acasti’s U.S. patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, commonly referred to as the Hatch-Waxman Amendments. The Hatch-Waxman Amendments permit a patent restoration term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, patent term restoration cannot extend the remaining term of a patent beyond a total of 14 years from the product's approval date. The patent term restoration period is generally one-half the time between the effective date of an IND and the submission date of an NDA plus the time between the submission date of an NDA and the approval of that application. Only one patent applicable to an approved drug is eligible for the extension and the application for the extension must be submitted prior to the expiration of the patent. The USPTO in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In the future, Acasti intends to apply for restoration of patent term for one of its currently owned or licensed patents to add patent life beyond its current expiration date, depending on the expected length of the clinical trials and other factors involved in the filing and review of the relevant NDA.
Non-U.S. Drug Regulation
In Canada, biopharmaceutical product candidates are regulated by the Food and Drugs Act and the rules and regulations promulgated thereunder, which are enforced by the Therapeutic Products Directorate of Health Canada. In order to obtain approval for commercializing new drugs in Canada, the sponsor (Acasti) must satisfy many regulatory conditions. The sponsor must first complete preclinical studies in order to file a clinical trial application (“CTA”) in Canada. The sponsor will then receive different clearance authorizations to proceed with Phase I clinical trials, which can then lead to Phase II and Phase III clinical trials. Once all three phases of trials are completed, the sponsor must file a registration file named a New Drug Submission (“NDS”) in Canada. If the NDS demonstrates that the product was developed in accordance with the regulatory authorities’ rules, regulations and guidelines and demonstrates favorable safety and efficacy and receives a favorable risk/benefit analysis, then the regulatory authorities issue a notice of compliance, which allows the sponsor to market the product.
39
In addition to regulations in the United States and Canada, Acasti is subject to a variety of regulations governing clinical studies and commercial sales and distribution of its products in other jurisdictions around the world. These laws and regulations typically require the licensing of manufacturing and contract research facilities, carefully controlled research and testing of product candidates and governmental review and approval of results prior to marketing therapeutic product candidates. Additionally, they require adherence to good laboratory practices, good clinical practices and good manufacturing practices during production. The process of new drug approvals by regulators in the United States, Canada and the European Union are generally considered to be among the most rigorous in the world.
Whether or not the FDA or Health Canada approval is obtained for a product, Acasti must obtain approvals from the comparable regulatory authorities of other countries before it can commence clinical studies or marketing of the product in those countries. The approval process varies from country to country and the time may be longer or shorter than that required for the FDA or Health Canada approval. The requirements governing the conduct of clinical studies, product licensing, pricing and reimbursement vary greatly from country to country. In some international markets, additional clinical trials may be required prior to the filing or approval of marketing applications within the country.
Medical Food Regulation
Prior to 1972, medical foods that mitigated serious adverse effects of the underlying diseases were regulated by the FDA as “drugs” under the Federal Food, Drug, and Cosmetic Act. In 1972, in an effort to encourage innovation and availability of such products, the FDA revised its regulatory approach and classified these products as “foods for special dietary use.” The Orphan Drug Amendments of 1988 provided a statutory definition of a medical food, which means a food that is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition, for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation. In the Nutrition Labeling and Education Act of 1990, the U.S. Congress exempted medical foods from the nutrition labeling, health claim, and nutrient disclosure requirements applicable to most other foods, further distinguishing this category from conventional food products.
The regulatory status of these products in other countries varies. It is also possible that such products would be regulated in Canada as natural health products pursuant to the Natural Health Products Regulations.
Active Pharmaceutical Ingredient Regulation
The FDA will regulate finished products containing APIs developed or under development by Acasti; however, the FDA does not actively regulate the APIs themselves. Depending on its intended uses, a finished product containing the API may be regulated as a drug or a medical food under the procedures described above. It may be possible to market a finished product containing an API developed or under development by Acasti as a dietary supplement. Dietary supplements do not require FDA premarket approval. However, it may be necessary to submit a notification to the FDA that a company intends to market a dietary supplement containing a “new dietary ingredient.” In general, the regulatory requirements in other countries also depend on the nature of the finished product and do not focus on the API itself.
|
C.
|
Organizational Structure
|
The Corporation has no subsidiaries. As of May 27, 2015, Neptune owns 50,755,933 Class A shares of Acasti (the “Common Shares”), representing approximately 47.68% of the Common Shares issued and outstanding. The Common Shares are voting, participating and have no par value. Neptune also owns a warrant entitling it to acquire 592,500 Common Shares.
|
D.
|
Property, Plants and Equipment
|
The Corporation’s head office and operations are located at 545, Promenade Centropolis, suite 100, Laval, Québec, Canada, H7T 0A3. The Corporation leases its premises for approximately $6,500 per month.
Acasti does not own its own manufacturing facility for the production of krill oil, CaPre® and ONEMIA® nor does it have plans to develop its own manufacturing facility in the foreseeable future. Acasti depends on third party suppliers and manufacturers for all of its required RKO and drug substance and products and, if approved for distribution by the FDA, Acasti expects to rely on cGMP- compliant third parties to manufacture NKPL66, encapsulate, bottle and package clinical supplies of CaPre®.
40
The Corporation entered into contractual agreements with a third party for the manufacturing, in accordance with cGMP regulations imposed by the FDA, of CaPre® clinical material for the purposes of Acasti’s upcoming clinical trials. See “Risk Factors – Risks Related to Product Development, Regulatory Approval and Commercialization – The Corporation’s supply of krill oil for commercial supply and clinical trials is dependent upon relationships with Neptune and other third party manufacturers and key suppliers” and “Risk Factors - Risks Related to Product Development, Regulatory Approval and Commercialization - The Corporation relies on third parties for the manufacturing, production and supply of CaPre® and ONEMIA® and may be adversely affected if those third parties are unable or unwilling to fulfill their obligations.” We are not subject to any material environmental risk in connection with our property, plants or equipment.
|
Item 4A.
|
Unresolved Staff Comments
|
Not applicable.
|
Item 5.
|
Operating and Financial Review and Prospects
|
Information relating to our operating and financial review and prospects are detailed in the MD&A, for the years ended February 28, 2015, February 28, 2014 and February 28, 2013 included herein, and in conjunction with the audited consolidated financial statements and related notes included at “Item 17 – Financial Statements” of this Annual Report.
|
A.
|
Operating Results
|
Refer to our MD&A included below in this Annual Report.
|
B.
|
Liquidity and Capital Resources
|
Refer to our MD&A included below in this Annual Report.
|
C.
|
Research and Development, Patents and Licenses, etc.
|
We incurred research and development costs net of tax credits amounting to $6,521,717, $4,297,195 and $3,009,016 in the years ended February 28, 2015, February 28, 2014 and February 29, 2013, respectively. Refer to the MD&A included below and to “Item 4.B – Business Overview” of this Annual Report.
|
D.
|
Trend Information
|
The only trend during the current fiscal year reasonably likely to affect our net sales or revenues, income from continuing operations, profitability, liquidity or capital resources, or that would cause our reported financial information not necessarily to be indicative of future operating results or financial condition is our expectation that research and development expenses will continue to trend upward as we pursue our product development strategy. Please refer to the MD&A included below.
|
E.
|
Off-Balance Sheet Arrangements
|
Refer to our MD&A included below in this Annual Report.
|
F.
|
Tabular Disclosure of Contractual Obligations
|
Refer to our MD&A included below in this Annual Report.
|
G.
|
Safe Harbor
|
This annual report contains forward-looking statements, principally in “Item 4 - Information on the Company” and “Item 5 - Operating and Financial Review and Prospects”. These statements may be identified by the use of words like “plan”, “expect”, “aim”, believe”, “project”, “anticipate”, “intend”, “estimate”, “will”, “should”, “could” and similar expressions in connection with any discussion, expectation, or projection of future operating or financial performance, events or trends. In particular, these include statements about the Corporation’s strategy for growth, future performance or results of current sales and production, interest rates, foreign exchange rates, and the outcome of contingencies, such as acquisitions and/or legal proceedings and intellectual property issues.
41
Forward-looking statements are based on certain assumptions and expectations of future events that are subject to risks and uncertainties. Actual future results and trends may differ materially from historical results or those projected in any such forward-looking statements depending on a variety of factors, including, among other things, the factors discussed in this annual report under “Item 3.D - Risk Factors” and factors described in documents that the Corporation may furnish from time to time to the SEC. Except as required by law, the Corporation undertakes no obligation to update publicly or revise any forward-looking statements because of new information. Please refer to the forward-looking statements section at the beginning of this annual report.
MANAGEMENT’S ANALYSIS OF THE FINANCIAL SITUATION AND OPERATING RESULTS — YEARS ENDED FEBRUARY 28, 2015 AND FEBRUARY 28, 2014 AND FEBRUARY 28, 2013
This management’s discussion and analysis (“MD&A”) is presented in order to provide the reader with an overview of the financial results and changes to the financial position of Acasti Pharma Inc. (“Acasti” or the “Corporation”) as at February 28, 2015 and for the year then ended. This MD&A explains the material variations in the financial statements of operations, financial position and cash flows of Acasti for the years ended February 28, 2015, 2014 and 2013. The Corporation effectively commenced active operations with the transfer of an exclusive worldwide license from its parent corporation, Neptune Technologies & Bioressources Inc. (“Neptune”), in August 2008. The Corporation was inactive prior to that date.
This MD&A, completed on May 27, 2015, must be read in conjunction with the Corporation’s audited financial statements for the years ended February 28, 2015, 2014 and 2013. The Corporation’s audited financial statements were prepared in accordance with International Financing Reporting Standards (“IFRS”), as issued by the International Accounting Standards Board and were authorized for issue by the Board of Directors on May 27, 2015. The MD&A and audited financial statements of the Corporation were previously furnished on a Form 6-K with the SEC on May 27, 2015. The Corporation’s financial results are published in Canadian dollars. All amounts appearing in this MD&A are in thousands of Canadian dollars, except share and per share amounts or unless otherwise indicated.
Additional information on the Corporation can be found on the SEDAR website at www.sedar.com and on the EDGAR website at www.sec.gov/edgar.shtml under Acasti Pharma Inc.
On March 31, 2011, following the submission of an initial listing application, the Class A shares of the Corporation were listed for trading on the TSX Venture Exchange under the ticker symbol “APO”. In January 2013, the Corporation had its Class A shares listed on the NASDAQ Capital Market exchange, under the symbol “ACST”.
Business Overview
Acasti is an emerging biopharmaceutical company focused on the research, development and commercialization of new krill oil-based forms of omega-3 phospholipid therapies for the treatment and prevention of certain cardiometabolic disorders, in particular abnormalities in blood lipids, also known as dyslipidemia. Because krill feeds on phytoplankton (diatoms and dinoflagellates), it is a major source of phospholipids and polyunsaturated fatty acids, mainly eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which are two types of omega-3 fatty acids well known to be beneficial for human health.
CaPre®, Acasti’s prescription drug candidate, is a highly purified omega-3 phospholipid concentrate derived from krill oil and is being developed to help prevent and treat hypertriglyceridemia, a condition characterized by abnormally high levels of triglycerides in the bloodstream. In 2011, two Phase II clinical trials were initiated in Canada (the TRIFECTA trial and the COLT trial) to evaluate the safety and efficacy of CaPre® for the management of mild to severe hypertriglyceridemia (high triglycerides with levels ranging from 200 to 877 mg/dL). Both trials also include the secondary objective of evaluating the effect of CaPre® in patients with mild to moderate hypertriglyceridemia (high triglycerides levels ranging from 200 to 499 mg/dL) as well as in patients with severe hypertriglyceridemia (very high triglycerides levels ranging from 500 to 877 mg/dL). The open-label COLT trial was completed during the second quarter of the 2014 fiscal year and the TRIFECTA trial was completed in the second quarter of fiscal 2015. Based on the positive results of the COLT trial, Acasti filed an investigational new drug (“IND”) submission to the U.S. Food and Drug Administration (“FDA”) to conduct a pharmacokinetic study (“PK trial”) in the U.S. Acasti subsequently received approval to conduct the PK trial and it was completed in the second quarter of fiscal 2015.
Due to a recent decision of the FDA not to grant authorization to commercialize a competitor’s drug in the mild to moderate patient population before the demonstration of clinical outcome benefits, Acasti is reassessing its clinical strategy and may put a primary first focus on the severe hypertriglyceridemia population.
42
Onemia®, Acasti’s commercialized product, has been marketed in the United States since 2011 as a “medical food”. Onemia® is only administered under the supervision of a physician and is intended for the dietary management of omega-3 phospholipids deficiency related to abnormal lipid profiles and cardiometabolic disorders.
Pursuant to a license agreement entered into with Neptune in August 2008, Acasti has been granted a license to rights on Neptune’s intellectual property portfolio related to cardiovascular pharmaceutical applications (the “License Agreement”). In December 2012, the Corporation entered into a prepayment agreement with Neptune pursuant to which the Corporation exercised its option under the License Agreement to pay in advance all of the future royalties’ payable under the license in 2014. The royalty free license allows Acasti to exploit the subject intellectual property rights in order to develop novel active pharmaceutical ingredients (“APIs”) into commercial products for the medical food and the prescription drug markets. Acasti is responsible for carrying out the research and development of the APIs, as well as required regulatory submissions and approvals and intellectual property filings relating to the cardiovascular applications. The products developed by Acasti require the approval from the FDA before clinical studies are conducted and approval from similar regulatory organizations before sales are authorized.
Operations
During the year ended February 28, 2015, Acasti made progress in its research and pharmaceutical product development, advancing with its prescription drug candidate, CaPre®, while continuing its commercialization efforts for its medical food Onemia®. The following is a summary of the period’s highlights.
CaPre® - Clinical Trials Update
Acasti initiated two Phase II clinical trials in Canada (the COLT trial and the TRIFECTA trial) designed to evaluate the safety and efficacy of CaPre® for the management of mild to moderate hypertriglyceridemia (high triglycerides with levels ranging from 200 to 499 mg/dL) and severe hypertriglyceridemia (high triglycerides with levels over 500 mg/dL).
COLT Trial
The COLT trial, a randomized, open-label, dose-ranging, multi-center trial, was designed to assess the safety and efficacy of CaPre® in the treatment of patients with triglycerides levels between 2.28 and 10.0 mmol/L (200-877 mg/dL) (clinical trial.gov identifier NCT01516151). The primary objectives of the COLT trial were to evaluate the safety and efficacy of 0.5, 1.0, 2.0 and 4.0g of CaPre® per day in reducing fasting plasma triglycerides over 4 and 8 weeks as compared to the standard of care alone.
The secondary objectives of the COLT trial were to evaluate the effect of CaPre® on fasting plasma triglycerides in patients with triglycerides between 2.28 and 5.69 mmol/L (200-499 mg/dL) (mild to moderate hypertriglyceridemia); to evaluate the dose dependent effect on fasting plasma triglycerides in patients with triglycerides > 5.7 and <10 mmol/L (500-877 mg/dL); and to evaluate the effect of CaPre® on fasting plasma levels of LDL-C (direct measurement), HDL-C, non-HDL-C, hs-CRP and omega-3 index. Non-HDL-C is the total cholesterol minus the HDL-C.
The final results of the COLT trial indicated that CaPre® was safe and effective in reducing triglycerides in patients with mild to severe hypertriglyceridemia with significant mean (average) triglyceride reductions above 20% after 8 weeks of treatment with both daily doses of 4.0g and 2.0g. Demographics and baseline characteristics of the patient population were balanced in terms of age, race and gender. A total of 288 patients were enrolled and randomized and 270 patients completed the study, which exceeded the targeted number of evaluable patients. From this patient population, approximately 90% had mild to moderate hypertriglyceridemia.
CaPre® was safe and well tolerated. The proportion of patients treated with CaPre® that experienced one or more adverse events in the COLT trial was similar to that of the standard of care group (30.0% versus 34.5%, respectively). A substantial majority of adverse events were mild (82.3%) and no severe treatment-related adverse effects have been reported. Only one patient was discontinued from the study due to an adverse event of moderate intensity. It was noted that the rate of gastrointestinal side effects were higher in the CaPre® groups compared to standard of care alone and appeared to increase in a dose-related manner. However, none of the subjects participating in the study suffered from a serious adverse event. The report concludes that even at higher doses, CaPre® is safe and well tolerated with only transient and predominantly mild adverse events occurring at low rates.
The COLT trial met its primary objective showing CaPre® to be safe and effective in reducing triglycerides in patients with mild to severe hypertriglyceridemia. After only a 4-week treatment, CaPre® achieved a statistically significant triglyceride reduction as compared to standard of care alone. Standard of care could be any treatment physicians considered appropriate in a real-life clinical setting and included lifestyle modifications as well as lipid modifying agents, such as statins, ezetimibe and fibrates. Patients treated with 4.0g of CaPre® a day over 4 weeks reached a mean triglyceride decrease of 15.4% from baseline and a mean improvement of 18.0% over the standard of care. Results also showed increased benefits after 8 weeks of treatment, with patients on a daily dose of 4.0g of CaPre® registering a mean triglyceride decrease of 21.6% from baseline and a mean improvement of 14.4% over the standard of care. It is noteworthy that a mean triglyceride reduction of 7.1% was observed for the standard of care group at week 8, which may be explained by lipid lowering medication adjustments during the study, which was allowed to be administered in the standard of care group alone.
43
Moreover, after 8 weeks of treatment, patients treated with 1.0g for the first 4 weeks of treatment and 2.0g for the following 4 weeks showed a statistically significant triglycerides mean improvement of 16.2% over the standard of care, corresponding to a 23.3% reduction for the 1.0-2.0g as compared to a 7.1% reduction for the standard of care. After an 8 week treatment, patients treated with 2.0g of CaPre® for the entire 8 weeks showed statistically significant triglycerides mean improvements of 14.8% over the standard of care, corresponding to a 22.0% reduction for the 2.0g as compared to a 7.1% reduction for the standard of care. Also, after 8 weeks of treatment, patients treated with 4.0g for the entire 8 weeks showed statistically significant triglycerides, non-HDL-C and HbA1C mean improvements of, respectively, 14.4% and 9.8% and 15.0% as compared to standard of care. The 4.0g group mean improvements in (i) triglycerides of 14.4% corresponds to a reduction of 21.6% as compared to a reduction of a 7.1% for the standard of care group, (ii) non-HDL-C of 9.8% corresponds to a reduction of 12.0% as compared to a reduction of 2.3% for the standard of care group, and (iii) HbA1C of 15.0% corresponds to a reduction of 3.5% as compared to an increase of 11.5% for the standard of care group. In addition, all combined doses of CaPre® showed a statistically significant treatment effect on HDL-C levels, with an increase of 7.4% as compared to standard of care. Trends (p-value < 0.1) were also noted on patients treated with 4.0g of CaPre® for the entire 8-week treatment period with mean reduction of total cholesterol of 7.0% and increase of HDL-C levels of 7.7% as compared to the standard of care. Furthermore, after doubling the daily dosage of CaPre® after an initial period of 4 weeks, the results indicate a dose response relationship corresponding to a maintained and improved efficacy of CaPre® after an 8-week period. The efficacy of CaPre® at all doses in reducing triglyceride levels and increased effect with dose escalation suggests that CaPre® may be titrable, allowing physicians to adjust dosage in order to better manage patients’ medical needs. In addition, the results of the COLT trial indicate that CaPre® has no significant deleterious effect on LDL-C (bad cholesterol) levels.
Acasti presented the results of the COLT trial at two scientific forums, the National Lipid Association Scientific Session in the USA from May 1 to 4, and the 82nd Congress of European Atherosclerosis Society in Spain from May 31 to June 3. Acasti also presented at the World Congress of Heart Disease in Boston (July 25-28th, 2014).
TRIFECTA Trial
The TRIFECTA trial, a 12-week, randomized, placebo-controlled, double-blind, dose-ranging trial, is designed to assess the safety and efficacy of CaPre®, at a dose of 1.0 or 2.0g, on fasting plasma triglycerides as compared to a placebo in patients with mild to severe hypertriglyceridemia. A total of 387 patients were randomized and 365 patients completed the 12-week study, in line with the targeted number of evaluable patients. From this patient population, approximately 90% had mild to moderate hypertriglyceridemia with baseline triglycerides between 200 and 499 mg/dL (2.28 to 5.69 mmol/L). The remainder had very high baseline triglycerides between 500 and 877 mg/dL (> 5.7 and < 10 mmol/L). Approximately 30% of patients were on lipid lowering medications, such as statins, and approximately 10% were diabetic.
Similar to the COLT trial, the primary objective of the TRIFECTA trial is to evaluate the effect of CaPre® on fasting plasma triglycerides in patients with triglycerides between 2.28 and 10.0 mmol/L (200-877 mg/dL) and to assess the tolerability and safety of CaPre®. The secondary objectives of the TRIFECTA trial are to evaluate the effect of CaPre® on fasting plasma triglycerides in patients with triglycerides between 2.28 and 5.69 mmol/L (200-499 mg/dL); to evaluate the dose dependent effect on fasting plasma triglycerides in patients with triglycerides > 5.7 and <10 mmol/L (500-877 mg/dL); to evaluate the effect of CaPre® in patients with mild to moderate hypertriglyceridemia and severe hypertriglyceridemia on fasting plasma levels of LDL-C (direct measurement), and on fasting plasma levels of HDL-C, non-HDL-C, hs-CRP and omega-3 index.
On December 20, 2012, the TRIFECTA trial completed an interim analysis. The review committee made up of medical physicians assembled to evaluate the progress of the TRIFECTA trial reviewed the interim analysis relative to drug safety and efficacy and unanimously agreed that the study should continue as planned. All committee members agreed that there were no toxicity issues related to the intake of CaPre® and that the signals of a possible therapeutic effect, noted as reduction of triglycerides in the groups evaluated, were reassuring and sufficiently clinically significant to allow the further continuation of the TRIFECTA trial. The data was provided to the committee members blind, meaning that the identity of the three groups was not revealed. Since the data revealed a possible therapeutic effect without any safety concerns, the committee decided that it was not necessary to unblind the data. The number of targeted patients evaluable as per protocol has been reached. Acasti is currently evaluating efficacy and safety of CaPre® for the treatment of patients with mild to severe hypertriglyceridemia, which is the primary objective of the study. A secondary objective of the study was to assess the efficacy of CaPre® in two distinct patient populations: those with mild to moderate hypertriglyceridemia and those with severe hypertriglyceridemia. Based on patient information currently available, the Corporation does not expect the sample size to be large enough to conclude on the efficacy of CaPre® on severe hypertriglyceridemia as part of the TRIFECTA trial. Acasti does not expect the FDA to request efficacy data on patients with severe hypertriglyceridemia before granting permission to conduct a phase III trial.
44
On September 29, 2014, Acasti announced successful top-line results for its TRIFECTA trial assessing the safety and efficacy of CaPre® for the treatment of patients with hypertriglyceridemia.
CaPre® successfully met the trial’s primary endpoint achieving a statistically significant (p < 0.001) mean placebo-adjusted decrease in triglycerides from baseline to week-12, with reductions of 36.4% for 1 gram and 38.6% for 2 grams.
Along with material triglyceride reductions, all key secondary endpoints were met. This is a notable achievement as the trial was not designed to show a statistical significance on any other lipid than triglycerides. Nevertheless, there was a statistically significant decrease in non-HDL-C versus placebo (p=0.038), with the 2 gram per day CaPre® group decreasing by 5.3% from baseline versus placebo over the 12-week period. Non-HDL is considered the most accurate risk marker for cardiovascular disease.
CaPre® was also shown to have a slight increase in HDL-C (good cholesterol) at both the 1 gram and 2 gram levels and decrease in LDL-C (bad cholesterol) at 2 grams. As well, there was a clinically meaningful mean placebo-adjusted reduction in VLDL-C of 10.9% and 13.5% at 1 gram and 2 gram daily doses of CaPre®, respectively. VLDL-C is considered a highly significant predictor of coronary artery disease.
Finally, a statistically significant dose response increase in the Omega-3 Index for patients on 1 gram and 2 grams of CaPre® versus placebo was noted. The Omega-3 Index reflects the percentage of EPA and DHA in red blood cell fatty acids. The risk of cardiovascular disease is considered to be lower as the Omega-3 Index increases.
CaPre® was found to be safe and well tolerated at all doses tested, with no serious adverse events that were considered treatment related. Out of 387 randomized patients, a total of 7 (1.8%) were discontinued as a result of adverse events, three were on placebo, two were on 1 gram of CaPre® and two were on 2 grams of CaPre®. The predominant incidence was gastrointestinal related, with no difference between CaPre® and placebo. The safety profiles of patients on CaPre® and placebo were similar.
On March 2, 2015, the Corporation announced that it had received the full data for its TRIFECTA trial which confirmed and supported the positive Phase II TRIFECTA results announced in September 2014, on the safety and efficacy of CaPre® in the treatment of patients with hypertriglyceridemia. The TRIFECTA trial’s primary endpoint was met, with patients on 1 gram or 2 grams of CaPre® achieving a statistically significant mean placebo-adjusted decrease in triglycerides from baseline. In addition, benefits in other key cholesterol markers were announced, including slight increases in HDL-C (good cholesterol), no deleterious effect on LDL-C (bad cholesterol) and no safety concerns.
PK Trial
On November 11, 2013, the Corporation announced that it submitted an investigational new drug application to the FDA to initiate a PK trial of CaPre® in the United States. The PK trial was an open-label, randomized, multiple-dose, single-center, parallel-design study to evaluate blood profiles and bioavailability of omega-3 phospholipids on healthy volunteers taking single and multiple daily oral doses of 1.0g, 2.0g and 4.0g of CaPre®.
On January 9, 2014, the Corporation announced that the FDA granted Acasti approval to conduct its PK trial, having found no objections with the proposed PK trial design, protocol or safety profile of CaPre®. Acasti also announced that Quintiles, the world’s largest provider of biopharmaceutical development and commercial outsourcing services, has been hired to conduct the PK trial. On July 9, 2014, Acasti announced the completion of the PK trial.
On September 30, 2014, Acasti announced top-line results for its PK trial. The PK trial was an open-label, randomized, multiple-dose, single-center, parallel-design study in healthy volunteers. Forty-two male and female individuals, at least 18 years of age, were enrolled into three groups of 14 subjects who took 1, 2 or 4 grams of CaPre®, administered once a day 30 minutes after breakfast. The objectives of the study were to determine the pharmacokinetic profile and safety on Day 1 following a single oral dose and Day 14 following multiple oral doses of CaPre® on individuals pursuing a low-fat diet (therapeutic lifestyle changes diet). The effect of a high-fat meal on the bioavailability of CaPre® was also evaluated at Day 15. Blood samples were collected for assessment of EPA and DHA total lipids in plasma to derive the pharmacokinetic parameters.
CaPre® pharmacokinetics results appeared to be approximately dose proportional over the 1 to 4 gram a day dose range. Following a single daily dose, CaPre® reached steady state (EPA and DHA levels plateaued) within seven days of dosing. The bioavailability of CaPre® did not appear to be meaningfully affected by the fat content of the meal consumed prior to dose administration.
CaPre® demonstrated a near dose proportional increase with plasma EPA and DHA levels increasing as dose increases. The bioavailability of CaPre® was not significantly reduced when taken with a low-fat meal versus high-fat meal; a significant advantage for the management of hypertriglyceridemic patients on low fat diets . CaPre® was safe and well tolerated, with no safety concerns
45
Next Steps
Acasti has in hand its phase II clinical trial data and is now corresponding with the FDA to obtain its feedback about the next steps proposed for the clinical development plan of CaPre®. Such correspondence is meant to allow the FDA to provide its feedback on Acasti’s plans and to clarify or answer specific questions that the FDA may have prior to such next steps (including an end of phase II meeting, special protocol assessment and IND amendment) toward to the pivotal phase III clinical trial. Such correspondence can take the form of written correspondence, discussions and potential in person meetings with the FDA.
Acasti intends to conduct a phase III clinical trial in the United States, with potentially a few Canadian clinical trial sites, in a patient population with very high triglycerides (>500 mg/dL). In addition to conducting a Phase III clinical trial, Acasti expects that additional time and capital will be required to complete the filing of a NDA to obtain FDA approval for CaPre® in the United States before reaching commercialization, which may initially be only for the treatment of severe hypertriglyceridemia. The FDA may require Acasti to conduct additional clinical studies to obtain FDA approval for the treatment of mild to moderate hypertriglyceridemia, which may include a cardiovascular outcomes study.
Onemia®
During the year ended February 28, 2015, Acasti continued its business development and direct commercialization activities in the U.S. for its medical food Onemia®. Physicians initiated and/or continued their recommendations of Onemia® for patients diagnosed with cardiometabolic disorders. Acasti expects continued sales of Onemia® to provide short-term revenues that will contribute, in part, to finance Acasti’s research and development projects while establishing Acasti’s omega-3 phospholipids product credentials.
Additional Developments
On April 28, 2014, Acasti announced the resignation of Mr. Henri Harland as President and Chief Executive Officer of Acasti. Mr. Harland’s mandate as a Director of Acasti ended at the Annual and Special meeting of Shareholders held on June 19, 2014. Following Mr. Harland’s resignation, Acasti was managed on an interim basis by Mr. André Godin, the then Chief Financial Officer of Neptune.
On May 29, 2014, Neptune and its subsidiaries, including the Corporation, were served with a lawsuit from Mr. Henri Harland, former President and Chief Executive Officer of Neptune and its subsidiaries who resigned from all his duties on April 25, 2014. Mr. Harland alleges in his complaint that he was forced to resign and is claiming inter alia, the acknowledgment of the relevant sections of his employment contract, the payment of a sum of approximately $8,500,000 and the issuance of 500,000 shares of each Neptune, Acasti and NeuroBioPharm Inc. (“NeuroBioPharm”), as well as two blocks of 1,000,000 call-options each on the shares held by Neptune in Acasti and NeuroBioPharm in his name. Neptune and its subsidiaries believe the claim as formulated is without merit or cause. On December 11, 2014 Neptune, Acasti and NeuroBioPharm filed their defense and counterclaim alleging inter alia that Mr. Harland’s contract is null and void and that he is owed nothing following his resignation. Should the Court determine that the contract is nonetheless valid, Neptune and its subsidiaries’ position, as stated in the defense and counterclaim, is that there was also enough evidence discovered after Mr. Harland’s resignation that would have justified a dismissal for cause and that again, nothing is owed to the plaintiff. No trial date has been set. All outstanding share-based payments held by Mr. Harland have been cancelled during the year ended February 28, 2015. As of the date of this management discussion and analysis, no agreement has been reached and no provision has been recognized in the financial statements in respect of this claim. Neptune and its subsidiaries also filed an additional claim to recover certain amounts from Mr. Harland.
On June 16, 2014, Acasti announced the resignation of Xavier Harland as Chief Financial Officer of Acasti, whose functions were assumed on an interim basis by Mr. André Godin, the then Chief Financial Officer of Neptune.
In September 2014, Dr. Harlan W. Waksal, M.D. resigned as Executive Vice-President of the Corporation. He remains a director on the Corporation’s Board of Directors.
On November 7, 2014 Acasti received notification from the NASDAQ Listing Qualifications Department for failing to maintain a minimum bid price of US$1.00 per share for 30 consecutive business days. This notification had no immediate effect on the listing of Acasti’s shares as the Corporation had 180 calendar days to regain compliance. On May 11, 2015, Acasti received notification from NASDAQ that it was eligible for an additional 180 calendar days to regain compliance. To regain compliance, Acasti's shares must close at US$1.00 per share or more for a minimum of ten (10) consecutive business days. The Corporation is evaluating all available options to resolve the deficiency and regain compliance with the minimum bid price rule.
On April 29, 2015, Acasti announced the departure of Mr. André Godin from the Corporation. Following Mr. Godin’s departure, an executive search was initiated to fulfill his functions with Acasti.
46
Basis of presentation of the financial statements
The Corporation’s current assets of $19,642 as at February 28, 2015 include cash and short-term investments for an amount of $18,382, mainly generated by the net proceeds from the public and private offerings of common shares and warrants, completed on December 3, 2013 and February 7, 2014, respectively. The Corporation’s liabilities at February 28, 2015 are comprised primarily of amounts due creditors for $1,084, payable to parent corporation of $539 as well as derivative warrant liabilities of $2,357, which represents the fair value as of February 28, 2015, of the warrants issued to the Corporation’s public offering participants. The warrant liabilities will be settled in shares. The fair value of the Warrants issued was determined to be $0.58 per warrant upon issuance and $0.13 per warrant as at February 28, 2015. The fair value of the Warrants are revalued at each reporting date. Changes in the fair value of the Warrants are recognized in finance income or costs. The Warrants forming part of the Units are derivative liabilities (“Derivative warrant liabilities”) for accounting purposes due to the currency of the exercise price being different from the Corporation’s functional currency.
The Corporation is subject to a number of risks associated with the successful development of new products and their marketing, the conduct of its clinical studies and their results, the meeting of development objectives set by Neptune in its license agreement, and the establishment of strategic alliances. The Corporation has incurred significant operating losses and negative cash flows from operations since inception. To date, the Corporation has financed its operations through public offering and private placement of common shares, funds from its parent corporation, proceeds from exercises of warrants, rights and options and research tax credits. To achieve the objectives of its business plan, the Corporation plans to establish strategic alliances, raise the necessary capital and make sales. It is anticipated that the products developed by the Corporation will require approval from the U.S Food and Drug Administration and equivalent organizations in other countries before their sale can be authorized. The ability of the Corporation to ultimately achieve profitable operations is dependent on a number of factors outside of the Corporation’s control.
SELECTED FINANCIAL INFORMATION
(In thousands of dollars, except per share data)
| Three-month periods ended February 28, |
Years ended
|
|||||||||||||||||||||||
|
February 28,
|
February 28
|
February 28,
|
||||||||||||||||||||||
|
2015
|
2014
|
2013
|
2015
|
2014
|
2013
|
|||||||||||||||||||
| $ | $ | $ | $ | $ | $ | |||||||||||||||||||
|
Revenue from sales
|
178 | 201 | 49 | 271 | 501 | 724 | ||||||||||||||||||
|
Adjusted EBITDA(1)
|
(2,263 | ) | (977 | ) | (1,373 | ) | (8,506 | ) | (5,584 | ) | (4,397 | ) | ||||||||||||
|
Net loss and comprehensive loss
|
(2,311 | ) | (2,553 | ) | (1,952 | ) | (1,655 | ) | (11,612 | ) | (6,892 | ) | ||||||||||||
|
Basic and diluted loss per share
|
(0.02 | ) | (0.02 | ) | (0.03 | ) | (0.02 | ) | (0.14 | ) | (0.09 | ) | ||||||||||||
|
Total assets
|
37,208 | 45,632 | 12,170 | 37,208 | 45,632 | 12,170 | ||||||||||||||||||
|
Working capital(2)
|
18,020 | 24,646 | 3,413 | 18,020 | 24,646 | 3,413 | ||||||||||||||||||
|
Total non-current
|
||||||||||||||||||||||||
|
financial liabilities
|
2,357 | 11,181 | - | 2,357 | 11,181 | - | ||||||||||||||||||
|
Total equity
|
33,228 | 33,280 | 9,724 | 33,228 | 33,280 | 9,724 | ||||||||||||||||||
|
Book value per Class A share(3)
|
0.31 | 0.31 | 0.13 | 0.31 | 0.31 | 0.13 | ||||||||||||||||||
(1) The Adjusted EBITDA (Earnings Before Interest, Taxes, Depreciation and Amortization) is not a standard measure endorsed by IFRS requirements. A reconciliation to the Corporation’s net loss is presented below.
(2) The working capital is presented for information purposes only and represents a measurement of the Corporation’s short-term financial health mostly used in financial circles. The working capital is calculated by subtracting current liabilities from current assets. Because there is no standard method endorsed by IFRS requirements, the results may not be comparable to similar measurements presented by other public companies.
(3) The book value per share is presented for information purposes only and is obtained by dividing the shareholders’ equity by the number of outstanding Class A shares at the end of the period. Because there is no standard method endorsed by IFRS requirements, the results may not be comparable to similar measurements presented by other public companies.
RECONCILIATION OF THE ADJUSTED EARNINGS BEFORE INTEREST, TAXES, DEPRECIATION AND AMORTIZATION (ADJUSTED EBITDA)
A reconciliation of Adjusted EBITDA is presented in the table below. The Corporation uses adjusted financial measures to assess its operating performance. Securities regulations require that companies caution readers that earnings and other measures adjusted to a basis other than IFRS do not have standardized meanings and are unlikely to be comparable to similar measures used by other companies. Accordingly, they should not be considered in isolation. The Corporation uses Adjusted EBITDA to measure its performance from one period to the next without the variation caused by certain adjustments that could potentially distort the analysis of trends in our operating performance, and because the Corporation believes it provides meaningful information on the Corporation financial condition and operating results.
47
Acasti obtains its Adjusted EBITDA measurement by adding to net loss, finance costs, depreciation and amortization and income taxes and by subtracting finance income. Finance income/costs include foreign exchange gain (loss) and change in fair value of derivatives. Acasti also excludes the effects of certain non-monetary transactions recorded, such as stock-based compensation, from its Adjusted EBITDA calculation. The Corporation believes it is useful to exclude this item as it is a non-cash expense. Excluding this item does not imply it is necessarily nonrecurring.
RECONCILIATION OF ADJUSTED EBITDA
(In thousands of dollars, except per share data)
|
Three-month periods ended February 28,
|
Years ended February 28,
|
|||||||||||||||||||||||
|
2015
|
2014
|
2013
|
2015
|
2014
|
2013
|
|||||||||||||||||||
| $ | $ | $ | $ | $ | $ | |||||||||||||||||||
|
Net loss
|
(2,311 | ) | (2,553 | ) | (1,952 | ) | (1,655 | ) | (11,612 | ) | (6,892 | ) | ||||||||||||
|
Add (deduct)
|
||||||||||||||||||||||||
|
Finance costs
|
705 | 1,073 | 1 | 4 | 1,626 | 3 | ||||||||||||||||||
|
Finance Income
|
(1,398 | ) | (770 | ) | (41 | ) | (10,744 | ) | (814 | ) | (90 | ) | ||||||||||||
|
Depreciation and amortization
|
584 | 435 | 166 | 2,335 | 1,774 | 665 | ||||||||||||||||||
|
Stock-based compensation
|
157 | 838 | 453 | 1,554 | 3,442 | 1,917 | ||||||||||||||||||
|
Adjusted EBITDA
|
(2,263 | ) | (977 | ) | (1,373 | ) | (8,506 | ) | (5,584 | ) | (4,397 | ) | ||||||||||||
Finance costs for the three-month periods ended February 28, 2015 and 2014, as well as for the year ended February 28, 2014 include the change in the fair value of the derivative warrant liabilities in the amounts of $703, $507, and $507, respectively. The finance costs for the year ended February 28, 2014 also include warrant issue costs in the amount of $1,117. There were no expenses related to changes in fair values in the three-month period and year ended February 28, 2013 as the Corporation did not have any derivative warrant liabilities as at February 28, 2013.
Finance income for the year ended February 28, 2015 includes an unrealized gain in an amount of $8,824 for the change in fair value of the derivative warrant liabilities. The derivative warrant liability declined in fiscal 2015 due to the decline in the Corporation’s stock price resulting in a gain in earnings. Finance income also includes foreign exchange gains mainly on the Corporation’s short-term investments in US dollars, which represented $1,833, $782, and $43 for the years ended February 28, 2015, 2014 and 2013, respectively.
The yearly increase in the depreciation and amortization expense is attributable to the prepayment agreement entered into in December 2013, whereby Acasti recognized an intangible asset in the amount of $15,130. See section “Issuance of shares on license prepayment agreement”.
The increase of the stock-based compensation expense for the year ended February 28, 2014 is attributable to the 2012 grants. Stock-based compensation expense decreased in the year ended February 2015 as the 2012 grants are fully vested.
SELECTED QUARTERLY FINANCIAL DATA
(In thousands of dollars, except per share data)
Fiscal year ended February 28, 2015
|
First
|
Second
|
Third
|
Fourth
|
|||||||||||||||||
|
Total
|
Quarter
|
Quarter
|
Quarter
|
Quarter
|
||||||||||||||||
| $ | $ | $ | $ | $ | ||||||||||||||||
|
Revenue from sales
|
271 | 56 | 8 | 29 | 178 | |||||||||||||||
|
Adjusted EBITDA(1)
|
(8,506 | ) | (1,695 | ) | (2,449 | ) | (2,099 | ) | (2,263 | ) | ||||||||||
|
Net (loss) earnings
|
(1,655 | ) | 1,356 | (3,712 | ) | 3,012 | (2,311 | ) | ||||||||||||
|
Basic and diluted (loss) earnings per share
|
(0.02 | ) | 0.01 | (0.03 | ) | 0.03 | (0.02 | ) | ||||||||||||
48
The net earnings in the first and third quarters are mainly attributable to the gain resulting from the change in fair value of the derivative warrant liability of $4,634, and $5,211, respectively. In the second and fourth quarters the change in fair value of the derivative warrant liability was a loss of $318 and $703, respectively.
Fiscal year ended February 28, 2014
|
First
|
Second
|
Third
|
Fourth
|
|||||||||||||||||
|
Total
|
Quarter
|
Quarter
|
Quarter
|
Quarter
|
||||||||||||||||
| $ | $ | $ | $ | $ | ||||||||||||||||
|
Revenue from sales
|
501 | 6 | 266 | 28 | 201 | |||||||||||||||
|
Adjusted EBITDA(1)
|
(5,584 | ) | (1,270 | ) | (1,763 | ) | (1,574 | ) | (977 | ) | ||||||||||
|
Net loss
|
(11,612 | ) | (1,956 | ) | (3,238 | ) | (3,856 | ) | (2,553 | ) | ||||||||||
|
Basic and diluted loss per share
|
(0.14 | ) | (0.03 | ) | (0.04 | ) | (0.05 | ) | (0.02 | ) | ||||||||||
Fiscal year ended February 28, 2013
|
First
|
Second
|
Third
|
Fourth
|
|||||||||||||||||
|
Total
|
Quarter
|
Quarter
|
Quarter
|
Quarter
|
||||||||||||||||
| $ | $ | $ | $ | $ | ||||||||||||||||
|
Revenue from sales
|
724 | 14 | 237 | 424 | 49 | |||||||||||||||
|
Adjusted EBITDA(1)
|
(4,397 | ) | (923 | ) | (1,053 | ) | (1,048 | ) | (1,373 | ) | ||||||||||
|
Net loss
|
(6,892 | ) | (1,576 | ) | (1,752 | ) | (1,611 | ) | (1,953 | ) | ||||||||||
|
Basic and diluted loss per share
|
(0.09 | ) | (0.02 | ) | (0.02 | ) | (0.02 | ) | (0.03 | ) | ||||||||||
(1) The Adjusted EBITDA (Earnings Before Interest, Taxes, Depreciation and Amortization) is not a standard measure endorsed by IFRS requirements. A reconciliation to the Corporation’s net loss is presented above.
COMMENTS ON THE SIGNIFICANT VARIATIONS OF RESULTS FROM OPERATIONS FOR THE THREE-MONTH PERIODS AND YEARS ENDED FEBRUARY 28, 2015, 2014 AND 2013
Revenues
The Corporation generated revenues from sales of $178 from the commercialization of Onemia®, its medical food product, during the three-month period ended February 28, 2015. The Corporation generated revenue from sales of $201 and $49 during the corresponding periods in 2014 and 2013 respectively.
The Corporation generated revenues from sales of $271 from the commercialization of Onemia®, its medical food product, during the year ended February 28, 2015, a decrease of $230 from the revenues of $501 generated during corresponding period of 2014. The Corporation generated revenue from sales of $724 during the corresponding period of 2013. The revenues were generated from a distribution agreement the Corporation entered into with a US distributor specialized in medical food, as well as from sales made directly to customers in the United States. Acasti relies on a limited number of distributors / clients, therefore, revenues from sales may vary significantly period to period.
Gross Profit
Gross profit is calculated by deducting the cost of sales from revenue. Cost of sales consists primarily of costs incurred to manufacture products. It also includes related overheads, such as certain costs related to quality control and quality assurance, inventory management, sub-contractors and costs for servicing and commissioning.
The gross profit for the three-month period ended February 28, 2015 amounted to $(3) or (2)%. The Corporation realized a gross profit of $77 or 38% during the three-month period ended February 28, 2014 and $12 representing a gross profit margin of 24% during the three-month period ended February 28, 2013.
The gross profit for the year ended February 28, 2015 amounted to $36 or 13%. The Corporation realized a gross profit of $209 or 42% during the year ended February 28, 2014 and $318 representing a gross profit margin of 44% during the year ended February 28, 2013. The gross margin for the three-month period ended and year ended February 28, 2015 was lower than the Corporation’s target range for its profit margin because of the increased cost of raw material the Corporation incurred following Neptune’s interruption of production.
49
Breakdown of Major Components of the Statement of Earnings and Comprehensive Loss for the Three-month periods and years ended February 28, 2015, 2014 and 2013
|
General and administrative expenses
|
Three-month periods ended
|
Years ended
|
||||||||||||||||||||||
|
February 28, 2015
|
February 28, 2014
|
February 28, 2013
|
February 28, 2015
|
February 28, 2014
|
February 28, 2013
|
|||||||||||||||||||
| $ | $ | $ | $ | $ | $ | |||||||||||||||||||
|
Salaries and benefits
|
280 | 323 | 158 | 1,267 | 990 | 912 | ||||||||||||||||||
|
Stock-based
|
||||||||||||||||||||||||
|
compensation
|
118 | 641 | 327 | 1,296 | 2,841 | 1,462 | ||||||||||||||||||
|
Professional fees
|
54 | 98 | 231 | 302 | 492 | 527 | ||||||||||||||||||
|
Royalties
|
- | - | 173 | - | 228 | 450 | ||||||||||||||||||
|
Amortization and
|
||||||||||||||||||||||||
|
depreciation
|
584 | 435 | 166 | 2,335 | 1,774 | 665 | ||||||||||||||||||
|
Sales and marketing
|
14 | 2 | 11 | 29 | 16 | 131 | ||||||||||||||||||
|
Investor relations
|
48 | 54 | 4 | 262 | 188 | 31 | ||||||||||||||||||
|
Rent
|
25 | 25 | 9 | 99 | 100 | 54 | ||||||||||||||||||
|
Other
|
127 | 36 | 8 | 318 | 83 | 57 | ||||||||||||||||||
|
TOTAL
|
1,614 | 1,614 | 1,087 | 5,908 | 6,712 | 4,289 | ||||||||||||||||||
|
Research and development expenses
|
Three-month periods ended
|
Years ended
|
||||||||||||||||||||||
|
February 28, 2015
|
February 28, 2014
|
February 28, 2013
|
February 28, 2015
|
February 28, 2014
|
February 28, 2013
|
|||||||||||||||||||
| $ | $ | $ | $ | $ | $ | |||||||||||||||||||
|
Salaries and benefits
|
86 | 54 | 163 | 465 | 457 | 684 | ||||||||||||||||||
|
Stock-based compensation
|
39 | 197 | 126 | 258 | 601 | 455 | ||||||||||||||||||
|
Contracts
|
1,463 | 503 | 816 | 5,062 | 3,081 | 2,030 | ||||||||||||||||||
|
Regulatory expenses
|
83 | 32 | 1 | 160 | 141 | 68 | ||||||||||||||||||
|
Professional fees
|
220 | 35 | 6 | 709 | 214 | 67 | ||||||||||||||||||
|
Other
|
52 | 11 | 18 | 133 | 73 | 75 | ||||||||||||||||||
|
Tax credits
|
(192 | ) | (118 | ) | (212 | ) | (265 | ) | (270 | ) | (370 | ) | ||||||||||||
|
TOTAL
|
1,751 | 714 | 918 | 6,522 | 4,297 | 3,009 | ||||||||||||||||||
Adjusted Earnings before Interest, Taxes, Depreciation and Amortization (Adjusted EBITDA)
Adjusted EBITDA decreased by $1,286 for the three-month period ended February 28, 2015 to $(2,263) compared to $(977)
for the three-month period ended February 28, 2014, mainly due to the increase in research and development expenses before consideration of stock-based compensation as well as to a decrease in gross profit. The increase in research and development expenses of $1,037 is mainly attributable to increases in contract expenses of $960 and professional fees related to the Corporation’s clinical trials of $185.
Adjusted EBITDA increased by $396 for the three-month period ended February 28, 2014 to $(977) compared to $(1,373) for the three-month period ended February 28, 2013, mainly due to the decrease in general and administrative and research and development expenses before consideration of stock-based compensation and amortization and depreciation as well as due to an increase in gross profit. The decrease in general and administrative expenses is mainly attributable to decreases in professional fees and royalties, offset by an increase in salaries and benefits. The decrease in research and development expenses of $204 is mainly attributable to decreases in salaries and benefits of $109 and contract expenses of $313 related to the Corporation’s clinical trials and regulatory expenses.
Adjusted EBITDA decreased by $2,922 for the year ended February 28, 2015 to $(8,506) compared to $(5,584) for the year ended February 28, 2014, mainly due to the increase in research and development expenses, before consideration of stock-based compensation and decrease in gross profit. The increase in research and development expenses of $2,225 is mainly attributable to increases in contract expenses of $1,981 and professional fees related to the Corporation’s clinical trials of $495.
Adjusted EBITDA decreased by $1,187 for the year ended February 28, 2014 to $(5,584) compared to $(4,397) for the year ended February 28, 2013, mainly due to the increase in research and development expenses, before consideration of stock-based compensation and amortization and depreciation, and decrease in gross profit. The increase in research and development expenses of $1,288 is mainly attributable to increases in contract expenses of $1,051 related to the Corporation’s clinical trials.
50
Net Loss
The Corporation realized a net loss for the three-month period ended February 28, 2015 of $2,311 or $0.02 per share compared to a net loss of $2,553 or $0.02 per share for the three-month period ended February 28, 2014. These results are mainly attributable to the factors described above in the Gross Profit and Adjusted EBITDA sections as well as by increases in amortization and depreciation, following the increase in the Corporation’s license asset as a result of the prepayment agreement with Neptune, and the increase in value of the derivative warrant liabilities of $703, principally offset by a decrease in stock-based compensation expenses of $681.
The Corporation realized a net loss for the three-month period ended February 28, 2014 of $2,553 or $0.02 per share compared to a net loss of $1,952 or $0.03 per share for the three-month period ended February 28, 2013. These results are mainly attributable to the factors described above in the Gross Profit and Adjusted EBITDA sections as well as by increases in amortization and depreciation, following the increase in the Corporation’s license asset as a result of the prepayment agreement with Neptune, stock-based compensation expenses, related to the grant of stock options and restricted share units, and finance costs related to the Corporation’s financing closed on December 3, 2013 and the increase in value of the derivative warrant liabilities, principally offset by the foreign exchange gain over the period.
The Corporation realized a net loss for the year ended February 28, 2015 of $1,655 or $0.02 per share compared to a net loss of $11,612 or $0.14 per share for the year ended February 28, 2014. These results are mainly attributable to the factors described above in the Gross Profit and Adjusted EBITDA sections as well as by the decrease in value of the derivative warrant liabilities of $8,824 compared to an increase of $507 in prior period, an increase in the foreign exchange gain over the prior period by $1,051 and a decrease in stock-based compensation expenses of $1,888, offset by increases in amortization and depreciation of $561, following the increase in the Corporation’s license asset as a result of the prepayment agreement with Neptune. The foreign exchange gain is due mainly to the strengthening US dollar impact on the Corporation’s US dollar short-term investments. Stock-based compensation decreased as grants provided in 2012 are fully vested.
The Corporation realized a net loss for the year ended February 28, 2014 of $11,612 or $0.14 per share compared to a net loss of $6,892 or $0.09 per share for the year ended February 28, 2013. These results are mainly attributable to the factors described above in the Gross Profit and Adjusted EBITDA sections as well as by increases in amortization and depreciation, following the increase in the Corporation’s license asset as a result of the prepayment agreement with Neptune, stock based compensation expenses related to the grant of stock options and restricted share units, finance costs related to the Corporation’s financing that closed on December 3, 2013 and the increase in value of the derivative warrant liabilities, principally offset by the foreign exchange gain mainly on the Corporation’s US dollar short-term investments over the period.
LIQUIDITY AND CAPITAL RESOURCES
Share Capital Structure
The authorized share capital consists of an unlimited number of Class A, Class B, Class C, Class D and Class E shares, without par value. Issued and outstanding fully paid shares, stock options, restricted shares units and warrants, were as follows as at February 28:
|
2015
|
2014
|
2013
|
||||||||||
|
Class A shares, voting, participating and without par value
|
106,444,012 | 105,862,179 | 73,107,538 | |||||||||
|
Stock options granted and outstanding
|
4,296,250 | 4,911,000 | 5,216,250 | |||||||||
|
Restricted Shares Units granted and outstanding
|
184,000 | 775,001 | - | |||||||||
|
Series 4 warrants expired on
|
||||||||||||
|
October 8, 2013
|
- | - | 5,432,350 | |||||||||
|
Series 6 & 7 warrants expired on February 10, 2015
|
- | 750,000 | 750,000 | |||||||||
|
Series 8 warrants exercisable at $1.50 USD, until
|
||||||||||||
|
December 3, 2018
|
18,400,000 | 18,400,000 | - | |||||||||
|
Series 9 warrants exercisable at $1.60, until
|
||||||||||||
|
December 3, 2018
|
1,616,542 | 1,616,542 | - | |||||||||
|
Total fully diluted shares
|
130,940,804 | 132,314,722 | 84,506,138 | |||||||||
51
Cash Flows and Financial Condition between the Three-month periods and years ended February 28, 2015, 2014 and 2013
Operating Activities
During the three-month periods ended February 28, 2015, 2014 and 2013, the Corporation’s activities generated decreases in liquidities of $2,622 and $4,723, and an increase of $60, respectively. The decrease in the cash flows from operating activities for the three-month period ended February 28, 2015 and 2014 is mainly attributable to the changes in non-cash working capital items, primarily by increases in trade and other receivables of $447, and prepaid expenses of $377, and decreases in trade and other payables of $428, payable to parent corporation of $2,490, and royalties payable to parent corporation of $337, offset by a decrease in tax credits receivable of $353. The increase in the cash flows from operating activities for the three-month period ended February 28, 2013 is mainly attributable to the net loss incurred after adjustments for non-cash items, offset by changes in non-cash working capital.
During the years ended February 28, 2015, 2014 and 2013, the Corporation’s operating activities resulted in decreases in liquidities of $7,198, $6,805 and $2,549 respectively. The decrease in the cash flows from operating activities for the year ended February 28, 2015 is mainly attributable to the higher loss from operating activities after adjustments for non-cash items offset by the changes in non-cash working capital items, primarily by decreases in trade and other receivables of $534 and prepaid expenses of $385, and an increase in payable to parent corporation of $539. The decrease in cash flows from operating activities for the year ended February 28, 2014 is mainly attributable to the net loss incurred after adjustments for non-cash items offet by changes in non-cash working capital, primarily by increases in trade and other receivables of $469 and prepaid expenses of $687, and decrease in payable to parent corporation of $417, offset by a decrease in tax credits receivable of $201 and an increase in trade and other payables of $464. The decrease in cash flows from operating activities for the year ended February 28, 2013 is mainly attributable to the net loss incurred after adjustments for non-cash items offset by changes in non-cash working capital, primarily increases in payable to parent corporation of $995 and royalties payable to parent corporation of $480.
Investing Activities
During the three-month periods ended February 28, 2015, 2014 and 2013, the Corporation’s investing activities generated an increase in liquidities of $2,000, a decrease in liquidities of $22,202 and an increase in liquidities of $168, respectively. The increase in liquidity generated by investing activities during the three-month period ended February 28, 2015 is mainly due to the maturity of short-term investments of $2,000. The decrease in liquidity generated by investing activities during the three-month period ended February 28, 2014 is mainly due to the acquisition of short-term investments of $22,396, principally offset by the maturity of short-term investments of $250. The increase in liquidity generated by investing activities during the three-month period ended February 28, 2013 is mainly due to the maturity of short-term investments of $250 offset by the acquisition of short-term investments of $83.
During the years ended February 28, 2015, 2014 and 2013, the Corporation’s investing activities generated an increase in liquidities of $7,627, a decrease in liquidities of $19,446 and an increase in liquidities of $1,899, respectively. The increase in liquidity generated by investing activities during the year ended February 28, 2015 is mainly due to the maturity of short-term investment of $22,150, principally offset by the acquisition of short-term investments of $14,478. The decrease in liquidity generated by investing activities during the year ended February 28, 2014 is mainly due to the acquisition of short-term investments of $25,396, principally offset by the maturity of short-term investments of $6,000. The increase in liquidity generated by investing activities during the year ended February 28, 2013 is mainly due to the maturity of short-term investments of $2,000 offset by the acquisition of short-term investments of $103.
Financing Activities
During the three-month periods ended February 28, 2015, 2014 and 2013, the Corporation’s financing activities generated decreases in liquidities of $1, increases in liquidities of $24,023 and increases in liquidities of $185, respectively. The increase in liquidities generated from financing activity during the three-month periods ended February 28, 2014 resulted mainly from the net proceeds from a public offering of $21,953 and net proceeds from a private placement of $2,068. As indicated in the Corporation’s Prospectus Supplement, the Corporation’s primary use of the net proceeds received from the public offering is to finance the Phase III clinical trials for CaPre®, the PK trial, the completion and filing of a NDA to obtain FDA approval for CaPre® in the United States, to complete marketing and precommercialization activities and for general and administrative matters. The increase in liquidities generated from financing activity during the three-month period ended February 28, 2013 resulted mainly from the proceeds from exercise of warrants and options of $185.
During the years ended February 28, 2015, 2014 and 2013, the Corporation’s financing activities generated increases in liquidities of $46, $24,963 and $227, respectively. The increase in liquidities generated from financing activity during the year ended February 28, 2015 resulted mainly from the proceeds from exercise of warrants and options of $50. The increase in liquidities generated from financing activity during the year ended February 28, 2014 resulted mainly from the net proceeds from a public offering of $21,953, net proceeds from a private placement of $2,068 and proceeds from exercise of warrants and options of $972. The increase in liquidities generated from financing activity during the year ended February 28, 2013 resulted mainly from the proceeds from exercise of warrants and options of $230.
52
Overall, as a result, the Corporation’s cash increased by $635, decreased by $521 and decreased by $393, respectively, for the years ended February 28, 2015, 2014 and 2013. Total liquidities as at February 28, 2015, comprised of cash and short-term investments, amounted to $18,382. See basis of presentation for additional discussion of the Corporation’s financial condition.
To date, the Corporation has financed its operations through public offering and private placement of common shares, funds from its parent corporation, proceeds from the exercise of warrants, rights and options and research tax credits. The future profitability of the Corporation is dependent upon such factors as the success of the clinical trials, the approval by regulatory authorities of products developed by the Corporation, the ability of the Corporation to successfully market and sell and distribute products and the ability to obtain the necessary financing to do so. The Corporation believes that its available cash and short-term investments, expected interest income and research tax credits should be sufficient to finance the Corporation’s operations and capital needs during the ensuing twelve-month period.
Financial Position
The following table details the significant changes to the statements of financial position as at February 28, 2015 compared to February 28, 2014:
|
Accounts
|
Increase
(Decrease)
|
Comments
|
|||
|
Cash
|
635 |
See cash flow statement
|
|||
|
Short-term investments
|
5,955 |
Maturity of investments held
|
|||
|
Trade and other receivables
|
(534 | ) |
Payments received
|
||
|
Tax credits receivable
|
286 |
Increase in tax credit eligible expenses
|
|||
|
Prepaid expenses
|
(385 | ) |
Decrease in prepaid expenses to Neptune
|
||
|
Inventories
|
(174 | ) |
Onemia® sales
|
||
|
Intangible assets
|
(2,280 | ) |
Amortization
|
||
|
Payable to parent corporation
|
539 |
Increase in expenses
|
|||
|
Derivative warrant liabilities
|
(8,825 | ) |
Change in fair value
|
||
Issuance of shares on license prepayment agreement
On July 12, 2013, the Corporation issued 6,750,000 Class A shares, at a price of $2.30 per share to Neptune to pay in advance all of the future royalties’ payable under the intellectual property license it had with Neptune.
The value of the prepayment, determined with the assistance of outside valuations specialists, using the pre-established formula set forth in the license agreement (adjusted to reflect the royalties of $395 accrued from December 4, 2012, the date at which the Corporation entered into the prepayment agreement to July 12, 2013, the date of issuance of the shares) totalling $15,130, was recognized as an intangible asset. The shares issued as a result of this transaction corresponded to an increase in share capital of $15,525, net of $29 of share issue costs. The Corporation no longer has a royalty payment commitment under the License Agreement.
Contractual Obligations, Off-Balance-Sheet Arrangements and Commitments
The Corporation has no off-balance sheet arrangements. As of February 28, 2015, the Corporation’s liabilities are $3,980, of which $1,622 is due within twelve months and $2,358 relates to a derivative warrant liability that will be settled in shares and thus is excluded from the table below.
A summary of Acasti’s contractual obligations at February 28, 2015 is as follows:
|
Total
|
Less than 1 year
|
1 – 3 years
|
3 – 5 years
|
Greater than 5 years
|
||||||||||||||||
| $ | $ | $ | $ | $ | ||||||||||||||||
|
Payables
|
1,622 | 1,622 | - | - | - | |||||||||||||||
|
Research and development contracts
|
3,831 | 2,580 | 1,251 | - | - | |||||||||||||||
|
Total
|
5,453 | 4,202 | 1,251 | - | - | |||||||||||||||
Significant commitments as of February 28, 2015 include:
53
Research and development agreements
In the normal course of business, the Corporation has signed agreements with various partners and suppliers for them to execute research projects and to produce and market certain products.
The Corporation initiated research and development projects that will be conducted over a 12 to 24 month period for a total initial cost of $10,562, of which an amount of $6,299 has been paid to date. As at February 28, 2015, an amount of $432 is included in ‘‘Trade and other payables’’ in relation to these projects.
Related Party Transactions
The Corporation was charged by Neptune for certain costs incurred by Neptune for the benefit of the Corporation and for royalties, as follows:
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Administrative costs
|
1,617 | 1,038 | 943 | |||||||||
|
Research and development costs, before tax credits
|
681 | 546 | 679 | |||||||||
|
Royalties1
|
- | 228 | 450 | |||||||||
|
Total fully diluted shares
|
2,298 | 1,812 | 2,072 | |||||||||
1 Refer to Issuance of shares on license prepayment agreement section above.
Where Neptune incurs specific incremental costs for the benefit of the Corporation, it charges those amounts directly. Costs that benefit more than one entity of the Neptune group are charged by allocating a fraction of costs incurred by Neptune that is commensurate to the estimated fraction of services or benefits received by each entity for those items. These charges do not represent all charges incurred by Neptune that may have benefited the Corporation, because, amongst others, Neptune does not allocate certain common office expenses and does not charge interest on indebtedness. Also, these charges do not necessarily represent the cost that the Corporation would otherwise need to incur, should it not receive these services or benefits through the shared resources of Neptune or receive financing from Neptune.
Payable to parent corporation has no specified maturity date for payment or reimbursement and does not bear interest.
The key management personnel of the Corporation are the members of the Board of Directors and certain officers. They control 2% of the voting shares of the Corporation. See note 5 to the financial statements for disclosures of key management personnel compensation.
Use of estimates and measurement of uncertainty
The preparation of the financial statements in conformity with IFRS requires management to make judgments, estimates and assumptions that affect the application of accounting policies and the reported amounts of assets, liabilities, income and expenses. Actual results may differ from these estimates. Estimates are based on the management’s best knowledge of current events and actions that the Corporation may undertake in the future. Estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimates are revised and in any future periods affected. Critical judgments in applying accounting policies that have the most significant effect on the amounts recognized in the financial statements include the identification of triggering events indicating that intangible assets might be impaired and the use of the going concern basis of preparation of the financial statements. At each reporting period, management assesses the basis of preparation of the financial statements. The financial statements have been prepared on a going concern basis in accordance with IFRS. The going concern basis of presentation assumes that the Corporation will continue its operations for the foreseeable future and be able to realize its assets and discharge its liabilities and commitments in the normal course of business. Assumptions and estimation uncertainties that have a significant risk of resulting in a material adjustment within the next financial year include allocation of shared costs amongst the Neptune group companies (See Related Party Transactions section above) and the measurement derivative warrant liabilities (note 19 to the financial statements) and of stock-based compensation (note 14 to the financial statements). Also, the management uses judgment to determine which research and development (“R&D”) expenses qualify for R&D tax credits and in what amounts. The Corporation recognizes the tax credits once it has reasonable assurance that they will be realized. Recorded tax credits are subject to review and approval by tax authorities and therefore, could be different from the amounts recorded.
54
Critical Accounting Policies
Impairment of non-financial assets
The carrying value of the Corporation’s license asset is reviewed at each reporting date to determine whether there is any indication of impairment. If any such indication exists, then the asset’s recoverable amount is estimated. The identification of impairment indicators and the estimation of recoverable amounts require the use of judgment.
Derivative warrant liabilities
The warrants forming part of the Units issued from the prior year’s public offering are derivative liabilities for accounting purposes due to the currency of the exercise price being different from the Corporation’s functional currency. The derivative warrant liabilities are required to be measure at fair value at each reporting date with changes in fair value recognized in earnings. The Corporation’s uses Black-Scholes pricing model to determine the fair value. The model requires the assumption of future stock price volatility, which is estimated based on weighted average historic volatility. Changes to the expected volatility could cause significant variations in the estimated fair value of the derivative warrant liabilities.
Stock-based compensation
The Corporation has a stock-based compensation plan, which is described in note 14 of the financial statements. The Corporation accounts for stock options granted to employees based on the fair value method, with fair value determined using the Black-Scholes model. The Black Scholes model requires certain assumptions such as future stock price volatility and expected life of the instrument. Expected volatility is estimated based on weighted average historic volatility. The expected life of the instrument is estimated based on historical experience and general holder behavior. Under the fair value method, compensation cost is measured at fair value at date of grant and is expensed over the award’s vesting period with a corresponding increase in contributed surplus. For stock options granted to non-employees, the Corporation measures based on the fair value of services received, unless those are not reliably estimable, in which case the Corporation measures the fair value of the equity instruments granted. Compensation cost is measured when the company obtains the goods or the counterparty renders the service.
Also, the Corporation records as stock-based compensation expense a portion of the expense being recorded by Neptune that is commensurate to the fraction of overall services that the grantees provide directly to the Corporation with the offset to contributed surplus reflecting Neptune’s contribution to the Corporation.
Tax credits
Tax credits related to eligible expenses are accounted for as a reduction of related costs in the year during which the expenses are incurred as long as there is reasonable assurance of their realization.
Future Accounting change
New standards and interpretations not yet adopted:
Financial instruments:
On July 24, 2014, the International Accounting Standards Board (IASB) issued the final version of IFRS 9, Financial Instruments, which addresses the classification and measurement of financial assets and liabilities, impairment and hedge accounting, replacing IAS 39, Financial Instruments: Recognition and Measurement. IFRS 9 is effective for annual periods beginning on or after January 1, 2018, with earlier adoption permitted. The Corporation has not yet assessed the impact of adoption of IFRS 9, and does not intend to early adopt IFRS 9 in its financial statements.
Revenue:
On May 28, 2014 the IASB issued IFRS 15, Revenue from Contracts with Customers. IFRS 15 will replace IAS 18, Revenue, among other standards. The standard contains a single model that applies to contracts with customers and two approaches to recognizing revenue: at a point in time or over time. The model features a contract-based five-step analysis of transactions to determine whether, how much and when revenue is recognized. New estimates and judgmental thresholds have been introduced, which may affect the amount and/or timing of revenue recognized. The new standard applies to contracts with customers. The new standard is effective for annual periods beginning on or after January 1, 2018, with earlier adoption permitted. The Corporation has not yet assessed the impact of adoption of IFRS 15, and does not intend to early adopt IFRS 15 in its financial statements.
Financial Instruments
Credit Risk
Credit risk is the risk of a loss if a customer or counterparty to a financial asset fails to meet its contractual obligations, and arises primarily from the Corporation’s trade receivables. The Corporation may also have credit risk relating to cash and short-term investments, which it manages by dealing only with highly-rated Canadian institutions. The carrying amount of financial assets, as disclosed in the statements of financial position, represents the Corporation’s credit exposure at the reporting date. The Corporation’s trade receivables and credit exposure fluctuate throughout the year. The Corporation’s average trade receivables and credit exposure during the year may be higher than the balance at the end of that reporting year.
55
The Corporation’s credit risk for trade receivables is concentrated, as the majority of its sales are to one customer. As at February 28, 2015, the Corporation has one trade debtor (eight in 2014). Most sales' payment terms are set in accordance with industry practice. One customer represents 100% of total trade accounts included in trade and other receivables as at February 28, 2015 and February 28, 2014.
Most of the Corporation's customers are distributors for a given territory and are privately-held enterprises. The profile and credit quality of the Corporation’s retail customers vary significantly. Adverse changes in a customer’s financial position could cause the Corporation to limit or discontinue conducting business with that customer, require the Corporation to assume more credit risk relating to that customer’s future purchases or result in uncollectible accounts receivable from that customer. Such changes could have a material adverse effect on business, results of operations, financial condition and cash flows.
Customers do not provide collateral in exchange for credit, except in unusual circumstances. Receivables from selected customers are covered by credit insurance, with coverage amount usually of 100% of the invoicing, with the exception of some customers under specific terms. The information available through the insurers is the main element in the decision process to determine the credit limits assigned to customers.
The Corporation’s extension of credit to customers involves considerable judgment and is based on an evaluation of each customer’s financial condition and payment history. The Corporation has established various internal controls designed to mitigate credit risk, including a credit analysis by the insurer which recommends customers' credit limits and payment terms that are reviewed and approved by the Corporation. The Corporation reviews periodically the insurer's maximum credit quotation for each of its clients. New clients are subject to the same process as regular clients. The Corporation has also established procedures to obtain approval by senior management to release goods for shipment when customers have fully-utilized approved insurers credit limits. From time to time, the Corporation will temporarily transact with customers on a prepayment basis where circumstances warrant.
While the Corporation’s credit controls and processes have been effective in mitigating credit risk, these controls cannot eliminate credit risk and there can be no assurance that these controls will continue to be effective, or that the Corporation’s low credit loss experience will continue.
The Corporation provides for trade receivables their expected realizable value as soon as the account is determined not to be fully collectible, with such write-offs charged to earnings unless the loss has been provided for in prior years, in which case the write-off is applied to reduce the allowance for doubtful accounts. The Corporation updates its estimate of the allowance for doubtful accounts, based on evaluations of the collectability of trade receivable balances at each reporting date, taking into account amounts which are past due, and any available information indicating that a customer could be experiencing liquidity or going concern problems.
The aging of trade receivable balances and the allowance for doubtful accounts as at February 28, 2015 and 2014 were as follows:
|
2015
|
2014
|
|||||||
|
Current
|
$ | - | $ | 196 | ||||
|
Past due 0-30 days
|
227 | - | ||||||
|
Past due 31-120 days
|
- | 24 | ||||||
|
Past due 121-180 days
|
89 | 178 | ||||||
|
Trade receivables
|
316 | 398 | ||||||
|
Less allowance for doubtful accounts
|
(66 | ) | (3 | ) | ||||
| $ | 250 | $ | 395 | |||||
The allowance for doubtful accounts is for customer accounts over 121 days past due.
During the year ended February 28, 2015, the Corporation recorded a bad debt expense of $63 (2014 - nil) related to one significant customer, for which total trade receivable due at February 28, 2015 is $316.
The movement in allowance for doubtful accounts in respect of trade receivables was as follows:
|
2015
|
2014
|
|||||||
|
Balance, beginning of year
|
$ | 3 | $ | 3 | ||||
|
Bad debts expenses
|
66 | - | ||||||
|
Write-off against reserve
|
(3 | ) | - | |||||
|
Balance, end of year
|
$ | 66 | $ | 3 | ||||
56
Currency risk
The Corporation is exposed to the financial risk related to the fluctuation of foreign exchange rates and the degrees of volatility of those rates. Foreign currency risk is limited to the portion of the Corporation's business transactions denominated in currencies other than the Canadian dollar. Fluctuations related to foreign exchange rates could cause unforeseen fluctuations in the Corporation's operating results.
All of the Corporation’s revenues are in US dollars. A portion of the expenses, mainly related to research contracts, is made in US dollars. There is a financial risk involved related to the fluctuation in the value of the US dollar in relation to the Canadian dollar.
The following table provides an indication of the Corporation’s significant foreign exchange currency exposures as stated in Canadian dollars at the following dates:
|
February 28, 2015
|
February 28, 2014
|
|||||||
|
US$
|
US$
|
|||||||
|
Cash
|
1,103 | 361 | ||||||
|
Short-term investments
|
15,007 | 15,505 | ||||||
|
Trade and other receivables
|
250 | 398 | ||||||
|
Trade and other payables
|
(399 | ) | (260 | ) | ||||
| 15,961 | 16,004 | |||||||
The following exchange rates are those applicable to the following periods and dates:
|
February 28,
|
February 28,
|
|||||||||||||||
|
2015
|
2014
|
|||||||||||||||
|
Average
|
Reporting
|
Average
|
Reporting
|
|||||||||||||
|
US$ per CAD
|
1.1266 | 1.2503 | 1.0466 | 1.1074 | ||||||||||||
Based on the Corporation’s foreign currency exposures noted above, varying the above foreign exchange rates to reflect a 5% strengthening of the US dollar would have increased the net profit as follows, assuming that all other variables remained constant:
|
February 28,
|
February 28,
|
|||||||
|
2015
|
2014
|
|||||||
|
US$
|
US$
|
|||||||
|
Increase in net profit
|
638 | 723 | ||||||
An assumed 5% weakening of the foreign currency would have had an equal but opposite effect on the basis that all other variables remained constant.
Interest rate risk
Interest rate risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market rates.
The Corporation’s exposure to interest rate risk as at February 28, 2015 and 2014 is as follows:
|
Cash
|
Short-term fixed interest rate
|
|
Short-term investments
|
Short-term fixed interest rate
|
The capacity of the Corporation to reinvest the short-term amounts with equivalent return will be impacted by variations in short-term fixed interest rates available on the market. Management believes that the risk that the Corporation will realize a loss as a result of the decline in the fair value of its short-term investments is limited because these investments have short-term liabilities and are generally held to maturity.
57
Liquidity risk
Liquidity risk is the risk that the Corporation will not be able to meet its financial obligations as they fall due. The Corporation manages liquidity risk through the management of its capital structure and financial leverage, as outlined in Note 20 to the financial statements. It also manages liquidity risk by continuously monitoring actual and projected cash flows. The Board of Directors reviews and approves the Corporation's operating budgets, and reviews the most important material transactions outside the normal course of business.
The following are the contractual maturities of financial liabilities as at February 28, 2015 and 2014:
|
February 28, 2015
|
||||||||||||||||||||
|
Required payments per year
|
Carrying
|
Less than
|
1 to
|
More than
|
||||||||||||||||
|
Total
|
amount
|
1 year
|
5 years
|
5 years
|
||||||||||||||||
|
Trade and other payables
|
$ | 1,084 | $ | 1,084 | $ | 1,084 | $ | - | $ | - | ||||||||||
|
Payable to parent corporation
|
538 | 538 | 538 | - | - | |||||||||||||||
| $ | 1,622 | $ | 1,622 | $ | 1,622 | $ | - | $ | - | |||||||||||
|
February 28, 2014
|
||||||||||||||||||||
|
Required payments per year
|
Total
|
Carrying
|
Less than
|
1 to
|
More than
|
|||||||||||||||
|
amount
|
1 year
|
5 years
|
5 years
|
|||||||||||||||||
|
Trade and other payables
|
$ | 1,171 | $ | 1,171 | $ | 1,171 | $ | - | $ | - | ||||||||||
The Derivative warrant liabilities are excluded from the above table as they will be settled in shares and not by the use of liquidities.
As at May 27, 2015, the total number of Class A shares of the Corporation issued and outstanding was 106,444,012. The
Corporation also has 4,213,750 stock options, 181,000 restricted shares units, 20,016,542 Series 8 & 9 warrants.
|
Item 6.
|
Directors, Senior Management and Employees
|
|
A.
|
Directors and Senior Management
|
Nominees for Election as Director
The following table sets out the name and the province and country of residence of each of the persons proposed for election as Directors in the Corporation’s proxy circular dated June 15, 2015, and all other positions and offices with the Corporation held by such person, his or her principal occupation, the year in which the person became a director of the Corporation, and the number of Common Shares of the Corporation that such person has declared to beneficially own, directly or indirectly, or over which control or direction is exercised by such person as at the date indicated below.
58
|
Name, province and country of residence of each director and proposed director
|
Principal Occupation
|
First year as director
|
Number of Common Shares beneficially owned or controlled or directed by each proposed director
|
|
Jerald J. Wenker
California, United States
Chairman of the Board
|
President and Chief Operating Officer, Dermalogica
|
2014
|
2,500
|
|
Roderick Carter
California, United States
|
Principal at Aquila Life Sciences LLC
|
-
|
-
|
|
Jim Hamilton
New Jersey, United States
|
President and CEO of Neptune
|
-
|
-
|
|
Adrian Montgomery
Ontario, Canada
|
President of Tuckamore Capital
|
2014
|
-
|
|
Reed V. Tuckson
Washington, United States
Director
|
Managing Director, Tuckson Health Connections, LLC
|
2013
|
7,299
|
|
Harlan W. Waksal
New York, United States
Director
|
President & Chief Executive Officer of Kadmon Corporation LLC
|
2013
|
873,700
|
The information as to the number of Common Shares beneficially owned or over which the above-named individuals exercise control or direction and the foregoing information, is not within the knowledge of the Corporation and has been furnished by the respective nominees individually.
The following is a brief biography of the nominees:
Jerald J. Wenker – Director and Chairman of the Board
Mr. Wenker is currently President and Chief Operating Officer of Dermalogica, a leading professional skin care company based in the United States. Previously, he was President of Ther-Rx Corporation, the branded division of KV Pharmaceuticals. Prior to Ther Rx, Mr. Wenker worked at Abbott Laboratories for approximately 15 years where he held several executive roles in such areas as commercial and marketing management, strategic planning, licensing and new business development as well as new product development. Mr. Wenker holds a Master of Science in Marketing from Northwestern University’s J.L. Kellogg Graduate School of Management.
Roderick Carter, M.D. – Proposed Director
Mr. Carter has a strong history of contributions to healthcare through clinical, research, business and people leadership. He has significant experience developing and commercializing nutraceutical and pharmaceutical products and has successfully led clinical research and business development strategies for cardiovascular and inflammation related diseases. Mr. Carter is currently Principal at Aquila Life Sciences LLC, a consulting firm he founded focusing on pharmaceutical development and commercialization. Prior to this he was Vice President of Clinical Development at Reliant Pharmaceuticals, which developed the omega-3 cardiovascular drug Lovaza, and today is a wholly owned subsidiary of GlaxoSmithKline. He also served as Executive Director at Merck and Co., USA, President and CEO of WellGen and Senior Medical Director at Pfizer Inc., USA. Dr. Carter received his Medical Degree from the University of Witwatersrand, Johannesburg, along with a Master of Science degree in Sports Medicine from Trinity College, Dublin.
Jim Hamilton – Proposed Director
Mr. Hamilton is currently President and CEO of Neptune Technologies & Bioressources Inc., Acasti’s mother company. Prior to joining Neptune, Mr. Hamilton served as Vice President Human Nutrition and Health, North America, and President of DSM Nutritional Products USA, Inc., based in Parsippany, New Jersey. He was serving on the global management team of DSM Nutritional Products’ Human Nutrition & Health business, an organization with over $2 billion in global sales and operations in more than 40 countries. DSM Nutritional Products is an important division of the life sciences and material sciences corporation, DSM N.V. of the Netherlands. Mr. Hamilton’s industry knowledge has made him a valuable contributor to several trade associations and he is the immediate past chairman of the board of directors of the Council for Responsible Nutrition, the dietary supplement industry’s leading trade association. Mr. Hamilton is a graduate of Concordia University in Montreal, Canada and he has attended a number of business education and leadership programs at the London Business School and INSEAD.
59
Adrian Montgomery – Proposed Director
Mr. Montgomery is President of Tuckamore Capital, a publicly-traded company that has invested approximately $700 million in successful private businesses since its inception in 2005. Prior to joining Tuckamore, he headed business development at Rogers Media Inc. Mr. Montgomery is a lawyer and member of the New York State Bar and currently serves on the boards of Epsilon Energy, a TSX-listed Company, and the Toronto East General Hospital Foundation.
Dr. Reed V. Tuckson – Director
Dr. Tuckson is a graduate of Howard University, Georgetown University School of Medicine, and the Hospital of the University of Pennsylvania's General Internal Medicine Residency and Fellowship Programs, where he was also a Robert Wood Johnson Foundation Clinical Scholar studying at the Wharton School of Business. Dr. Tuckson is currently the Managing Director of Tuckson Health Connections, LLC, a health and medical care consulting business. Previously, he served a long tenure as Executive Vice President and Chief of Medical Affairs for UnitedHealth Group, a Fortune 25 health and well-being company. Dr. Tuckson is member of the Advisory Committee to the Director of the National Institutes of Health and is also an active member of the Institute of Medicine of the National Academy of Sciences. He also serves on the Boards of the American Telemedicine Association, Howard University and Cell Therapeutics Inc., a public corporation.
Dr. Harlan W. Waksal – Director
Dr. Harlan W. Waksal is a retired physician. Dr. Waksal was the Vice-President, Business and Scientific Affairs at Acasti, the Corporation’s subsidiary. He received his B.A. from Oberlin College and M.D. from Tufts University School of Medicine, and his post graduate training in Internal Medicine and in Pathology. In addition, he did research in immunology at the Weizmann Institute of Science. Dr. Waksal was a founder of Imclone Systems Incorporated; a New York based pharmaceutical company specializing in developing new treatment for various forms of cancer. He served as the Chief Operating Officer and member of the Board of Directors from 1986 until 2001 and as President/CEO from 2001 until 2002. During his tenure, he was responsible for building the scientific and operation infrastructure of the company. Dr. Waksal is the author of over 50 scientific publications and has been the author of multiple patents and patent applications. His current activities are focused on managing various real estate developments and serving on select Board of Directors. Dr. Waksal currently serves on the Boards of the Oberlin College, Senesco Technologies, Inc. He also serves on the Advisory Board of Northern Rivers Funds.
Other than information with respect to Mr. Waksal, our Vice-President, Business and Scientific Affairs, which is found in the table above regarding information about our directors, the following table sets forth each member of our senior management’s name, province and country of residence and his/her principal occupation.
|
Name, Province and Country of
Residence
|
Principal Occupation
|
Position Within the Corporation
|
||
|
Pierre Lemieux
Québec, Canada
|
Chief Operating Officer of Acasti
|
Chief Operating Officer
|
Following are brief biographies of our senior managers:
Dr. Pierre Lemieux Ph.D. – Chief Operating Officer
Dr. Pierre Lemieux has been the Chief Operating Officer of the Corporation since April 12, 2010. He holds a post-doctoral degree in Oncology from the Health Science Center, University of Texas (San Antonio), USA, and a PhD in biochemistry from Laval University, Canada, jointly with University of Nottingham, England. Prior to joining the Corporation, Dr. Lemieux was the President, Chief Executive Officer and the chairman of the board as well as being the founder of Technologie Biolactis Inc., a late-stage biotechnology company specialized in the valorization of proteins to better serve the nutraceutical, cosmetic and pharmaceutical industries.
|
B.
|
Compensation
|
60
Director Compensation
For the financial year ended on February 28, 2015, Mr. Henri Harland (the Corporation’s former President and CEO until April 28, 2014) did not receive any compensation by the Corporation in his capacity as Director and was not considered by the Board as being “independent” within the meaning of National Instrument 52-110 – Audit Committees (“NI 52-110”). Dr. Harland Waksal (former Vice-President, Business and Scientific Affairs at Acasti until October 14, 2015) was also not considered by the Board as being “independent”.
The Directors’ compensation consists of a base annual retainer in the amount of $10,000 and attendance fees for meetings of the Board of Directors and its committees in the amount of $1,000 when the meeting is held in person and half of said amount when the meeting is held by telephone. There was no additional annual retainer for the Board and committee chairs.
In addition to acting as Directors of the Corporation, Mr. Jerald J. Wenker, Mr. Valier Boivin, Dr. Ronald Denis, Mr. Pierre Fitzgibbon, Mr. Adrian Montgomery, Dr. Reed V. Tuckson and Dr. Harlan W. Waksal, also occupied the position of director of Neptune and were remunerated by Neptune in those capacities For a description of the compensation paid to the Directors of the Corporation who rendered services to Neptune or other subsidiaries of Neptune during the financial year ended February 28, 2015, we refer you to Neptune’s management information circular dated June 15, 2015 (the “Neptune Circular”) available on SEDAR at www.sedar.com.
Compensation Paid to Directors
The total compensation paid to the non-executive Directors by the Corporation and its subsidiaries during the financial year ended on February 28, 2015 is set out in the following table:
|
Name
|
Financial Year Ended February 28
|
Fees earned
($)
|
Option-based awards(1)(2)
($)
|
All other compensation (3)(4)
($)
|
Total
($)
|
|
Jerald J.Wenker
|
2015
|
14,000
|
15,316
|
3,751 (5)
|
33,067
|
|
Valier Boivin
|
2015
|
18,250
|
-
|
-
|
18,250
|
|
Ronald Denis
|
2015
|
15,250
|
-
|
-
|
15,250
|
|
Pierre Fitzgibbon
|
2015
|
13,000
|
30,633
|
-
|
43,633
|
|
Adrian Montgomery
|
2015
|
10,500
|
30,633
|
-
|
41,133
|
|
Reed V. Tuckson
|
2015
|
14,750
|
-
|
-
|
14,750
|
|
Harlan Waksal
|
2015
|
16,250
|
-
|
40,000 (6)
|
56,250
|
|
(1)
|
The Corporation has adopted the IFRS 2 Shared-based payment to account for the issuance of stock options to employees and non-employees. The fair value of the awards is estimated at the grant date using the Black-Scholes Option Pricing Model. This model requires the input of a number of parameters, including stock price, stock exercise price, expected stock price volatility, expected time until exercise and risk-free interest rates. Although the assumptions used reflect management’s best estimates, they involve inherent uncertainties based on market conditions generally outside of the Corporation’s control.
|
|
(2)
|
For the period ended on February 28, 2015, the fair market value of the June 26, 2014 option-based award granted to Mr. Wenker, Mr. Montgomery and Mr. Fitzgibbon is based on a fair value of $0,41 per option.
|
|
(3)
|
The Directors do not receive pension benefits, perquisites or other non-equity annual compensation.
|
|
(4)
|
The value of the perquisites and other personal benefits received by these Directors did not total an aggregate value of $50,000 or more, and does not represent more than 10% of the compensation paid during 2015.
|
|
(5)
|
3,500 USD converted at 1.2503 (exchange rate, as of February 27th 2015) was paid for consulting services rendered to the Corporation and its subsidiaries.
|
61
|
(6)
|
This amount represents a salary payment for his role as Vice-President, Business and Scientific Affairs at Acasti until October 14, 2014 for the sum of $40 000.
|
Outstanding Share-Based, Option-Based, and Warrant-Based Awards for Directors
The following tables provides information on the number and value of the outstanding share-based, option-based and warrant-based awards held by non-executive Directors of the Corporation at the end of the financial year ended February 28, 2015.
Share-Based Awards
|
Non-Executive Directors’ Name
|
Number of shares or units of shares that have not vested (#)
|
Market or payout value of share-based awards that have not vested ($) (1)
|
Market or payout value of vested share-based awards that have not paid-out or distributed ($)
|
|
Harlan W. Waksal
|
37,500
|
25,125
|
n/a
|
|
(1) Calculation is based on the trading price, at closing, of Acasti’s shares on the TSXV of $0.67 on February 27, 2015.
|
|||
Option-Based Awards
|
Name / Grant Date
|
Number of securities underlying unexercised options(1)
|
Option exercise price ($)
|
Option expiration date
|
Value of unexercised in-the-money options
($)(2)
|
|
Jerald Wenker
|
||||
|
June 26, 2014
|
37,500
|
1.20
|
June 26, 2017
|
-
|
|
December 19, 2013
|
37,500
|
2.10
|
December 19, 2016
|
-
|
|
Ronald Denis
|
||||
|
April 11, 2012
|
50,000
|
2.10
|
April 11, 2017
|
-
|
|
June 16, 2011
|
75,000
|
1.40
|
June 16, 2016
|
-
|
|
October 8, 2008
|
25,000
|
0.25
|
October 8, 2018
|
10,500
|
|
Pierre Fitzgibbon
|
||||
|
June 26, 2014
|
75,000
|
1.20
|
June 26, 2017
|
-
|
|
Adrian Montgomery
|
||||
|
June 26, 2014
|
75,000
|
1.20
|
June 26, 2017
|
-
|
|
Reed Tuckson
|
||||
|
December 19, 2013
|
75,000
|
2.10
|
December 19, 2016
|
-
|
|
Harlan Waksal
|
||||
|
April 11, 2012
|
200,000(3)
|
2.10
|
April 11, 2017
|
-
|
|
June 16, 2011
|
200,000(3)
|
1.40
|
June 16, 2016
|
-
|
|
(1) On June 21, 2013, Neptune granted call-option based awards to independent Directors of the Corporation at the time, namely, Dr. Denis and Mr. Boivin. They were each granted call-options for 75,000 Class A Shares of the Corporation, such call-options having a call-option exercise price of $3.00 and a call option expiration date of June 21, 2017. For additional information, please refer to the “Outstanding Share-Based, Option-Based, Call-Option-Based, and Warrant-Based Awards for Directors – Call-Option Based Awards” section in the Neptune Circular.
(2) Calculation is based on the trading price, at closing, of Acasti’s shares on the TSXV of $0.67 on February 27, 2015.
(3) Awards received for his role as former Vice-President, Business and Scientific Affairs.
|
||||
62
Share-based and Option-based Awards of the Corporation – value vested during the financial year ended on February 28, 2015
The following table sets out the value of share-based and option- awards of the Corporation held by non-executive Directors of the Corporation that vested during the financial year ended on February 28, 2015:
|
Name
|
Share-based Awards of the Corporation – value vested during the financial year ended on February 28, 2015 ($)
|
Option-based Awards of the Corporation – value vested during the financial year ended on February 28, 2015 ($)
|
|
Valier Boivin
|
5,533.35
|
-
|
|
Ronald Denis
|
11,066.65
|
-
|
|
Harlan W. Waksal
|
67,783.35
|
-
|
Compensation of Named Executive Officers
During the financial year ended February 28, 2015, the Corporation had four Named Executive Officers of the Corporation, being, Pierre Lemieux, Chief Operating Officer (“COO”), André Godin, the Corporation’s interim Chief Executive Officer (“CEO”) and Chief Financial Officer (“CFO”), Henri Harland , the Corporation’s former Chief Executive Officer until April 27, 2014 and Xavier Harland, the Corporation’s former Chief Financial Officer until June 13, 2014.
“Named Executive Officer” (or “NEO”) means: (a) a CEO, (b) a CFO, (c) each of the three most highly compensated executive officers of the Corporation, including any of its subsidiaries, or the three most highly compensated individuals acting in a similar capacity, other than the CEO and the CFO, at the end of the most recently completed financial year whose total compensation was, individually, more than $150,000, and (d) each individual who would be an NEO under paragraph (c) above but for the fact that the individual was neither an executive officer of the Corporation or its subsidiaries, nor acting in a similar capacity, at the end of that financial year.
Compensation Discussion and Analysis
Compensation of executive officers of the Corporation is recommended to the Board of Directors by the Human Resources and Governance Committee. In its review process, the Human Resources and Governance Committee relies on input from management on the assessment of executives and Corporation performance.
During the most recently completed financial year, the Human Resources and Governance Committee was composed of the following independent members: Pierre Fitzgibbon, Ronald Denis, Adrian Montgomery, Reed V. Tuckson, and Jerald J. Wenker. The Human Resources and Governance Committee establishes management compensation policies and oversees their general implementation. All members of the Human Resources and Governance Committee have direct experience which is relevant to their responsibilities as Human Resources and Governance Committee members. All members are or have held senior executive or director roles within significant businesses, several also having public companies experience, and have a good financial understanding which allows them to assess the costs versus benefits of compensation plans. The members combined experience in the Corporation’s sector provides them with the understanding of the Corporation’s success factors and risks, which is very important when determining metric for measuring success.
Risk management is a primary consideration of the Human Resources and Governance Committee when implementing its compensation program. It does not believe that its compensation program results in unnecessary or inappropriate risk taking, including risks that are likely to have a material adverse effect on the Corporation. Payments of bonuses, if any, are not made until performance goals are met.
Executive compensation is generally based on pay for performance and competitive with other firms of comparable size in similar fields. The Chief Executive Officer makes recommendations to the Human Resources and Governance Committee as to the compensation of the Corporation’s executive officers, other than himself, for approval by the Board. The Human Resources and Governance Committee makes recommendations to the Board of Directors as to the compensation of the Chief Executive Officer, for approval, in accordance with the same criteria upon which the compensation of other executive officers is based.
63
Executive compensation is comprised of a base salary and variable components in the form of an annual bonus opportunity and stock options. The annual bonus provides an opportunity for management and executive employees to earn an annual cash incentive based on the global financial results of the Corporation and the degree of achievement of objectives set by the Board of Directors, generally based on actual versus budgeted results. These performance goals will therefore take into account (1) the Corporation’s earnings, profit, adjusted EBITDA and their compliance with budgeted results, (2) the Corporation’s share performance during the last completed financial year, and (3) the business development and personal achievements fulfilled by each executive employee, as the case may be. Generally, new stock option grants do not take into account previous grants of options when considering new grants.
Qualitative factors beyond the quantitative financial metrics are also a key consideration in determination of individual executive compensation payments. How executives achieve their financial results and demonstrate leadership consistent with the Corporation’s values are key to individual compensation decisions.
The President and Chief Executive Officer’s salary is based on comparable market consideration and the Human Resources and Governance Committee’s assessment of his performance, with regard to the Corporation’s financial performance and progress in achieving strategic performance.
The Corporation’s executive compensation program is intended to attract, motivate and retain high performing senior executives, encourage and reward superior performance and align the executives’ interests with those of the Corporation by providing a compensation which is competitive with the compensation received by executives employed by comparable companies. Ensuring that the achievement of annual objectives is rewarded through the payment of bonuses and providing executives with long-term incentive through the grant of stock options.
The Human Resources and Governance Committee has authority to retain the services of independent compensation consultants to advise its members on executive compensation and related matters, and to determine the fees and the terms and conditions of the engagement of such consultants. During the year, the Human Resources and Governance Committee retained the services of Hexarem Inc. (“Hexarem”) to review the Corporation’s executive compensation programs, including base salary, short-term and long-term incentives, total cash compensation levels and total direct compensation of certain senior positions, against those of peer groups of similar and larger size, as measured by market capitalization, biotechnology and pharmaceutical companies listed or headquartered in North America. The compensation policy is currently under review and is expected to be finalized during the current financial year.
All of the services provided by Hexarem were provided to the Human Resources and Governance Committee. The Human Resources and Governance Committee has assessed the independence of Hexarem and concluded that its engagement of Hexarem does not raise any conflict of interest with the Corporation or any of the Directors or executive officers.
The Directors and executive officers are not permitted to purchase financial instruments, including for greater certainty, prepaid variable forward contracts, equity swaps, collars or units of exchange funds that are designed to hedge or offset a decrease in market value of equity securities granted as compensation or held, directly or indirectly, by the Director or officer.
Compensation Elements
Compensation of Named Executive Officers is revised each year and has been structured to encourage and reward the executive officers on the bases of short-term and long-term corporate performance. In the context of the analysis of the compensation for the financial year ended February 28, 2015, the following components were examined:
|
(i)
|
base salary;
|
|
(ii)
|
annual incentive plan, consisting of a cash bonus;
|
|
(iii)
|
grant of stock options of the Corporation;
|
|
(iv)
|
equity based compensation; and
|
|
(v)
|
other elements of compensation, consisting of benefits.
|
Base Salary
The compensation of the Corporation’s executive officers is determined by the Board of Directors upon recommendations made by the Human Resources and Governance Committee. Executive compensation is generally based on pay for performance and to be competitive with other firms of comparable size in similar fields.
Annual Incentive Plan
The Corporation has a bonus plan for the executive officers, representing a percentage of their base annual salary. The grant of bonus performance is left at the discretion of the Board of Directors upon the recommendation of the Human Resources and Governance Committee, based on the global financial results of the Corporation and the degree of achievement of objectives set by the Board of Directors, as more fully described above. Mr. Pierre Lemieux, COO of Acasti, is eligible for up to a 30% bonus of his annual base salary.
64
Stock Options and Warrants
The grant of stock options by Acasti and/or the transfer of Acasti warrants held by Neptune to the Named Executives Officers aims to recognize and reward the impact of longer-term strategic actions undertaken by management, offering an added incentive for the retention of the Named Executive Officers as well as aligning the interests of the Corporation’s executives with those of its Shareholders.
The stock option component of an NEO’s compensation, which includes a vesting element to ensure retention, serves to both motivate the executive toward increasing share value and to enable the executive to share in the future success of the Corporation.
The Corporation’s Human Resources and Governance Committee is responsible for overseeing and managing the Stock Option Plan. All grants of options to executives are approved by the Board of Directors.
The grant of options and/or warrants is part of the long-term incentive component of executive and director compensations and an essential part of compensation. Designated senior executives and Directors may participate in the stock option plan, which is designed to encourage optionees to link their interests with those of Shareholders, in order to promote an increase in Shareholder value. Awards are made by the Board of Directors, after recommendation by the Human Resources and Governance Committee. Awards are established, among other things, according to the role and responsibilities associated with the participant’s position and his or her influence over appreciation in Shareholder value. Previous awards may sometimes be taken into account when new awards are considered. The terms of the plan are described below under the heading “Stock Option Plan” below.
Equity Based Executive Compensation
The grant of restricted share units, stock options by the Corporation and/or the transfer of warrants to the Named Executive Officers aims to recognize and reward the impact of longer-term strategic actions undertaken by management, offering an added incentive for the retention of the Corporation’s executives as well as aligning the interests of the Corporation’s executives with that of its Shareholders.
On May 22, 2013, the Equity Incentive Plan was adopted by the Board of Directors in order to provide the Corporation with a share-related mechanism to attract, retain and motivate qualified Directors, employees and consultants of the Corporation and its subsidiaries. The adoption of the Corporation’s Equity Incentive Plan was approved by the Shareholders at its 2013 Shareholders’ meeting held on June 27, 2013. For more a more detailed description of the Corporation’s Equity Incentive Plan, please see below.
Stock Option Plan
The Corporation’s Stock Option Plan was adopted by the Board of Directors on October 8, 2008, amended as of April 29, 2009, and further amended as of March 21, 2011 and May 22, 2013.
The Stock Option Plan was adopted to ensure that the Corporation and its Shareholders benefit from incentive participation through the holding of Common Shares by Directors, officers, employees and consultants of the Corporation, as designated by the Board of Directors.
On May 22, 2013, the Board approved an amendment to the Stock Option Plan in order to comply with the revised regulations of the TSXV governing stock option plans. This amendment was approved by the Shareholders at its 2013 Shareholders’ meeting held on June 27, 2013.
The Stock Option Plan is administered by the Board of Directors, which will determine, inter alia, the number of Common Shares covered by any stock option and the exercise price, expiry date and vesting period of each stock option in accordance with the terms of the Stock Option Plan. The Corporation’s Human Resources and Governance Committee is responsible for overseeing and managing the Stock Option Plan. All grants of options to executives are approved by the Board of Directors.
Options for Common Shares of the Corporation representing, from time to time, up to 10% of the issued Common Shares of the Corporation then outstanding may be granted by the Board of Directors pursuant to the Stock Option Plan.
65
The number of options granted to a consultant or to a person the services of whom are retained in investor relations shall not exceed, for any 12 month period, more than 2% of the outstanding and issued shares of the Corporation. In addition, the Stock Option Plan, together with any other plan that may be established by the Corporation or any options already granted by the Corporation will not (unless the requisite Shareholder approval is obtained under applicable securities legislation) result in either (i) the number of securities (calculated on a fully diluted basis) reserved for issuance under options being granted to (A) related persons, in excess of 10% of the outstanding securities of the Corporation; or (B) a related person and the associates of the related person, in excess of 5% of the outstanding securities of the Corporation, or (ii) the number of securities, calculated on a fully diluted basis, issued within a period of 12 months to (A) related persons, in excess of 10% of the outstanding securities of the Corporation, or (B) an insider, in excess of 5% of the outstanding securities of the Corporation.
The options are non-transferable and may be exercised during the period determined by the Board of Directors, such period will begin at the earliest on the date of the grant of such options and will end at the latest ten years after such grant. The options will lapse upon termination of employment or the end of the business relationship with the Corporation or death of the holder, except that the options may be exercised for 60 days following either termination of employment or the end of the business relationship or the end of a director’s term (30 days for an employee who works in investor relations). In the case of the death of a holder, their options may be exercised within one year of their death. Any option granted to a holder who becomes bankrupt shall be presumed to have expired prior to the date that the holder is declared bankrupt.
Subject to the approval of the relevant authorities, including the TSXV if applicable, and compliance with any conditions attached to such approval (including, in certain circumstances, approval by disinterested Shareholders) if applicable, the Board of Directors has the right to amend or terminate the Stock Option Plan. However, unless option holders consent to the amendment or termination of the Stock Option Plan in writing, any such amendment or termination of the Stock Option Plan cannot affect the conditions of options that have already been granted and that have not been exercised under the Stock Option Plan.
Pursuant to the rules of the TSXV, the Stock Option Plan must be approved each year by the Shareholders of the Corporation at its annual meeting.
Equity Incentive Plan
The following is a summary of important provisions of the equity incentive plan of Acasti (the “Equity Incentive Plan”). It is not a comprehensive discussion of all of the terms and conditions of the Equity Incentive Plan. Readers are advised to review the full text of the Equity Incentive Plan to fully understand all terms and conditions of the Equity Incentive Plan. A copy of the Equity Incentive Plan can be obtained by contacting Acasti’s Corporate Secretary.
On May 22, 2013, the Equity Incentive Plan was adopted by the Board in order to, amongst other things, provide Acasti with a share-related mechanism to attract, retain and motivate qualified Directors, employees and consultants of Acasti. The adoption of the Equity Incentive Plan was approved by the Shareholders at its 2013 Shareholders’ meeting held on June 27, 2013.
Eligible Persons may participate in the Equity Incentive Plan. “Eligible Persons” under the Equity Incentive Plan consist of any director, officer, employee or consultant (as defined in the Equity Incentive Plan) of Acasti or of a subsidiary. A participant (“Participant”) is an Eligible Person to whom an award has been granted under the Equity Incentive Plan. The Equity Incentive Plan provides Acasti with the option to grant to Eligible Participants Bonus Shares, Restricted Shares, Restricted Share Units, Performance Share Units, Deferred Share Units and other Share-Based Awards.
Subject to the adjustment provisions provided for in the Equity Incentive Plan and the applicable rules and regulations of all regulatory authorities to which Acasti is subject (including any stock exchange), the total number of Common Shares reserved for issuance pursuant to awards granted under the Equity Incentive Plan will be equal to a number that (A) if, and for so long as the Common Shares are listed on the TSXV, shall not exceed either (i) 1,829,282 Common Shares, and (ii) 10% of the issued and outstanding Common Shares, which number shall include Common Shares issuable pursuant to the Acasti Stock Option Plan, or (B) if, and for so long as the Common Shares are listed on the TSX, shall not exceed 2.5% of the issued and outstanding Common Shares from time to time.
If, and for so long as the Common Shares are listed on the TSXV, no more than 5% of the issued and outstanding Common Shares may be granted to any one individual Participant in any 12 month period (unless Acasti has obtained disinterested approval for such grant) and no more than 2% of the issued and outstanding Common Shares may be granted to any one consultant or employee conducting investor relations activities in any 12 month period.
66
If, and for so long as the Common Shares are listed on the TSX, the number of Common Shares (A) issuable, at any time, to Participants that are insiders, and (B) issued to Participants that are insiders within any 12 month period, pursuant to the Equity Incentive Plan, or when combined with all of Acasti’s other security based share compensation arrangements shall not, in aggregate, exceed 10% of the total number of outstanding Common Shares on a non-diluted basis.
The Board shall have the right to determine that any unvested or unearned Restricted Share Units, Deferred Share Units, Performance Share Units or other Share-Based Awards or Restricted Shares subject to a Restricted Period outstanding immediately prior to the occurrence of a change in control shall become fully vested or earned or free of restriction upon the occurrence of such change in control. The Board may also determine that any vested or earned Restricted Share Units, Deferred Share Units, Performance Share Units or other Share-Based Awards shall be cashed out at the market price as of the date such change in control is deemed to have occurred, or as of such other date as the Board may determine prior to the change in control. Further, the Board shall have the right to provide for the conversion or exchange of any Restricted Share Unit, Deferred Share Unit, Performance Share Unit or other Share-Based Award into or for rights or other securities in any entity participating in or resulting from the change in control.
The Equity Incentive Plan is administered by the Board and the Board has sole and complete authority, in its discretion, to determine the type of awards under the Equity Incentive Plan relating to the issuance of common shares (including any combination of Bonus Shares, Restricted Share Units, Performance Share Units, Deferred Share Units, Restricted Shares or other Share-Based Awards) in such amounts, to such persons and under such terms and conditions as the Board may determine, in accordance with the provisions of the Equity Incentive Plan.
Other Forms of Compensation
The Corporation’s executive employee benefit program includes life, medical, dental and disability insurance. These benefits and perquisites are designed to be competitive overall with equivalent positions in comparable organizations. The Corporation does not have any pension plan available for its employees, executives or Directors.
Summary Compensation Table – Named Executive Officers
The following Summary Compensation Table sets forth the compensation information for the Named Executive Officers for services rendered during the financial year ended February 28, 2015 and allocated to the Corporation. For a description of the compensation of the Named Executives Officers that includes compensation for their roles with Neptune and its subsidiaries, refer to the information relating thereto in the management information circular of Neptune dated June 15, 2015 which can be found on SEDAR at www.sedar.com.
|
Name and
Principal Position
|
Year ended February 28/29
|
Salary
($)
|
Share-Based Awards(1)(2)
($)
|
Option-based/Warrant-based awards(1)(2)
($)
|
Annual incentive plans
($)
|
All other compensation
($)(3)(4)(8)
|
Total compensation
($)
|
|
Pierre Lemieux
Chief Operating Officer
|
2015
2014
2013
|
184,115
170,308
190,769
|
-
207,000
-
|
22,163
102,505
167,956
|
-
-
-
|
16,000
-
-
|
222,278
479,813
358,725
|
|
André Godin(6)
Former Interim President, CEO and CFO
|
2015
2014
2013
|
63,538
23,442
25,277
|
-
54,790
-
|
14,775
12,255
120,986
|
20,000
-
-
|
19,419
-
-
|
117,732
90,487
146,263
|
|
Henri Harland(7)
Former CEO and President
|
2015
2014
2013
|
25,742
128,712
106,402
|
-
492,180
-
|
-
119,487
368,659
|
-
-
-
|
72,811
-
-
|
98,553
740,379
475,061
|
|
Xavier Harland(8)
Former Chief Financial Officer
|
2015
2014
2013
|
38,077
115,693
118,038
|
-
345,000
-
|
-
85,421
191,073
|
-
-
-
|
31,651
-
-
|
69,728
546,114
309,111
|
|
(1)
|
The Corporation has adopted the IFRS 2 Shared-based payment to account for the issuance of stock options to employees and non-employees. The fair value of stock options is estimated at the grant date using the Black-Scholes Option Pricing Model. This model requires the input of a number of parameters, including stock price, stock exercise price, expected stock price volatility, expected time until exercise and risk-free interest rates. Although the assumptions used reflect management’s best estimates, they involve inherent uncertainties based on market conditions generally outside of the Corporation’s control.
|
67
|
(2)
|
For the period ended on February 28, 2015, the fair market value of the October 20, 2014 option-based award granted to Mr. André Godin and Mr. Pierre Lemieux is based on a fair value of $0.30 per option.
|
For the period ended on February 28, 2014, the fair market value of the June 27, 2013 Acasti share-based awards is based on a fair value of $2.89 per restricted share unit (“RSU”) granted to all NEOs.
For the period ended on February 28, 2014, the fair market value of the June 21, 2013 Acasti call-option based awards granted by Neptune is based on a fair value of $1.14 per Acasti call-option granted to Mr. Pierre Lemieux and Mr. Xavier Harland, and $1.22 per Acasti call-option granted to Mr. Henri Harland and Mr. André Godin.
For the period ending on February 28, 2013, the fair market value of the April 11, 2012 option-based awards is based on a fair value of $1.12 per option granted to Mr. Pierre Lemieux, $0.96 per option granted to Mr. Xavier Harland, $1.21 per option granted to Mr. André Godin and $1.23 per option granted to Mr. Henri Harland.
|
(3)
|
The NEOs do not receive pension benefits, perquisites or other non-equity annual compensation.
|
|
(4)
|
The value of perquisites and other personal benefits received by these executives did not total an aggregate value of $50,000 or more, and does not represent 10% or more of their total salary in FY2015, 2014 or 2013.
|
|
(5)
|
These amounts include severance payments, vacation time accumulated and paid during FY2015, as well as salary cuts applied during FY2013-2014 that were paid back to the Name Executive Officers during FY2015.
|
|
(6)
|
Mr. André Godin became Interim President and Chief Executive Officer of the Corporation on May 23, 2014 and Chief Financial Officer of the Corporation on June 16, 2014. Mr. Godin’s functions with the Corporation were terminated on April 29, 2015.
|
|
(7)
|
Mr. Henri Harland resigned as President, Secretary and Chief Executive Officer of the Corporation on April 27, 2014.
|
|
(8)
|
Mr. Xavier Harland resigned as Chief Financial Officer of the Corporation on June 13, 2014.
|
Outstanding Share-Based, Option-Based and Warrant-Based Awards
The following tables provide information on the number and value of the outstanding share-based, option-based and warrant-based awards held by Named Executive Officer at the end of the financial year ended February 28, 2015.
Share-Based Awards
|
Named Executive Officers
|
Number of shares or units of shares that have not vested (#)
|
Market or payout value of share-based awards that have not vested ($) (1)
|
Market or payout value of vested share-based awards that have not paid-out or distributed ($)
|
|
Pierre Lemieux
Chief Operating Officer
|
12,500
|
8,375
|
-
|
|
André Godin(2)
Interim Chief Executive Officer and Interim Chief Financial Officer
|
12,500
|
8,375
|
-
|
|
Xavier Harland(3)
Former Chief Financial Officer
|
25,000
|
16,750
|
-
|
|
(1) Calculation is based on the trading price, at closing, of Acasti’s shares on the TSXV of $0.67 on February 27, 2014.
(2) Mr. André Godin became Interim President and Chief Executive Officer of the Corporation on May 23, 2014 and Chief Financial Officer of the Corporation on June 16, 2014. Mr. Godin’s functions with the Corporation were terminated on April 29, 2015.
(3) Mr. Xavier Harland resigned as Chief Financial Officer of the Corporation on June 13, 2014.
|
|||
68
Option-Based Awards
|
Name / Grant Date
|
Number of securities underlying unexercised options (#)
|
Option exercise price ($)
|
Option expiration date
|
Value of unexercised in-the-money options(1)
($)
|
|
Pierre Lemieux
|
||||
|
October 20, 2014
|
75,000
|
0.65
|
October 19, 2019
|
1,500
|
|
April 11, 2012
|
150,000
|
2.10
|
April 11, 2017
|
-
|
|
June 16, 2011
|
200,000
|
1.40
|
June 16, 2016
|
-
|
|
André Godin(2)
|
||||
|
October 20, 2014
|
50,000
|
0.65
|
October 19, 2019
|
1,000
|
|
April 11, 2012
|
100,000
|
2.10
|
April 11, 2017
|
-
|
|
June 16, 2011
|
150,000
|
1.40
|
June 16, 2016
|
-
|
|
October 8, 2008
|
100,000
|
0.25
|
October 8, 2018
|
42,000
|
|
Xavier Harland(3)
|
||||
|
April 11, 2012
|
200,000
|
2.10
|
April 11, 2017
|
-
|
|
June 16, 2011
|
200,000
|
1.40
|
June 16, 2016
|
-
|
|
October 8, 2008
|
50,000
|
0.25
|
October 8, 2018
|
21,000
|
|
(1) Calculation is based on the trading price, at closing, of Acasti’s shares on the TSXV of $0.67 on February 27, 2014.
(2) Mr. André Godin became Interim President and Chief Executive Officer of the Corporation on May 23, 2014 and Chief Financial Officer of the Corporation on June 16, 2014. Mr. Godin’s functions with the Corporation were terminated on April 29, 2015.
(3) Mr. Xavier Harland resigned as Chief Financial Officer of the Corporation on June 13, 2014.
|
||||
Share-based, Option-based, and Warrant-based Awards of the Corporation – value vested during the financial year ended on February 28, 2015
The following table sets out the value of share-based awards and the value of option-based and warrant-based awards of the Corporation held by the NEOs of the Corporation that vested during the financial year ended on February 28, 2015:
|
Name
|
Share-based Awards of the Corporation – value vested during the financial year ended on February 28, 2014 ($)
|
Option-based and Warrant-based Awards of the Corporation – value vested during the financial year ended on February 28, 2014 ($)
|
|
Pierre Lemieux
|
20,750
|
-
|
|
André Godin(1)
|
20,750
|
-
|
|
Henri Harland(2)
|
3,633
|
-
|
|
Xavier Harland(3)
|
41,500
|
-
|
69
|
(1) Mr. André Godin became Interim President and Chief Executive Officer of the Corporation on May 23, 2014 and Chief Financial Officer of the Corporation on June 16, 2014. Mr. Godin’s functions with the Corporation were terminated on April 29, 2015.
(2) Mr. Henri Harland resigned as President, Secretary and Chief Executive Officer of the Corporation on April 27, 2014.
(3) Mr. Xavier Harland resigned as Chief Financial Officer of the Corporation on June 13, 2014.
|
Performance Graph
On February 27, 2015, the closing price of the Common Shares of the Corporation on the TSXV was $0.67 per share. The following graph shows the cumulative return in dollars of a $100 investment in common shares of the Corporation, as of March 31st, 2011 on the TSXV, compared with the total return of the S&P TSX Composite Index for the period shown on this graph.
Note: The Corporation’s shares were listed on the TSXV for the first time on March 31, 2011 (CA: APO).
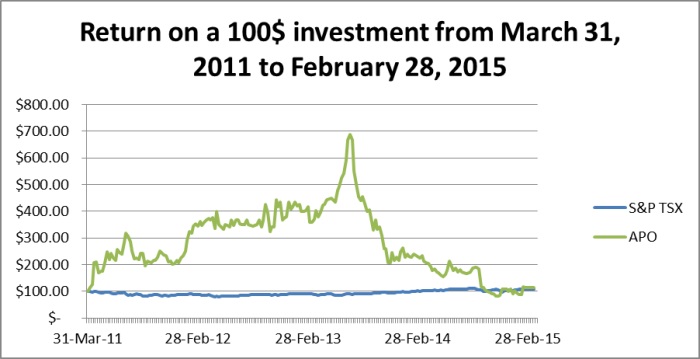
The Human Resources and Governance Committee considers a number of factors and performance elements when determining compensation for the members of the executive management. Although total cumulative Shareholder return is one performance measure that is reviewed, it is not the only consideration in executive compensation deliberations. As a result, a direct correlation between total cumulative Shareholder return over a given period and executive compensation levels is not anticipated.
Securities Authorized for Issuance Under Equity Compensation Plans
The following table sets out, as at February 28, 2015 the share-based compensation plans of the Corporation pursuant to which shares can be issued from treasury. The number of shares which appears at in the line “Share-based compensation plan” refers to the Corporation’s Stock Option Plan and Equity Incentive Plan.
70
|
Plan Category
|
(A) Number of securities to be issued upon the exercise of outstanding options and rights
|
(B)
Weighted average exercise price of outstanding options and rights
($)
|
(C)
Numbers of Shares available for further issuance under the stock based compensation plans (excluding shares from (A))
(Common Shares)
|
|
|
Equity compensation plans approved by security holders
|
Stock Option Plan(1)
|
4,296,500
|
1.53
|
6,347,901
|
|
Equity Incentive Plan(2)
|
184,000
|
n/a
|
769,282
|
|
|
Equity compensation plans not approved by security holders
|
n/a
|
n/a
|
n/a
|
|
|
Total
|
4,480,500
|
7,117,183 (3)
|
||
|
(1) Please refer to Section “Stock Option Plan” elsewhere in this Annual Report for a description of the principal terms of the Stock Option Plan.
(2) Please refer to Section “Equity Incentive Plan” elsewhere in this Annual Report for a description of the principal terms of the Equity Incentive Plan.
(3) Subject to the adjustment provisions provided for in the Equity Incentive Plan and the applicable rules and regulations of all regulatory authorities to which Acasti is subject (including any stock exchange), the total number of Common Shares reserved for issuance pursuant to awards granted under the Equity Incentive Plan will be equal to a number that (A) if, and for so long as the Common Shares are listed on the TSXV, shall not exceed either (i) 1,829,282 Common Shares, and (ii) 10% of the issued and outstanding Common Shares, which number shall include Common Shares issuable pursuant to the Acasti Stock Option Plan, or (B) if, and for so long as the Common Shares are listed on the TSX, shall not exceed 2.5% of the issued and outstanding Common Shares from time to time.
|
||||
The Stock Option Plan of the Corporation is a rolling stock option plan within the meaning of the Policy 4.4 of the TSX Venture Exchange Corporate Finance Manual which permits the issuance of up to 10% of the issued and outstanding Common Shares of the Corporation from time to time. The number of Shares reserved for issuance and which will be available for issuance pursuant to awards granted under the Equity Incentive Plan is equal to a number that, if, and for so long as the Shares are listed on the TSXV, shall not exceed either (i) 1,829,282 Common Shares, and (ii) 10% of the issued and outstanding Shares, which number shall include Shares issuable pursuant to the Stock Option Plan.
Pension Benefit Plans
The Corporation has no pension benefit plans.
Termination and Change of Control Benefits
Pierre Lemieux, Chief Operating Officer of Acasti
In accordance with the terms and provisions of the employment agreement entered into between the Corporation and Mr. Pierre Lemieux, the Corporation may terminate the executive’s employment at any time without cause by providing him with a six-week notice of termination and payment of base salary payable in six equal monthly installments, representing one month plus one month per year of service up to the lower of (i) $125,000, or (ii) twelve (12) months.
The employee may also, within sixty (60) days of the occurrence of a “fundamental change” as defined in the employment agreement (which includes a reduction of salary or of the responsibilities or functions of the employee), voluntarily terminate his employment by giving the Corporation thirty (30) days written notice of termination. In this case, the employee will be entitled to the same compensation and conditions as for a termination of the employment agreement by the Corporation for any reason other than just cause, as described above.
71
|
C.
|
Board Practices
|
Board of Directors
Director Independence
The Board of Directors believes that, in order to maximize effectiveness, the Board of Directors must be able to operate independently A majority of Directors must satisfy the applicable tests of independence, such that the Board of Directors complies with all independence requirements under applicable corporate and securities laws and stock exchange requirements applicable to the Corporation. No Director will be independent unless the Board of Directors has affirmatively determined that the Director has no material relationship with the Corporation or any of its affiliates, either directly or indirectly or as a partner, shareholder or officer of an organization that has a relationship with the Corporation or its Affiliates. Such determinations will be made on an annual basis and, if a Director joins the Board of Directors between annual meetings, at such time.
Independent Directors.
The Board of Directors considers that Mr. Wenker, Dr. Denis, Mr. Boivin, Mr. Fitzgibbon, Mr. Montgomery and Dr. Tuckson are “independent” within the meaning of NI 52-110 and NASDAQ listing rules, as it applies to the Board of Directors.
Directors who are not independent.
The Board of Directors considers that Dr. Harlan Waksal is not “independent” within the meaning of NI 52-110, as it applies to the Board of Directors in that Dr. Harlan Waksal was executive officer and employee of Acasti. Mr. Waksal resigned as an executive officer of Acasti on October 14, 2014.
Majority of Directors will be independent.
As of the date of this Annual Report, the Board of Directors considers that currently six of its seven members of the Board of Directors are independent within the meaning of NI 52-110 and NASDAQ listing rules, as it applies to the Board of Directors. Upon the election of the proposed Directors, four of the six members of the Board for the ensuing year will be independent within the meaning of NI 52-110 and NASDAQ listing rules, as it applies to the Board of Directors, and a majority of the Directors will therefore be independent.
Upon the election of the proposed Directors, only Mr. Jim Hamilton will serve on the Board of Directors of Neptune.
Independent Directors hold regularly scheduled closed meetings.
During the last completed financial year ended February 28, 2015, the independent Directors held at least three (3) scheduled meetings at which non-independent Directors and members of management were not in attendance.
Attendance record of Directors for Board meetings
During the financial year ended February 28, 2015, the Board of Directors held 8 meetings. Attendance of Directors at the meetings is indicated in the table below:
|
Board Members
|
Meeting Attendance in Person
|
Telephone Meeting Attendance
|
Total Attendance
|
|
Jerald Wenker
|
5/7
|
2/7
|
7/7
|
|
Ronald Denis
|
5/8
|
1/8
|
6/8
|
|
Valier Boivin
|
7/8
|
1/8
|
8/8
|
|
Pierre Fitzgibbon
|
5/5
|
1/5
|
5/5
|
|
Harlan Waksal
|
6/8
|
1/8
|
7/8
|
|
Reed Tuckson
|
2/8
|
6/8
|
8/8
|
|
Adrian Montgomery
|
3/5
|
-
|
3/5
|
72
Chairman of the Board
Mr. Jerald Wenker, an independent director, acts as Chairman of the Board. His duties and responsibilities consist in the oversight of the quality and integrity of the Board of Directors’ practices.
Board Mandate
How the Board delineates its role and responsibilities
There is no specific mandate for the Board of Directors, since the Board has plenary power. Any responsibility that is not delegated to senior management or a committee of the Board remains with the full Board of Directors.
Position Descriptions
How the Board delineates the role and responsibilities of the chair and the chair of each Board committee
No written position description has been developed for the chair of the Board of Directors and for the chairs of each committee. The primary role and responsibility of the chair of each committee of the Board of Directors is to: (i) in general, ensure that the committee fulfills its mandate, as determined by the Board of Directors; (ii) chair meetings of the committee; (iii) report thereon to the Board to the Board of Directors; and (iv) act as liaison between the committee and the Board of Directors and, if necessary, management of the Corporation.
How the Board delineates the role and responsibilities of the CEO
The Board of Directors has not developed a written position description for the Chief Executive Officer. The Chief Executive Officer’s objectives are discussed and decided during a Board of Directors meeting following the Chief Executive Officer’s presentation of the Corporation’s annual plan. These objectives include a general mandate to maximize Shareholder value. The Board of Directors approves the Chief Executive Officer’s objectives for the Corporation on an annual basis
Orientation and Continuing Education
Measures the Board takes to orient new Directors
The Corporation provides orientation for new appointees to the Board of Directors and committees in the form of informal meetings with members of the Board and senior management, complemented by presentations on the main areas of the Corporation’s business.
Measures the Board takes to ensure that its Directors maintain the skill and knowledge necessary to meet their obligations as Directors
The Board does not formally provide continuing education to its Directors. The Directors are experienced members. The Board of Directors relies on professional assistance when judged necessary in order to be educated/updated on a particular topic.
Audit Committee Information
The Audit Committee is responsible for assisting the Board of Directors in fulfilling its oversight responsibilities with respect to financial reporting, including (i) reviewing the Corporation’s procedures for internal control with the Corporation’s auditor and management performing financial functions; (ii) reviewing and approving the engagement of the auditor; (iii) reviewing annual and quarterly financial statements and all other material continuous disclosure documents, including the Corporation’s annual information form and management’s discussion and analysis; (iv) assessing the Corporation’s financial and accounting personnel; (v) assessing the Corporation’s accounting policies; (vi) reviewing the Corporation’s risk management procedures; and (vii) reviewing any significant transactions outside the Corporation’s ordinary course of business and any pending litigation involving the Corporation.
The Audit Committee has direct communication channels with Acasti’s management performing financial functions and the external auditor of Acasti to discuss and review such issues as the Audit Committee may deem appropriate.
The Audit Committee is comprised of Mr. Valier Boivin, who acts as Chair and Messrs. Pierre Fitzgibbon and Jerald J. Wenker. Each of these individuals is “financially literate” and “independent” within the meaning of NI 52-110. For more information on the expertise and experience of each member, please refer to the “Report on the Audit Committee” section of the Corporation’s annual information form.
73
Compensation Committee
The Compensation Committee has the responsibility of evaluating the compensation, performance incentives as well as the benefits granted to the Corporation’s upper management in accordance with their responsibilities and performance as well as to recommend the necessary adjustments to the Board. This committee also reviews the amount and method of compensation granted to the directors. The Compensation Committee may mandate an external firm in order to assist it during the execution of its mandate. The Compensation Committee considers time commitment, comparative fees and responsibilities in determining compensation.
The Compensation Committee is only composed of independent members within the meaning of NI 52-110, namely Dr. Ronald Denis, Mr. Valier Boivin and Mr. Jean-Claude Debard. Mr. Debard is not a nominee for election as a director for the ensuing year.
Other Board Committees
Other than the Audit Committee, the Corporation also has a Human Resources and Governance Committee. The mandate of the Human Resources and Governance Committee consists of the evaluation of the proposed nominations of senior executives and Director candidates to the Corporation’s Board of Directors, recommending for Board approval, if appropriate, revisions to our corporate governance practices and procedures, developing new charters for any new committees established by the Board of Directors, monitoring relationships and communication between management and the Board of Directors, monitoring emerging best practices in corporate governance and oversight of governance matters and assessing the Board of Directors, its committees and Directors. The Human Resources and Governance Committee is also in charge of establishing the procedure which must be followed by the Corporation in order for it to comply with the guidelines of the TSXV regarding corporate governance.
Assessments
The Board of Directors, its committees and each Director of the Corporation are subject to regular evaluations of their efficacy and contribution. The evaluation procedure consists in identifying any shortcomings and implementing adjustments proposed by Directors at the beginning and during meetings of the Board of Directors and of each of its committees. Among other things, these adjustments deal with the level of preparation of Directors, management and consultants employed by the Corporation, the relevance and sufficiency of the documentation provided to Directors and the time allowed to Directors for discussion and debate of items on the agenda.
Director Term Limits
The Board has actively considered the issue of term limits for Directors and will continue to do so. At this time, the Board does not believe that it is in the best interests of the Corporation to establish a limit on the number of times a Director may stand for election. While such a limit could help create an environment where fresh ideas and viewpoints are available to the Board, a director term limit could also disadvantage the Corporation through the loss of the beneficial contribution of Directors who have developed increasing knowledge of, and insight into, the Corporation and its operations, over a period of time. As the Corporation operates in a unique industry, it is difficult to find qualified Directors with the appropriate background and experience and the introduction of a director term limit would impose further difficulty.
Policies Regarding the Representation of Women on the Board and Amongst Executive Officers
The Corporation has not adopted a formal written policy regarding diversity amongst executive officers and members of the Board of Directors, including mechanisms for Board renewal, in connection with, among other things, the identification and nomination of women Directors. Nevertheless, the Corporation recognizes that gender diversity is a significant aspect of diversity and acknowledges the important role that women with appropriate and relevant skills and experience can play in contributing to the diversity of perspective on the Board of Directors.
Rather than considering the level of representation of women for directorship and executive officer positions when making Board or executive officer appointments, Acasti considers all candidates based on their merit and qualifications relevant to the specific role. While Acasti recognizes the benefits of diversity at all levels within its organization, it does not currently have any targets, rules or formal policies that specifically require the identification, consideration, nomination or appointment of candidates for directorship or executive management positions or that would otherwise force the composition of the Corporation’s Board of Directors and executive management team. Currently, Neptune does not have any women who are executive officers or Directors.
|
D.
|
Employees
|
Acasti’s management consists of professionals experienced in business development, finance and science. The Acasti research team includes scientists with expertise in pharmaceutical development, chemistry, manufacturing and controls, nonclinical and clinical studies, pharmacology, regulatory affairs, quality assurance/quality control, intellectual property and strategic alliances. As of February 28, 2015, the Corporation employed seven people in Canada, six of whom have biology, chemistry, biochemistry or microbiology credentials, and one administrative staff with a pharmaceutical industry background. Acasti generally requires all of its employees to enter into an invention assignment, non-disclosure and non-compete agreement. The Corporation relies, in part, on the administrative and other staff of its parent company, Neptune, and also relies on consultants from time to time. The Corporation’s employees are not covered by any collective bargaining agreement or represented by a trade union. The Corporation places special emphasis on training for its personnel.
74
|
E.
|
Share Ownership
|
The following table shows the total number of Common Shares beneficially owned by each of our directors and senior management and the percentage of the total issued and outstanding Common Shares that such holdings represent.
|
Name
|
Common Shares beneficially owned
as of May 27, 2015
|
Percentage of total issued and
outstanding Common Shares
as of May 27, 2015(1)
|
||||||
|
Jerald J. Wenker
|
2500 | * | ||||||
|
Reed V. Tuckson
|
7,299 | * | ||||||
|
Pierre Lemieux
|
45,000 | * | ||||||
|
Harlan Waksal
|
873,700 | * | ||||||
|
Adrian Montgomery
|
- | * | ||||||
|
Jim Hamilton
|
- | * | ||||||
|
Roderick Carter
|
- | * | ||||||
|
|
(1)
|
Based on 106,444,012 Common Shares outstanding.
|
|
|
*
|
Less than 1%.
|
See “Item 6.B – Compensation” above for information regarding the share-based, option-based, call-option-based, and warrant-based awards held by our directors and senior managers.
See “Item 6.B – Compensation” above for a description of our Stock Option Plan and Equity Incentive Plan.
|
Item 7.
|
Major Shareholders and Related Party Transactions
|
|
A.
|
Major Shareholders
|
As of May 27, 2015, Neptune owns 50,755,933 Common Shares representing approximately 47.68% of the Common Shares issued and outstanding. The Common Shares are voting, participating and have no par value. Neptune also owns a warrant entitling it to acquire 592,500 Common Shares. Neptune does not have different voting rights than other beneficial owners of Common Shares.
To the best of our knowledge, there are no other beneficial owners of 5% or more of any class of our voting securities.
On February 10, 2012, Neptune acquired 750,000 Common Shares through a private placement. As a result, Neptune’s equity participation in Acasti increased from approximately 56% to approximately 57%.
On July 12, 2013, Neptune announced that it had acquired 6,750,000 Common Shares upon the exercise of a warrant issued to it by Acasti under the prepayment agreement. The prepayment agreement and the issuance of the 6,750,000 Common Shares to Neptune were approved by the TSX-V and the disinterested shareholders of Acasti (excluding Neptune and non-arm’s length parties to Neptune) at the annual meeting of shareholders of Acasti held on June 27, 2013. As a result, Neptune’s equity participation in Acasti increased from approximately 57% to approximately 60%.
On December 3, 2013, Neptune acquired 592,500 units (each unit consists of one Common Share and one common share purchase warrant) in our underwritten public unit offering. As a result, Neptune’s equity participation in Acasti decreased from approximately 60% to approximately 49.95%.
All Common Shares of the Corporation, including all those held by Neptune, are common shares with similar voting rights. Based on the records of the Corporation’s registrar and transfer agent as of June 15, 2015, Computershare Trust Company of Canada, there were approximately 116 registered holders (including DTC) of the Corporation’s Common Shares resident in the United States (approximately 10% of all registered holders).
75
|
B.
|
Related Party Transactions
|
Please see the section entitled “Related Party Transactions” in our MD&A included above.
|
C.
|
Interests of Experts and Counsel
|
Not applicable.
|
Item 8.
|
Financial Statements
|
|
A.
|
Consolidated Statements and Other Financial Information
|
Financial Statements
See “Item 17 – Financial Statements” for our audited consolidated financial statements.
Legal Proceedings
Due to the fact that a significant portion of the Corporation’s intellectual property rights are licensed to it by Neptune, the Corporation relies on Neptune to protect a significant portion of the intellectual property rights that it uses under such license. Neptune is engaged in a number of legal actions related to its intellectual property.
Henri Harland
On May 29, 2014, Henri Harland, former President and Chief Executive Officer of the Corporation filed a lawsuit against the Corporation, Neptune and NeuroBioPharm Inc. (“NeuroBioPharm”) in connection with his departure as President and Chief Executive Officer of each of Neptune, Acasti and NeuroBioPharm. Among other things, Mr. Harland alleged that his resignation occurred as a result of a constructive dismissal and is seeking approximately $8.5 million in damages, interest and costs. In addition, Mr. Harland is seeking from Neptune, Acasti and NeuroBioPharm, as applicable, the issuance of 500,000 shares of each of Neptune, Acasti and NeuroBioPharm as well as two blocks of 1,000,000 call options on shares held by Neptune in Acasti and NeuroBioPharm. As a result of the lawsuit, Mr. Harland was requested to resign as Director of the Corporation. On December 11, 2014, Neptune, Acasti and NeuroBioPharm filed their defense and counterclaim alleging inter alia that Mr. Harland’s contract is null and void and that he is owed nothing following his resignation. Should the Court determine that the contract is nonetheless valid, the Defendants’ position, as stated in the defense and counterclaim, is that there was also enough evidence discovered after Mr. Harland’s resignation that would have justified a dismissal for cause and that again, nothing is owed to the plaintiff. No trial date has been set. No agreement has been reached and an estimate of its financial effect cannot be made. Neptune and the Corporation have also filed an additional claim to recover certain amounts from Mr. Harland.
Dividend Policy
We do not anticipate paying any cash dividend on the Common Shares in the foreseeable future. We presently intend to retain future earnings to finance the expansion and growth of our business. Any future determination to pay dividends will be at the discretion of the Corporation’s Board of Directors and will depend on our financial condition, results of operations, capital requirements and other factors the Board of Directors deems relevant. In addition, the terms of any future debt or credit facility may preclude us from paying dividends.
|
Item 9.
|
The Offer and Listing
|
|
A.
|
Listing Details
|
Since March 31, 2011, the Common Shares have been listed on the TSX-V under the ticker symbol APO. Since January 7, 2013, the Common Shares have been listed on the NASDAQ Stock Market under the ticker symbol ACST. The following tables set forth, for the periods indicated, the high and low market prices of our common shares as reported on the TSX-V and the NASDAQ Stock Market.
|
|
(a)
|
For the five most recent full fiscal years:
|
76
|
TSX-V
|
NASDAQ Stock Market
|
|||||||||||||||
|
Fiscal year ended
|
High $
|
Low $
|
High US$
|
Low US$
|
||||||||||||
|
Feb. 28, 2011
|
— | — | — | — | ||||||||||||
|
Feb. 29, 2012
|
2.15 | 0.51 | — | — | ||||||||||||
|
Feb. 28, 2013
|
2.76 | 1.60 | 3.99 | 2.00 | ||||||||||||
|
Feb. 28, 2014
|
4.32 | 1.15 | 4.20 | 1.09 | ||||||||||||
|
Feb. 28, 2015
|
1.49 | 0.40 | 1.34 | 0.35 | ||||||||||||
|
|
(b)
|
For each full financial quarter of the two most recent full fiscal years and any subsequent period:
|
|
TSX-V
|
NASDAQ Stock Market
|
|||||||||||||||
|
Period
|
High $
|
Low $
|
High US$
|
Low US$
|
||||||||||||
|
1st Quarter ended May 31, 2013
|
2.74 | 2.00 | 3.15 | 1.97 | ||||||||||||
|
2nd Quarter ended Aug. 31, 2013
|
4.32 | 2.45 | 4.20 | 2.39 | ||||||||||||
|
3rd Quarter ended Nov. 30, 2013
|
3.05 | 1.15 | 2.90 | 1.09 | ||||||||||||
|
4th Quarter ended Feb. 28, 2014
|
1.70 | 1.20 | 1.56 | 1.15 | ||||||||||||
|
1st Quarter ended May 31, 2014
|
1.49 | 0.88 | 1.34 | 0.80 | ||||||||||||
|
2nd Quarter ended Aug. 31, 2014
|
1.30 | 0.88 | 1.22 | 0.81 | ||||||||||||
|
3rd Quarter ended Nov. 30, 2014
|
1.20 | 0.40 | 1.11 | 0.35 | ||||||||||||
|
4th Quarter ended Feb. 28, 2015
|
0.78 | 0.46 | 0.62 | 0.40 | ||||||||||||
|
|
(c)
|
for the most recent six months:
|
|
TSX-V
|
NASDAQ Stock Market
|
|||||||||||||||
|
Period
|
High $
|
Low $
|
High US$
|
Low US$
|
||||||||||||
|
December 2014
|
0.72 | 0.46 | 0.61 | 0.40 | ||||||||||||
|
January 2015
|
0.76 | 0.52 | 0.62 | 0.44 | ||||||||||||
|
February 2015
|
0.78 | 0.50 | 0.62 | 0.41 | ||||||||||||
|
March 2015
|
0.76 | 0.56 | 0.61 | 0.45 | ||||||||||||
|
April 2015
|
0.64 | 0.48 | 0.52 | 0.39 | ||||||||||||
|
May 2015
|
0.55 | 0.40 | 0.46 | 0.32 | ||||||||||||
|
June 2015 (up to June 15)
|
0.78 | 0.36 | 0.62 | 0.29 | ||||||||||||
The holders of Common Shares are entitled to vote at all meetings of our shareholders except meetings at which only holders of a specified class or series of shares are entitled to vote. The holders of Common Shares are entitled to receive dividends as and when declared by the Board, if any.
No Common Shares have been issued subject to call or assessment. There are no pre-emptive or conversion rights and no provisions for redemption or purchase for cancellation, surrender, or sinking or purchase funds. The Common Shares must be issued as fully-paid and non-assessable, and are not subject to further capital calls by us. All of the Common Shares rank equally as to voting rights, participation in a distribution of the assets of the Corporation on a liquidation, dissolution or winding-up of the Corporation and the entitlement to dividends.
Common shares are transferable at the offices of our transfer agent and registrar in Toronto, Ontario, Canada and Montreal, Québec, Canada.
There are no restrictions in our constating documents on the free transferability of the Common Shares.
77
|
B.
|
Plan of Distribution
|
Not applicable.
|
C.
|
Markets
|
Since March 31, 2011, the Common Shares have been listed on the TSX-V under the ticker symbol APO. Since January 7, 2013, the Common Shares have been listed on the NASDAQ Stock Market under the ticker symbol ACST.
|
D.
|
Selling Shareholders
|
Not applicable.
|
E.
|
Dilution
|
Not applicable.
|
F.
|
Expenses of the Issuer
|
Not applicable.
|
Item 10.
|
Additional Information
|
|
A.
|
Share Capital
|
Not applicable.
|
B.
|
Memorandum and Articles of Association
|
We were incorporated on February 1, 2002 under Part 1A of the Companies Act (Québec) under the name “9113-0310 Québec Inc”. On August 7, 2008, pursuant to a Certificate of Amendment, we changed our name to “Acasti Pharma Inc.”, our share capital, the provisions regarding the restrictions on securities transfers and the borrowing powers of the Corporation. On November 7, 2008, pursuant to a Certificate of Amendment, we further revised our provisions regarding our borrowing powers. We became a reporting issuer in the Province of Québec on November 17, 2008. On February 14, 2011, the Business Corporations Act (Québec) came into effect and replaced the Companies Act (Québec). We are now governed by the Business Corporations Act (Québec) (the “BCA”).
|
1.
|
Register, Entry Number and Purposes
|
Our articles of incorporation, as amended, or Articles, and general by-laws, or By-laws, do not define any of the Corporation’s objects and purposes. In that respect, the Corporation has no limit on the type of business it can carry out.
|
2.
|
Directors’ Powers
|
Our Articles and By-laws do not contain any provision regarding: (a) a director’s power to vote on a proposal, arrangement or contract in which the director is materially interested; (b) a director’s power in the absence of an independent quorum, to vote compensation to itself or any members of the committees of the Board; (c) borrowing powers exercisable by the directors and how such powers can be varied; (d) retirement or non-retirement of directors under an age limit requirement; and (e) number of shares, if any, required for a director’s qualification. However, the BCA provides that a director shall avoid placing himself in a situation where his personal interest would conflict with his obligations as a director of the Corporation. If such is the case, the BCA provides that he must declare to the Corporation any interest he has in an enterprise or other entity that may place him in a situation of conflict of interest.
The quorum at every meeting of the Board has been set to the minimum number of directors required under our Articles. In the absence of a quorum, a director has no power to make any decision regarding, among other things, compensation to himself or to any member of the committees of the Board.
Our By-laws do not contain any requirements with respect to a mandatory retirement age for our directors and the number of shares required for directors’ qualifications.
78
|
3.
|
Rights, Preferences and Restrictions Attaching to Each Class of Shares
|
The Corporation’s authorized capital consists of an unlimited number of no par value Common Shares and an unlimited number of no par value Class B, Class C, Class D and Class E preferred shares (collectively the “Preferred Shares”), issuable in one or more series.
As of February 28, 2015, there were (i) a total of 105,862,179 Common Shares issued and outstanding and no Preferred Shares issued and outstanding, (ii) 4,911,000 options to purchase Common Shares issued and outstanding, at a weighted average exercise price of $1.57 per Common Share, and (iii) 20,766,542 warrants (including 592,500 warrants held by Neptune) to purchase Common Shares issued and outstanding, at a weighted average exercise price of $1.65 per Common Share.
The following is a brief description of the rights, privileges, conditions and restrictions attaching to the Common Shares and Preferred Shares.
Common Shares
Voting Rights
Each Common Share entitles its holder to receive notice of, and to attend and vote at, all annual or special meetings of the shareholders of the Corporation. Each Common Share entitles its holder to one vote at any meeting of the shareholders, other than meetings at which only the holders of a particular class or series of shares are entitled to vote due to statutory provisions or the specific attributes of this class or series.
Dividends
Subject to the prior rights of the holders of Preferred Shares ranking before the Common Shares as to dividends, the holders of Common Shares are entitled to receive dividends as declared by the Board of the Corporation from the Corporation’s funds that are available for the payment of dividends.
Winding-up and Dissolution
In the event of the Corporation’s voluntary or involuntary winding-up or dissolution, or any other distribution of the Corporation’s assets among its shareholders for the purposes of winding up its affairs, the holders of Common Shares shall be entitled to receive, after payment by the Corporation to the holders of Preferred Shares ranking prior to Common Shares regarding the distribution of the Corporation’s assets in the case of winding-up or dissolution, share for share, the remainder of the property of the Corporation, with neither preference nor distinction. The order of priority, applicable to all classes of shares of the Corporation with respect to the redemption, liquidation, dissolution or distribution of property (the “Order of priority”) is as follows: First, the Class E non-voting shares; Second, the Class D non-voting shares; Third, the Class B multiple voting shares and Class C non-voting shares, pari passu; and Fourth, the Common Shares.
Notwithstanding the above-mentioned Order of priority, shareholders of a class of shares may renounce the above-mentioned Order of priority by unanimous approval by all shareholders of that class of shares.
Preferred Shares
Class B multiple voting shares
Each Class B multiple voting share entitles the holder thereof to ten (10) votes per share in all shareholder meetings of the Corporation.
Dividends
Holders of Class B multiple voting shares are entitled to receive, as and when such dividends are declared, an annual non-cumulative dividend of five percent (5%) on the amount paid for the said shares, payable at the time and in the manner which the Directors may determine and subject to the Order of priority.
Participation
Subject to the provisions of subsection 5.2.2 of the Articles, holders of Class B multiple voting shares do not have the right to participate in the profits or surplus assets of the Corporation.
79
Conversion
Holders of Class B multiple voting shares have the right, at their entire discretion, to convert, part or all of the Class B multiple voting shares they hold into Common Shares on the basis of one (1) Common Share for each Class B multiple voting share converted.
Redemption
Subject to the provisions of the BCA and the Order of priority, holders of Class B multiple voting shares have the right to demand from the Corporation, upon a thirty (30) day written notice, that the Corporation redeem the Class B multiple voting shares at a price equivalent to the amount paid for such shares plus the redemption premium, as defined in subsection 5.2.4.1 of the Articles, and any and all declared but yet unpaid dividends on same.
Liquidation
In the event of the dissolution or liquidation of the Corporation or any other distribution of its property, the Class B voting shareholders shall have the right to be reimbursed for the amount paid on Class B multiple voting shares plus the redemption premium, as defined in subsection 5.2.4.1 of the Articles as well as the amount of any and all declared but yet unpaid dividends on said shares, subject to the Order of priority.
Class C Non-Voting Shares
Subject to the provisions of the BCA, holders of Class C non-voting shares are neither be entitled to vote at any meeting of the shareholders of the Corporation, nor to receive a notice of such meeting nor to attend any such meeting.
Dividends
Holders of Class C non-voting shares are entitled to receive, as and when such dividends are declared, an annual non-cumulative dividend of five percent (5%) on the amount paid for the said shares, plus a redemption premium as defined in subsection 5.3.6.1 of the Articles, payable at the time and in the manner which the Directors may determine and subject to the Order of priority.
Participation
Subject to the provisions of subsection 5.3.2 of the Articles, holders of Class C non-voting shares do not have the right to participate in the profits or surplus assets of the Corporation.
Conversion
Holders of Class C non-voting shares have the right, at their entire discretion, to convert, part or all of the Class C non-voting shares they hold into Common Shares on the basis of one (1) Common Share for each Class C non-voting share converted.
Forced Conversion
All of the Corporation’s Class C non-voting shares shall automatically be converted in Common Shares upon the request of an unrelated third party investor in the Corporation, investing more than $500,000, or any other amount to be determined by the Board of directors of the Corporation, in the Corporation and requesting as a condition to the investment that the Class C non-voting shares be converted into Common Shares on the basis of one Common Share for each Class C non-voting share converted.
Redemption
Subject to the provisions of the BCA and the Order of priority, holders of Class C non-voting shares have the right to demand from the Corporation, upon a thirty (30) day written notice, that the Corporation redeem the Class C non-voting shares at $0.20 per share, and any and all declared but yet unpaid dividends on same.
Liquidation
In the event of the dissolution or liquidation of the Corporation or any other distribution of its property, the shareholders have the right to be reimbursed for the amount paid on Class C non-voting shares plus the redemption premium, as defined in subsection 5.3.6.1 of the Articles, as well as the amount of any and all declared but yet unpaid dividends on said shares, subject to the Order of priority.
80
Class D Non-Voting Shares
Subject to the provisions of the BCA, holders of Class D non-voting shares shall neither be entitled to vote at any meeting of the shareholders of the Corporation, nor to receive a notice of such meeting nor to attend any such meeting.
Dividends
Holders of Class D non-voting shares are entitled to receive, as and when such dividends are declared, a monthly non-cumulative dividend of half of one percent to two percent (0.5% to 2%) on the amount paid for such shares, plus a redemption premium as defined in subsection 5.4.6.1 of the Articles, payable at the time and in the manner which the Directors may determine and subject to the Order of priority.
Participation
Subject to the provisions of subsection 5.4.2 of the Articles, holders of Class D non-voting shares shall not have the right to participate in the profits or surplus assets of the Corporation.
Conversion
Holders of Class D non-voting shares shall have the right, at their entire discretion, to convert, part or all of the Class D non-voting shares they hold into Common Shares on the basis of a number of Common Shares equal to the number of Class D non-voting shares converted multiplied by the conversion ratio, calculated as follows:
|
Conversion Ratio =
|
The product obtained by multiplying a factor to be agreed at the time of the issuance of the Class D non-voting shares by the average amount paid per share for the Class D non-voting shares plus the redemption premium per share, as defined in subsection 5.4.6.1 of the Articles as well as the amount of any and all declared but yet paid dividends per said shares
|
|
Fair Market Value of the Common Shares at the date of any conversion of Class D non-voting shares in Common Shares
|
Forced Conversion
All of the Corporation’s Class C non-voting shares shall automatically be converted in Common Shares upon the request of an unrelated third party investor in the Corporation, investing more than $500,000, or any other amount to be determined by the Board of directors of the Corporation, in the Corporation and requesting as a condition to the investment that the Class C non-voting shares be converted into Common Shares in all cases, on the basis of a number of Common Shares equal to the number of Class D non-voting shares converted multiplied by the conversion ratio, calculated as follows :
|
Conversion Ratio =
|
The product obtained by multiplying a factor to be agreed at the time of the issuance of the Class D non-voting shares by the average amount paid per share for the Class D non-voting shares plus the redemption premium per share, as defined in subsection 5.4.6.1 of the Articles as well as the amount of any and all declared but yet paid dividends per said shares
|
|
Fair Market Value of the Common Shares at the date of any conversion of Class D non-voting shares in Common Shares
|
Redemption
Subject to the provisions of the BCA and the Order of priority, holders of Class D non-voting shares have the right to demand from the Corporation, upon a thirty (30) day written notice, that the latter redeem the Class D non-voting shares that are held by the shareholder(s) at a price equivalent to the amount paid for said shares plus the redemption premium, as defined in subsection 5.4.6.1 of the Articles, and any and all declared but yet unpaid dividends on same.
81
Liquidation
In the event of the dissolution or liquidation of the Corporation or any other distribution of its property, the shareholders shall have the right to be reimbursed for the amount paid on Class D non-voting shares plus the redemption premium, as defined in subsection 5.4.6.1 of the Articles as well as the amount of any and all declared but yet unpaid dividends on said shares, subject to the Order of priority.
Class E Non-Voting Shares
Subject to the provisions of the BCA, holders of Class E non-voting shares shall neither be entitled to vote at any meeting of the shareholders of the Corporation, nor to receive a notice of such meeting nor to attend any such meeting.
Dividends
Holders of Class E non-voting shares are entitled to receive, as and when such dividends are declared, a monthly non-cumulative dividend of half of one percent to two percent (0.5% to 2%) on the amount paid for the said shares, payable at the time and in the manner which the Directors may determine and subject to the Order of priority.
Participation
Subject to the provisions of subsection 5.5.2 of the Articles, holders of Class E non-voting shares shall not have the right to participate in the profits or surplus assets of the Corporation.
Conversion
Holders of Class E non-voting shares shall have the right, at their entire discretion, to convert, part or all of the Class E non-voting shares they hold into Common Shares on the basis of a number of Common Shares equal to the number of Class E non-voting shares converted multiplied by the conversion ratio, calculated as follows:
|
Conversion Ratio =
|
The product obtained by multiplying a factor to be agreed at the time of the issuance of the Class E non-voting shares by the average amount paid per share for the Class E non-voting shares plus the amount of any and all declared but yet paid dividends per said shares
|
|
Fair Market Value of the Common Shares at the date of any conversion of Class E non-voting shares in Common Shares
|
Redemption
Subject to the provisions of the BCA and the Order of priority, the Corporation has the right to demand from holders of Class E non-voting shares, upon a thirty (30) day written notice, that the latter redeem the Class E non-voting shares that are held by the shareholder(s) at a price equivalent to the amount paid for said shares and any and all declared but yet unpaid dividends on same.
Liquidation
In the event of the dissolution or liquidation of the Corporation or any other distribution of its property, the shareholders shall have the right to be reimbursed for the amount paid on Class E non-voting shares as well as the amount of any and all declared but yet unpaid dividends on said shares, subject to the Order of priority.
|
4.
|
Procedures to Change the Rights of Shareholders
|
In order to change the rights attached to all classes of our shares, the vote of at least 66 2/3% of the holders of each class, as the case may be, must be cast at a shareholders meeting called for amending the rights attached to our Common Shares or Preferred Shares, as the case may be.
|
5.
|
Ordinary and Extraordinary Shareholders’ Meetings
|
Our By-laws provide that the annual meeting of shareholders of the Corporation must be held on a yearly basis on such date and on such time as may be fixed by the Board.
82
Our By-laws provide that special meetings of shareholders may be called at any time as determined by the Board. Our shareholders are entitled to call special meetings of shareholders provided that they hold at least 10% of the issued and outstanding shares entitled to vote at the meeting so called.
Our By-laws provide that notice of each annual and special meeting of shareholders must be sent to the shareholders entitled to attend such meetings at least ten (10) days prior to the date fixed for such meeting.
Our By-laws provide that during any meeting of the shareholders, the attendance, in person or by proxy, of the shareholders representing ten percent (10%) of the Common Shares shall constitute a quorum.
|
6.
|
Limitations on Rights to Own Securities
|
There exists no limitation on the right to own our securities.
|
7.
|
Impediments to Change of Control
|
Neither our Articles nor By-laws contain any provision that would have an effect of delaying, deferring or preventing a change in control of the Corporation.
|
8.
|
Stockholder Ownership Disclosure Threshold in Bylaws
|
Our Articles and By-laws do not contain any provision requiring a shareholder to disclose his ownership above a particular threshold.
|
9.
|
Significant Differences with Applicable U.S. Law
|
Canadian securities regulations, it is necessary for a shareholder to disclose his ownership above the threshold of 10%. This requirement is less stringent than in the United States where ownership must be reported when a shareholder owns at least 5% of the outstanding voting securities of an issuer. Accordingly, in Canada, it is easier for a shareholder to accumulate a substantial portion of the voting securities of an issuer without reporting it. In widely-held corporations such as ours, we believe that we are at a disadvantage compared to similar US issuers.
|
10.
|
Special Conditions for Changes in Capital
|
The conditions imposed by the Corporation’s Articles of Incorporation are not more stringent than required under the Business Corporations Act (Québec).
A copy of the Corporation’s Articles of Incorporation and By-Laws have been incorporated by reference as exhibits to this Registration Statement.
|
C.
|
Material Contracts
|
The contracts outlined below are considered to be material to us. For the two years preceding the publication of this annual report, we have not entered into any material contracts, other than contracts entered into in the ordinary course of our business, except for the contracts summarized below. Those contracts that were entered into in the ordinary course of business and which do not satisfy the requirements for disclosure have not been included below.
Prepayment Agreement
On December 4, 2012, we entered into a prepayment agreement with Neptune (the “Prepayment Agreement”). The Prepayment Agreement followed a technology license agreement that we entered into with Neptune on August 7, 2008, which was amended on February 20, 2009 and January 28, 2011, pursuant to which Neptune granted to us a license to use licensed intellectual property in consideration for the payment of royalties by the Corporation. Pursuant the Prepayment Agreement the Corporation exercised its option to pay in advance all of the future royalties through the issuance of Common Shares issuable upon the exercise of a warrant, to Neptune. The Corporation issued to Neptune a warrant entitling Neptune to acquire 6,750,000 Common Shares at a price of $2.30 per Common Share in satisfaction of the payment of royalties.
83
Warrant Indenture
On December 3, 2013 we entered into a warrant indenture with Computershare Trust Company of Canada, providing for the issue of the Corporation’s warrants (the “Warrant Indenture”). Pursuant the Warrant Indenture the Corporation appointed Computershare Trust Company of Canada as warrant agent to hold the rights, interests and benefits contained in the Warrant Indenture for and on behalf of those persons who become the holders of the warrants issued pursuant to the Warrant Indenture.
Copies of the agreements noted above are available, free of charge and are available electronically on the website of the SEC at www.sec.gov and on our SEDAR profile at www.sedar.com. Requests for such documents should be directed to our Corporate Secretary.
|
D.
|
Exchange Controls
|
Subject to the following paragraph, there is no law or governmental decree or regulation in Canada that restricts the export or import of capital, or affects the remittance of dividends, interest or other payments to non-resident holders of our subordinate voting shares, other than withholding tax requirements.
There is no limitation imposed by Canadian law or by our Articles or our other charter documents on the right of a non-resident to hold or vote voting shares, other than as provided by the Investment Canada Act (Canada), or Investment Canada Act, the North American Free trade Agreement Implementation Act (Canada), or North American Free Trade Agreement, and the World Trade Organization Agreement Implementation Act. The Investment Canada Act requires notification and, in certain cases, advance review and approval by the Government of Canada of an investment to establish a new Canadian business by a non-Canadian or of the acquisition by a “non-Canadian” of “control” of a “Canadian business”, all as defined in the Investment Canada Act. Generally, the threshold for review will be higher in monetary terms for a member of the World Trade Organization or North American Free Trade Agreement.
|
E.
|
Taxation
|
The following is a summary of certain U.S. federal income tax considerations to a U.S. Holder (as defined below) arising from and relating to the acquisition, ownership, and disposition of our Common Shares as capital assets.
This summary provides only general information and does not purport to be a complete analysis or listing of all potential U.S. federal income tax consequences that may apply to a U.S. Holder as a result of the acquisition, ownership, and disposition of our Common Shares. In addition, this summary does not take into account the individual facts and circumstances of any particular U.S. Holder that may affect the U.S. federal income tax consequences applicable to such U.S. Holder. Accordingly, this summary is not intended to be, and should not be construed as, legal or U.S. federal income tax advice with respect to any U.S. Holder. Each U.S. Holder should consult its own tax advisor regarding the U.S. federal, U.S. state and local, and non-U.S. tax consequences arising from or relating to the acquisition, ownership, and disposition of our Common Shares.
No legal opinion from U.S. legal counsel or ruling from the Internal Revenue Service (“IRS”) has been requested, or will be obtained, regarding the U.S. federal income tax consequences to U.S. Holders of the acquisition, ownership, and disposition of our Common Shares. This summary is not binding on the IRS, and the IRS is not precluded from taking a position that is different from, and contrary to, the positions taken in this summary. In addition, because the authorities on which this summary is based are subject to various interpretations, the IRS and the U.S. courts could disagree with one or more of the positions taken in this summary.
Scope of this Disclosure
Authorities
This summary is based on the Code, U.S. Treasury Regulations promulgated thereunder (whether final, temporary or proposed), published IRS rulings, judicial decisions, published administrative positions of the IRS, and the Convention between Canada and the United States of America with Respect to Taxes on Income and on Capital, signed September 26, 1980, as amended (the “Canada-U.S. Tax Treaty”). Any of the authorities on which this summary is based could be changed in a material and adverse manner at any time, and any such change could be applied on a retroactive basis. Unless otherwise discussed herein, this summary does not discuss the potential effects, whether adverse or beneficial, of any proposed legislation.
U.S. Holders
For purposes of this summary, a “U.S. Holder” is a beneficial owner of Common Shares that, for U.S. federal income tax purposes, is (a) an individual who is a citizen or resident of the U.S., (b) a corporation, or other entity classified as a corporation for U.S. federal income tax purposes, that is created or organized in or under the laws of the U.S., any state in the U.S. or the District of Columbia, (c) an estate if the income of such estate is subject to U.S. federal income tax regardless of the source of such income, or (d) a trust if (i) such trust has validly elected to be treated as a U.S. person for U.S. federal income tax purposes or (ii) a U.S. court is able to exercise primary supervision over the administration of such trust and one or more U.S. persons have the authority to control all substantial decisions of such trust.
84
U.S. Holders Subject to Special U.S. Federal Income Tax Rules Not Addressed
This summary does not address the U.S. federal income tax consequences applicable to U.S. Holders that are subject to special provisions under the Code, including, but not limited to, the following U.S. Holders: (a) U.S. Holders that are tax-exempt organizations, qualified retirement plans, individual retirement accounts, or other taxdeferred accounts; (b) U.S. Holders that are financial institutions, insurance companies, real estate investment trusts, or regulated investment companies; (c) U.S. Holders that are dealers in securities or currencies or U.S. Holders that are traders in securities that elect to apply a mark-to-market accounting method; (d) U.S. Holders that have a “functional currency” other than the U.S. dollar; (e) U.S. Holders subject to the alternative minimum tax provisions of the Code; (f) U.S. Holders that own the Common Shares as part of a straddle, hedging transaction, conversion transaction, integrated transaction, constructive sale, or other arrangement involving more than one position; (g) U.S. Holders that acquired the Common Shares through the exercise of employee stock options or otherwise as compensation for services; (h) U.S. Holders that hold the Common Shares other than as a capital asset within the meaning of Section 1221 of the Code; (i) U.S. Holders that beneficially own (directly, indirectly or by attribution) 10% or more of our voting securities or otherwise held 10% or more of the total combined voting power of the Corporation; and (j) U.S. expatriates. U.S. Holders that are subject to special provisions under the Code, including U.S. Holders described above, should consult their own tax advisor regarding the U.S. federal, U.S. federal alternative minimum, U.S. federal estate and gift, U.S. state and local, and non-U.S. tax consequences arising from and relating to the acquisition, ownership, and disposition of the Common Shares.
If an entity or arrangement that is classified as a partnership for U.S. federal income tax purposes holds Common Shares, the U.S. federal income tax consequences to such partnership and the partners of such partnership generally will depend on the activities of the partnership and the status of such partners. Partners of entities that are classified as partnerships for U.S. federal income tax purposes should consult their own tax advisors regarding the U.S. federal income tax consequences arising from and relating to the acquisition, ownership and disposition of the Common Shares.
Tax Consequences Other than U.S. Federal Income Tax Consequences Not Addressed
This summary does not address the U.S. estate and gift, alternative minimum, state, local or non-U.S. tax consequences to U.S. Holders of the acquisition, ownership, and disposition of the Common Shares. Each U.S. Holder should consult its own tax advisor regarding the U.S. estate and gift, alternative minimum, state, local and foreign tax consequences arising from and relating to the acquisition, ownership, and disposition of the Common Shares.
U.S. Federal Income Tax Considerations of the Acquisition, Ownership, and Disposition of Common Shares
Distributions on Common Shares
Subject to the possible application of the passive foreign investment company (“PFIC”) rules described below (see more detailed discussion below at “Passive Foreign Investment Company Rules”), a U.S. Holder that receives a distribution, including a constructive distribution or a taxable stock distribution, with respect to the Common Shares generally will be required to include the amount of such distribution in gross income as a dividend (without reduction for any Canadian income tax withheld from such distribution) to the extent of the current or accumulated “earnings and profits” of the Corporation (as computed for U.S. federal income tax purposes). To the extent that a distribution exceeds the current and accumulated “earnings and profits” of the Corporation, such excess amount will be treated (a) first, as a tax-free return of capital to the extent of a U.S. Holder’s adjusted tax basis in the Common Shares with respect to which the distribution is made (resulting in a corresponding reduction in the tax basis of such Common Shares) and, (b) thereafter, as gain from the sale or exchange of such Common Shares (see more detailed discussion at “Disposition of Common Shares” below). The Corporation does not intend to calculate its current or accumulated earnings and profits for U.S. federal income tax purposes and, therefore, will not be able to provide U.S. Holders with such information. U.S. Holders should therefore assume that any distribution by the Corporation with respect to the Common Shares will constitute a dividend. However, U.S. Holders should consult their own tax advisors regarding whether distributions from the Corporation should be treated as dividends for U.S. federal income tax purposes. Dividends paid on the Common Shares generally will not be eligible for the “dividends received deduction” allowed to corporations under the Code with respect to dividends received from U.S. corporations.
A dividend paid by the Corporation generally will be taxed at the preferential tax rates applicable to long-term capital gains if, among other requirements, (a) the Corporation is a “qualified foreign corporation” (as defined below), (b) the U.S. Holder receiving such dividend is an individual, estate, or trust, and (c) such dividend is paid on Common Shares that have been held by such U.S. Holder for at least 61 days during the 121-day period beginning 60 days before the “ex-dividend date” (i.e., the first date that a purchaser of such Common Shares will not be entitled to receive such dividend).
85
For purposes of the rules described in the preceding paragraph, the Corporation generally will be a “qualified foreign corporation” (a “QFC”) if (a) the Corporation is eligible for the benefits of the Canada-U.S. Tax Treaty, or (b) the Common Shares are readily tradable on an established securities market in the U.S., within the meaning provided in the Code. However, even if the Corporation satisfies one or more of such requirements, it will not be treated as a QFC if it is classified as a PFIC (as discussed below) for the taxable year during which the Corporation pays the applicable dividend or for the preceding taxable year. The dividend rules are complex, and each U.S. Holder should consult its own tax advisor regarding the application of such rules to them in their particular circumstances. Even if the Corporation satisfies one or more of such requirements, as noted below, there can be no assurance that the Corporation will not become a PFIC in the future. Thus, there can be no assurance that the Corporation will qualify as a QFC.
Disposition of Common Shares
Subject to the possible application of the PFIC rules described below (see more detailed discussion below at “Passive Foreign Investment Company Rules”), a U.S. Holder will recognize gain or loss on the sale or other taxable disposition of Common Shares (that is treated as a sale or exchange for U.S. federal income tax purposes) equal to the difference, if any, between (a) the U.S. dollar value of the amount realized on the date of such sale or disposition and (b) such U.S. Holder’s adjusted tax basis (determined in U.S. dollars) in the Common Shares sold or otherwise disposed of. Any such gain or loss generally will be capital gain or loss, which will be long-term capital gain or loss if such Common Shares are held for more than one year. Each U.S. Holder should consult its own tax advisor as to the tax treatment of dispositions of Common Shares in exchange for Canadian dollars.
Preferential tax rates apply to long-term capital gains of a U.S. Holder that is an individual, estate, or trust. There are currently no preferential tax rates for long-term capital gains of a U.S. Holder that is a corporation. Deductions for capital losses are subject to complex limitations.
Passive Foreign Investment Company Rules
Special, generally unfavorable, rules apply to the ownership and disposition of the stock of a PFIC. For U.S. federal income tax purposes, a non-U.S. corporation is classified as a PFIC for each taxable year in which either:
|
|
•
|
at least 75% of its gross income is “passive” income (referred to as the “income test”); or
|
|
|
•
|
at least 50% of the average value of its assets is attributable to assets that produce passive income or are held for the production of passive income (referred to as the “asset test”).
|
Passive income includes the following types of income:
|
|
•
|
dividends, royalties, rents, annuities, interest, and income equivalent to interest; and
|
|
|
•
|
net gains from the sale or exchange of property that gives rise to dividends, interest, royalties, rents, or annuities and certain gains from the commodities transactions.
|
In determining whether it is a PFIC, the Corporation will be required to take into account a pro rata portion of the income and assets of each corporation in which it owns, directly or indirectly, at least 25% by value.
The Corporation has not made a determination as to whether it was a PFIC for the taxable year ended February 28, 2015 or whether it will be a PFIC for the current taxable year ending February 28, 2016. Accordingly, there can be no assurance that the Corporation was not a PFIC for the taxable year ended February 28, 2015. Whether the Corporation is a PFIC depends on complex U.S. federal income tax rules that are subject to differing interpretations and whose application to the Corporation is uncertain. Further, since the PFIC status of the Corporation will depend upon the composition of its income and assets and the fair market value of its assets from time to time (including whether the Corporation owns, directly or indirectly, at least 25% by value, of the stock of any subsidiary) and generally cannot be determined until the end of a taxable year, there can be no assurance that the Corporation will not be a PFIC for the current taxable year. In addition, the Corporation cannot predict whether the composition of its income and assets (including income and assets held indirectly) or the fair market value of its assets from time to time may result in it being treated as a PFIC in any future taxable year. Accordingly, no assurance can be given that the Corporation is not a PFIC or will not become a PFIC in subsequent taxable years.
86
Generally, if the Corporation is or has been treated as a PFIC for any taxable year during a U.S. Holder’s holding period of Common Shares, any “excess distribution” with respect to the Common Shares would be allocated rateably over the U.S. Holder’s holding period. The amounts allocated to the taxable year of the excess distribution and to any year before the Corporation became a PFIC would be taxed as ordinary income. The amount allocated to each other taxable year would be subject to tax at the highest rate in effect for individuals or corporations in such taxable year, as appropriate, and an interest charge would be imposed on the amount allocated to that taxable year. Distributions made in respect of Common Shares during a taxable year will be excess distributions to the extent they exceed 125% of the average of the annual distributions on Common Shares received by the U.S. Holder during the preceding three taxable years or the U.S. Holder’s holding period, whichever is shorter.
Generally, if the Corporation is treated as a PFIC for any taxable year during which a U.S. Holder owns Common Shares, any gain on the disposition of the Common Shares would be treated as an excess distribution and would be allocated rateably over the U.S. Holder’s holding period and subject to taxation in the same manner as described in the preceding paragraph.
Certain elections may be available (including a “mark-to-market” or “qualified electing fund” election) to U.S. Holders in limited circumstances that may mitigate the adverse consequences resulting from PFIC status, particularly if they are made in the first taxable year during such holder’s holding period in which the Corporation is treated as a PFIC. U.S. Holders should be aware that, for each tax year, if any, that the Corporation is a PFIC, the Corporation can provide no assurances that it will make available to U.S. Holders the information such U.S. Holders require to make a “qualified electing fund” election with respect to the Corporation.
If the Corporation were to be treated as a PFIC in any taxable year, a U.S. Holder may be required to file an annual report with the IRS containing such information as the U.S. Treasury Department may require.
87
Each U.S. Holder should consult its own tax advisor regarding the status of the Corporation as a PFIC, the possible effect of the PFIC rules to such holder and information reporting required if the Corporation were a PFIC, as well as the availability of any election that may be available to such holder to mitigate adverse U.S. federal income tax consequences of holding shares in a PFIC.
Receipt of Foreign Currency
The amount of a distribution paid in Canadian dollars or Canadian dollar proceeds received on the sale or other taxable disposition of Common Shares will generally be equal to the U.S. dollar value of such currency on the date of receipt. If any Canadian dollars received with respect to the Common Shares are later converted into U.S. dollars, U.S. Holders may realize gain or loss on the conversion. Any gain or loss generally will be treated as ordinary income or loss and generally will be from sources within the U.S. for U.S. foreign tax credit purposes. Each U.S. Holder should consult its own tax advisor concerning the possibility of foreign currency gain or loss if any such currency is not converted into U.S. dollars on the date of receipt.
Foreign Tax Credit
Subject to certain limitations, a U.S. Holder who pays (whether directly or through withholding) Canadian or other foreign income tax with respect to the Common Shares may be entitled, at the election of such U.S. Holder, to receive either a deduction or a credit for such Canadian or other foreign income tax paid. Dividends paid on Common Shares generally will constitute income from sources outside the United States. The foreign tax credit rules (including the limitations with respect thereto) are complex, and each U.S. Holder should consult its own tax advisor regarding the foreign tax credit rules, having regard to such holder’s particular circumstances.
Information Reporting; Backup Withholding
Generally, information reporting and backup withholding will apply to distributions on, and the payment of proceeds from the sale or other taxable disposition of, the Common Shares unless (i) the U.S. Holder is a corporation or other exempt entity, or (ii) in the case of backup withholding, the U.S. Holder provides a correct taxpayer identification number and certifies that such U.S. Holder is not subject to backup withholding.
Backup withholding is not an additional tax. Any amount withheld generally will be creditable against a U.S. Holder’s U.S. federal income tax liability or refundable to the extent that it exceeds such liability provided the required information is provided to the IRS in a timely manner.
In addition, certain categories of U.S. Holders must file information returns with respect to their investment in a non-U.S. corporation. For example, certain U.S. Holders must file IRS Form 8938 with respect to certain “specified foreign financial assets” (such as the Common Shares) with an aggregate value in excess of US$50,000 (and, in some circumstances, a higher threshold). Failure to do so could result in substantial penalties and in the extension of the statute of limitations with respect to such holder’s U.S. federal income tax returns. Each U.S. Holder should consult its own tax advisor regarding application of the information reporting and backup withholding rules to it in connection with an investment in the Common Shares.
Medicare Contribution Tax
U.S. Holders that are individuals, estates or certain trusts generally will be subject to a 3.8% Medicare contribution tax on, among other things, dividends on, and capital gains from the sale or other taxable disposition of, the Common Shares, subject to certain limitations and exceptions. Each U.S. Holder should consult its own tax advisor regarding possible application of this additional tax to income earned in connection with an investment in the Common Shares.
|
F.
|
Dividends and Paying Agents
|
Not applicable.
|
G.
|
Statement by Experts
|
Not applicable.
88
|
H.
|
Documents on Display
|
Any statement in this Annual Report about any of our contracts or other documents is not necessarily complete. If the contract or document is filed as an exhibit to this Annual Report, the contract or document is deemed to modify the description contained in this Annual Report. You must review the exhibits themselves for a complete description of the contract or document.
Our SEC filings are available at the SEC’s website at www.sec.gov. You may also read and copy any document we file with the SEC at the public reference facilities maintained by the SEC at SEC Headquarters, Public Reference Section, 100 F Street, N.E., Washington D.C. 20549. You may obtain information on the operation of the SEC’s public reference facilities by calling the SEC at 1-800-SEC-0330.
In addition, we are required by Canadian securities laws to file documents electronically with Canadian securities regulatory authorities and these filings are available on our SEDAR profile at www.sedar.com. Requests for such documents should be directed to our Corporate Secretary.
|
I.
|
Subsidiary Information
|
Not applicable.
|
Item 11.
|
Quantitative and Qualitative Disclosure about Market Risk
|
Information relating to quantitative and qualitative disclosures about market risks is detailed in our MD&A in “Item 5 - Operating and Financial Review and Prospects” above, as well as in Note 17 to our audited consolidated financial statements contained in “Item 17 – Financial Statements” below.
|
Item 12.
|
Description of Securities other than Equity Securities
|
|
A.
|
Debt Securities
|
Not applicable.
|
B.
|
Warrants and Rights
|
Not applicable.
|
C.
|
Other Securities
|
Not applicable.
|
D.
|
American Depositary Shares
|
Not applicable.
89
PART II
|
Item 13.
|
Defaults, Dividend Arrearages and Delinquencies
|
None.
|
Item 14.
|
Material Modification to the Rights of Security Holdings and Use of Proceeds
|
None.
|
Item 15.
|
Controls and Procedures
|
Disclosure Controls and Procedures
As of the end of the period covered by this annual report, our management, with the participation of the persons acting in the capacity of principal executive officer (CEO) and principal financial officer (CFO), has performed an evaluation of the effectiveness of our disclosure controls and procedures within the meaning of Rules 13a-15 (e) and 15d-15(e) of the Exchange Act. Based upon this evaluation, our management has concluded that, as of February 28, 2015, our existing disclosure controls and procedures were effective. It should be noted that while the CEO and CFO believe that our disclosure controls and procedures provide a reasonable level of assurance that they are effective, they do not expect the disclosure controls and procedures to be capable of preventing all errors and fraud. A control system, no matter how well conceived or operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met.
Management’s Report on Internal Controls over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Our internal control system was designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation and fair presentation of its published consolidated financial statements. All internal control systems, no matter how well designed, have inherent limitations. Therefore, even those systems determined to be effective may not prevent or detect misstatements and can provide only reasonable assurance with respect to financial statement preparation and presentation. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate. Our management conducted an assessment of the design and operation effectiveness of our internal control over financial reporting as of February 28, 2015. In making this assessment, we used the criteria established within the Internal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on this assessment, our management has concluded that, as of February 28, 2015, our internal control over financial reporting was effective.
Changes in internal control over financial reporting
No changes were made to our internal controls over financial reporting that occurred during the three month period and fiscal year ended February 28, 2015 that have materially affected, or are reasonably likely to materially affect, our internal controls over financial reporting.
We qualify as an “emerging growth company” under Section 3(a)(80) of the Exchange Act, as a result of enactment of the Jumpstart Our Business Startups Act of 2012, or JOBS Act. Under the JOBS Act, emerging growth companies are exempt from Section 404(b) of the Sarbanes-Oxley Act of 2002, which generally requires that a public company’s registered public accounting firm provide an attestation report relating to management’s assessment of internal control over financial reporting. We qualify as an emerging growth company and therefore have not included in, or incorporated by reference into, this annual report such an attestation report as of the end of the period covered by this annual report.
|
Item 16.
|
[Reserved]
|
|
Item 16A.
|
Audit Committee Financial Expert
|
Our board of directors has determined that Mr. Valier Boivin is the “audit committee financial expert” within the meaning of “Item 16A – Audit Committee Financial Expert” of this Annual Report.
The Commission has indicated that the designation of Mr. Boivin as an audit committee financial expert does not make Mr. Boivin an “expert” for any purpose, impose any duties, obligations or liability on Mr. Boivin that are greater than those imposed on members of the audit committee and board of directors who do not carry this designation or affect the duties, obligations or liability of any other member of the audit committee or board of directors.
90
|
Item 16B.
|
Code of Ethics
|
The Board of Directors adopted a Code of Business Conduct and Ethics for its directors, officers and employees on May 31, 2007 which can be found on SEDAR at www.sedar.com and on the Corporation’s web site on www.neptunebiotech.com. A copy of the Code of Ethics and Conduct can also be obtained by contacting the Secretary of the Corporation. Since its adoption by the Board of Directors, any breach of the Code of Ethics must be brought to the attention of the Board of Directors by the Chief Executive Officer or other senior executive of the Corporation. No material change report has ever been filed which pertains to any conduct of a director or executive officer that constitutes a departure from the Code.
The Board of Directors also adopted an Insider Trading Program for its Directors, officers and employees and adopted recently a majority voting policy for the election of its proposed Director candidates at the Corporation’s annual Shareholder meeting.
|
Item 16C.
|
Principal Accountant Fees and Services
|
Audit Fees
“Audit fees” consist of fees for professional services for the audit of our annual financial statements, interim reviews and limited procedures on interim financial statements, securities filings and consultations on accounting or disclosure issues. For the fiscal year ended February 28, 2015, KPMG LLP, our external auditors, billed $99,500 to the Corporation for audit fees. For the fiscal year ended February 28, 2014, KPMG LLP billed $214,500 to the Corporation for audit fees.
Audit-Related Fees
“Audit-related fees” consist of fees for professional services that are reasonably related to the performance of the audit or review of our financial statements and which are not reported under “Audit Fees” above. For the fiscal year ended February 28, 2015, KPMG LLP, our external auditors, billed $10,475 to the Corporation. For the fiscal year ended February 28, 2014, KPMG LLP billed $14,000 to the Corporation.
Tax Fees
“Tax fees” consist of fees for professional services for tax compliance, tax advice and tax planning. KPMG LLP, our external auditors, billed a total of $27,400 to the Corporation for tax fees for the fiscal year ended February 28, 2015 and a total of $25,500 to the Corporation for tax fees for fiscal year ended February 28, 2014. Tax fees include, but are not limited to, preparation of tax returns.
All Other Fees
The “other fees” include all other fees billed for professional services other than those mentioned hereinabove. KPMG LLP, our external auditors, billed no fees as to this matter the fiscal years ended February 28, 2015 and February 28, 2014.
Pre-Approval Policies and Procedures
The Audit Committee approves all audit, audit-related services, tax services and other non-audit related services provided by the external auditors in advance of any engagement. Under the Sarbanes-Oxley Act of 2002, audit committees are permitted to approve certain fees for non-audit related services pursuant to a de minimus exception prior to the completion of an audit engagement. Non-audit related services satisfy the de minimus exception if the following conditions are met:
(a) that the aggregate amount of all non-audit services that were not pre-approved is reasonably expected to constitute no more than five per cent of the total amount of fees paid by the Corporation and its subsidiaries to the Corporation’s external auditors during the fiscal year in which the services are provided;
(b) that the Corporation or its subsidiaries, as the case may be, did not recognize the services as non-audit services at the time of the engagement; and
91
(c) that the services are promptly brought to the attention of the Audit Committee and approved, prior to the completion of the audit, by the Audit Committee or by one or more of its members to whom authority to grant such approvals had been delegated by the Audit Committee.
None of the services described above under “Principal Accountant Fees and Services” were approved by the Audit Committee pursuant to the de minimus exception.
|
Item 16D.
|
Exemptions from the Listing Standards for Audit Committees
|
Not applicable.
|
Item 16E.
|
Purchases of Equity Securities by the Issuer and Affiliated Purchasers
|
Not applicable.
|
Item 16F.
|
Change in Registrant’s Certifying Accountant
|
None.
|
Item 16G.
|
Corporation Governance
|
NASDAQ Marketplace Rule 5615(a)(3) permits a foreign private issuer to follow its home country practice in lieu of certain of the requirements of the Rule 5600 Series. A foreign private issuer that follows a home country practice in lieu of one or more provisions of the Rule 5600 Series is required to disclose in its annual report filed with the SEC, or on its website, each requirement of the Rule 5600 Series that it does not follow and describe the home country practice followed by the issuer in lieu of such NASDAQ corporate governance requirements.
We do not follow NASDAQ Marketplace Rule 5620(c), but instead follow our home country practice. The NASDAQ minimum quorum requirement under Rule 5620(c) for a meeting of shareholders is 33.33% of the outstanding shares of common voting stock. Our quorum requirement, as set forth in our by-laws, is that a quorum for a meeting of our holders of common shares is the attendance, in person or by proxy, of the shareholders representing 10% of our common shares. The foregoing is consistent with the laws, customs and practices in Québec and the rules and policies of the TSX-V.
|
Item 16H.
|
Mining Safety Disclosure
|
Not applicable.
PART III
|
Item 17.
|
Financial Statements
|
Financial Statements of Acasti Pharma Inc. for the years ended February 28, 2015, 2014 and 2013
92

|
KPMG LLP
|
Telephone (514) 840-2100
|
|
600 de Maisonneuve Blvd. West
|
Fax (514) 840-2187
|
|
Suite 1500
|
Internet www.kpmg.ca
|
|
Tour KPMG
|
|
|
Montréal (Québec) H3A 0A3
|
INDEPENDENT AUDITORS’ REPORT OF REGISTERED PUBLIC ACCOUNTING FIRM
To the Shareholders of Acasti Pharma Inc.
We have audited the accompanying financial statements of Acasti Pharma Inc., which comprise the statements of financial position as at February 28, 2015 and 2014, the statements of earnings and comprehensive loss, changes in equity and cash flows for each of the years in the three-year period ended February 28, 2015, and notes, comprising a summary of significant accounting policies and other explanatory information.
Management’s Responsibility for the Financial Statements
Management is responsible for the preparation and fair presentation of these financial statements in accordance with International Financial Reporting Standards as issued by the International Accounting Standards Board, and for such internal control as management determines is necessary to enable the preparation of financial statements that are free from material misstatement, whether due to fraud or error.
Auditors’ Responsibility
Our responsibility is to express an opinion on these financial statements based on our audits. We conducted our audits in accordance with Canadian generally accepted auditing standards and the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we comply with ethical requirements and plan and perform the audit to obtain reasonable assurance about whether the financial statements are free from material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the financial statements. The procedures selected depend on our judgment, including the assessment of the risks of material misstatement of the financial statements, whether due to fraud or error. In making those risk assessments, we consider internal control relevant to the entity’s preparation and fair presentation of the financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity’s internal control. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of accounting estimates made by management, as well as evaluating the overall presentation of the financial statements.
We believe that the audit evidence we have obtained in our audits is sufficient and appropriate to provide a basis for our audit opinion.
Opinion
In our opinion, the financial statements present fairly, in all material respects, the financial position of Acasti Pharma Inc. as at February 28, 2015 and 2014, and its financial performance and its cash flows for each of the years in the three-year period ended February 28, 2015 in accordance with International Financial Reporting Standards as issued by the International Accounting Standards Board.
May 27, 2015
Montréal, Canada
*CPA auditor, CA, public accountancy permit No. A119178
|
|
KPMG LLP is a Canadian limited liability partnership and a member firm of the KPMG
|
|
|
network of independent member firms affiliated with KPMG International Cooperative
|
|
|
("KPMG International"), a Swiss entity.
|
|
|
KPMG Canada provides services to KPMG LLP.
|
93
ACASTI PHARMA INC.
Financial Statements
Years ended February 28, 2015, 2014 and 2013
|
Financial Statements
|
|
|
Statements of Financial Position
|
1
|
|
Statements of Earnings and Comprehensive Loss
|
2
|
|
Statements of Changes in Equity
|
3
|
|
Statements of Cash Flows
|
5
|
|
Notes to Financial Statements
|
6
|
94
ACASTI PHARMA INC.
Statements of Financial Position
February 28, 2015 and 2014
|
February 28,
|
February 28,
|
|||||||
|
2015
|
2014
|
|||||||
|
Assets
|
||||||||
|
Current assets:
|
||||||||
|
Cash
|
$ | 1,310,556 | $ | 675,490 | ||||
|
Short-term investments (note 17 (e))
|
17,071,344 | 23,025,951 | ||||||
|
Trade and other receivables (note 4)
|
384,886 | 919,371 | ||||||
|
Receivable from corporation under common control
|
49,658 | 49,658 | ||||||
|
Receivable from parent corporation
|
– | 47,140 | ||||||
|
Tax credits receivable (note 6)
|
419,992 | 134,120 | ||||||
|
Inventories (note 7)
|
87,370 | 261,431 | ||||||
|
Prepaid expenses
|
318,457 | 703,497 | ||||||
| 19,642,263 | 25,816,658 | |||||||
|
Equipment (note 8)
|
69,937 | 38,941 | ||||||
|
Intangible assets (note 9)
|
17,495,905 | 19,776,204 | ||||||
|
Total assets
|
$ | 37,208,105 | $ | 45,631,803 | ||||
|
Liabilities and Equity
|
||||||||
|
Current liabilities:
|
||||||||
|
Trade and other payables (note 10)
|
$ | 1,083,847 | $ | 1,170,828 | ||||
|
Payable to parent corporation (note 5 (b))
|
538,531 | – | ||||||
| 1,622,378 | 1,170,828 | |||||||
|
Derivative warrant liabilities (notes 11 (d) and 19)
|
2,357,408 | 11,181,475 | ||||||
|
Total liabilities
|
3,979,786 | 12,352,303 | ||||||
|
Equity:
|
||||||||
|
Share capital (note 11 (a))
|
61,627,743 | 61,027,307 | ||||||
|
Warrants (note 11 (d))
|
– | 406,687 | ||||||
|
Contributed surplus
|
4,911,381 | 3,501,587 | ||||||
|
Deficit
|
(33,310,805 | ) | (31,656,081 | ) | ||||
|
Total equity
|
33,228,319 | 33,279,500 | ||||||
|
Commitments and contingencies (note 18)
|
||||||||
|
Subsequent event (note 22)
|
||||||||
|
Total liabilities and equity
|
$ | 37,208,105 | $ | 45,631,803 | ||||
See accompanying notes to financial statements.
On behalf of the Board:
|
/s/ Jerald Wenker
|
/s/Valier Boivin
|
|
Jerald Wenker
|
Valier Boivin
|
|
Chairman of the Board
|
Director
|
95
ACASTI PHARMA INC.
Statements of Earnings and Comprehensive Loss
Years ended February 28, 2015, 2014, and 2013
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Revenue from sales
|
$ | 270,615 | $ | 500,875 | $ |
724,196
|
||||||
|
Cost of sales (note 7)
|
(235,091 | ) | (291,853 | ) | (406,371 | ) | ||||||
|
Gross profit
|
35,524 | 209,022 | 317,825 | |||||||||
|
General and administrative expenses
|
(5,908,268 | ) | (6,711,533 | ) | (4,288,542 | ) | ||||||
|
Research and development expenses,
|
||||||||||||
|
net of tax credits of $264,270 (2014 - $269,591; 2013 - $370,259)
|
$ | (6,521,717 | ) | $ | (4,297,195 | ) | $ | (3,009,016 | ) | |||
|
Results from operating activities
|
(12,394,461 | ) | (10,799,706 | ) | (6,979,733 | ) | ||||||
|
Finance income (note 13)
|
10,743,797 | 813,842 | 90,058 | |||||||||
|
Finance costs (note 13)
|
(4,060 | ) | (1,625,785 | ) | (2,685 | ) | ||||||
|
Net finance income (cost)
|
10,739,737 | (811,943 | ) | 87,373 | ||||||||
|
Net loss and total comprehensive loss for the year
|
$ | (1,654,724 | ) | $ | (11,611,649 | ) | $ | (6,892,360 | ) | |||
|
Basic and diluted loss per share (note 15)
|
$ | (0.02 | ) | $ | (0.14 | ) | $ | (0.09 | ) | |||
|
Weighted average number of shares outstanding (note 15)
|
106,177,039 | 84,368,933 | 72,754,436 | |||||||||
See accompanying notes to financial statements
96
ACASTI PHARMA INC.
Statements of Changes in Equity
Years ended February 28, 2015, 2014 and 2013
|
Share capital
|
||||||||||||||||||||||||
|
Number
|
Dollar
|
Warrants
|
Contributed
surplus
|
Deficit
|
Total
|
|||||||||||||||||||
|
Balance, February 28, 2014
|
105,862,179 | $ | 61,027,307 | $ | 406,687 | $ | 3,501,587 | $ | (31,656,081 | ) | $ | 33,279,500 | ||||||||||||
|
Net loss and total comprehensive loss for the year
|
– | – | – | – | (1,654,724 | ) | (1,654,724 | ) | ||||||||||||||||
| 105,862,179 | 61,027,307 | 406,687 | 3,501,587 | (33,310,805 | ) | 31,624,776 | ||||||||||||||||||
|
Transactions with owners, recorded directly in equity
|
||||||||||||||||||||||||
|
Contributions by and distributions to owners
|
||||||||||||||||||||||||
|
Share-based payment
|
||||||||||||||||||||||||
|
transactions (note 14)
|
– | – | – | 1,553,543 | – | 1,553,543 | ||||||||||||||||||
|
Share options exercised (note 14)
|
200,000 | 50,000 | – | – | – | 50,000 | ||||||||||||||||||
|
RSUs released (note 14)
|
381,833 | 550,436 | – | (550,436 | ) | – | – | |||||||||||||||||
|
Expiration of warrants (note 11 (d))
|
– | – | (406,687 | ) | 406,687 | – | – | |||||||||||||||||
|
Total contributions by and distributions to owners
|
581,833 | 600,436 | (406,687 | ) | 1,409,794 | – | 1,603,543 | |||||||||||||||||
|
Balance at February 28, 2015
|
106,444,012 | $ | 61,627,743 | $ | – | $ | 4,911,381 | $ | (33,310,805 | ) | $ | 33,228,319 | ||||||||||||
|
Balance, February 28, 2013
|
73,107,538 | $ | 28,922,710 | $ | 406,687 | $ | 438,711 | $ | (20,044,432 | ) | $ | 9,723,676 | ||||||||||||
|
Net loss and total comprehensive loss for the year
|
– | – | – | – | (11,611,649 | ) | (11,611,649 | ) | ||||||||||||||||
| 73,107,538 | 28,922,710 | 406,687 | 438,711 | (31,656,081 | ) | (1,887,973 | ) | |||||||||||||||||
|
Transactions with owners, recorded directly in equity
|
||||||||||||||||||||||||
|
Contributions by and distributions to owners
|
||||||||||||||||||||||||
|
Public offering (note 11(b))
|
18,400,000 | 12,396,535 | – | – | – | 12,396,535 | ||||||||||||||||||
|
Private placement (note 11 (c))
|
1,616,542 | 2,067,605 | – | – | – | 2,067,605 | ||||||||||||||||||
|
Issuance of shares on
|
||||||||||||||||||||||||
|
royalty prepayment(note 18)
|
6,750,000 | 15,496,000 | – | – | – | 15,496,000 | ||||||||||||||||||
|
Share-based payment
|
||||||||||||||||||||||||
|
transactions (note 14)
|
– | – | – | 3,441,719 | – | 3,441,719 | ||||||||||||||||||
|
Warrants exercised
|
5,432,350 | 1,358,088 | – | – | – | 1,358,088 | ||||||||||||||||||
|
Share options exercised (note 14)
|
296,500 | 492,289 | – | (84,763 | ) | – | 407,526 | |||||||||||||||||
|
RSUs released (note 14)
|
259,249 | 294,080 | – | (294,080 | ) | – | – | |||||||||||||||||
|
Total contributions by and distributions to owners
|
32,754,641 | 32,104,597 | – | 3,062,876 | – | 35,167,473 | ||||||||||||||||||
|
Balance at February 28, 2014
|
105,862,179 | $ | 61,027,307 | $ | 406,687 | $ | 3,501,587 | $ | (31,656,081 | ) | $ | 33,279,500 | ||||||||||||
See accompanying notes to financial statements.
97
ACASTI PHARMA INC.
Statements of Changes in Equity
Years ended February 28, 2015, 2014 and 2013
| Share capital |
Contributed
|
|||||||||||||||||||||||
|
Number
|
Dollar
|
Warrants
|
surplus
|
Deficit
|
Total
|
|||||||||||||||||||
|
Balance, February 29, 2012
|
72,636,888 | $ | 28,614,550 | $ | 313,315 | $ | (1,306,451 | ) | $ | (13,152,072 | ) | $ | 14,469,342 | |||||||||||
|
Net loss and total comprehensive loss for the year
|
– | – | – | – | (6,892,360 | ) | (6,892,360 | ) | ||||||||||||||||
| 72,636,888 | 28,614,550 | 313,315 | (1,306,451 | ) | (20,044,432 | ) | 7,576,982 | |||||||||||||||||
|
Transactions with owners, recorded directly in equity
|
||||||||||||||||||||||||
|
Contributions by and distributions to owners
|
||||||||||||||||||||||||
|
Share-based payment transactions
|
– | – | 93,372 | 1,823,845 | – | 1,917,217 | ||||||||||||||||||
|
Warrants exercised
|
353,150 | 88,289 | – | – | – | 88,289 | ||||||||||||||||||
|
Share options exercised
|
117,500 | 219,871 | – | (78,683 | ) | – | 141,188 | |||||||||||||||||
|
Total contributions by and distributions to owners
|
470,650 | 308,160 | 93,372 | 1,745,162 | – | 2,146,694 | ||||||||||||||||||
|
Balance at February 28, 2013
|
73,107,538 | $ | 28,922,710 | $ | 406,687 | $ | 438,711 | $ | (20,044,432 | ) | $ | 9,723,676 | ||||||||||||
See accompanying notes to financial statements.
98
ACASTI PHARMA INC.
Statements of Cash Flows
Years ended February 28, 2015, 2014 and 2013
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Cash flows used in operating activities:
|
||||||||||||
|
Net loss for the year
|
$ | (1,654,724 | ) | $ | (11,611,649 | ) | $ | (6,892,360 | ) | |||
|
Adjustments:
|
||||||||||||
|
Depreciation of equipment
|
3,654 | 5,337 | 7,886 | |||||||||
|
Amortization of intangible asset
|
2,331,569 | 1,768,500 | 657,144 | |||||||||
|
Stock-based compensation
|
1,553,543 | 3,441,719 | 1,917,217 | |||||||||
|
Net finance (income) cost
|
(10,739,737 | ) | 811,943 | (87,373 | ) | |||||||
|
Realized foreign exchange gain (loss)
|
1,606 | (92,944 | ) | 12,669 | ||||||||
| (8,504,089 | ) | (5,677,094 | ) | (4,384,817 | ) | |||||||
|
Changes in non-cash operating working capital items:
|
||||||||||||
|
Trade and other receivables
|
534,485 | (468,533 | ) | (8,120 | ) | |||||||
|
Receivable from parent corporation and corporation under common control
|
47,140 | (47,140 | ) | – | ||||||||
|
Tax credits receivable
|
(285,872 | ) | 201,381 | 254,901 | ||||||||
|
Inventories
|
174,061 | (39,306 | ) | 377,331 | ||||||||
|
Prepaid expenses
|
385,040 | (686,806 | ) | 24,959 | ||||||||
|
Trade and other payables
|
(86,981 | ) | 463,945 | (288,779 | ) | |||||||
|
Payable to parent corporation
|
538,531 | (417,167 | ) | 995,832 | ||||||||
|
Royalties payable to parent corporation
|
– | (133,817 | ) | 479,801 | ||||||||
| 1,306,404 | (1,127,443 | ) | 1,835,925 | |||||||||
|
Net cash used in operating activities
|
(7,197,685 | ) | (6,804,537 | ) | (2,548,892 | ) | ||||||
|
Cash flows from (used in) investing activities:
|
||||||||||||
|
Interest received
|
40,995 | 98,132 | 1,778 | |||||||||
|
Acquisition of equipment
|
(34,650 | ) | (25,000 | ) | – | |||||||
|
Acquisition of intangible assets
|
(51,270 | ) | (123,610 | ) | (103,068 | ) | ||||||
|
Acquisition of short-term investments
|
(14,478,186 | ) | (25,395,800 | ) | – | |||||||
|
Maturity of short-term investments
|
22,149,888 | 6,000,000 | 2,000,000 | |||||||||
|
Net cash from (used in) investing activities
|
7,626,777 | (19,446,278 | ) | 1,898,710 | ||||||||
|
Cash flows from financing activities:
|
||||||||||||
|
Net proceeds from public offering (note 11 (b))
|
– | 21,953,200 | – | |||||||||
|
Net proceeds from private placement (note 11 (c))
|
– | 2,067,605 | – | |||||||||
|
Proceeds from exercise of warrants and options
|
50,000 | 972,177 | 229,477 | |||||||||
|
Share issue costs (note 18)
|
– | (29,000 | ) | – | ||||||||
|
Interest paid
|
(4,060 | ) | (975 | ) | (2,685 | ) | ||||||
|
Net cash from financing activities
|
45,940 | 24,963,007 | 226,792 | |||||||||
|
Foreign exchange gain on cash held in foreign currencies
|
160,034 | 766,730 | 30,148 | |||||||||
|
Net increase (decrease) in cash
|
635,066 | (521,078 | ) | (393,242 | ) | |||||||
|
|
||||||||||||
|
Cash, beginning of year
|
675,490 | 1,196,568 | 1,589,810 | |||||||||
|
Cash, end of year
|
$ | 1,310,556 | $ | 675,490 | $ | 1,196,568 | ||||||
|
Supplemental cash flow disclosure:
|
||||||||||||
|
Non-cash transactions:
|
||||||||||||
|
Issuance of common shares (note 18)
|
$ | – | $ | 15,525,000 | $ | – | ||||||
|
Royalties settled through
|
||||||||||||
|
issuance of shares (note 18)
|
– | 395,068 | – | |||||||||
|
Acquisition of intangible asset (note 18)
|
– | 15,129,932 | – | |||||||||
|
Exercise of warrants by Neptune
|
||||||||||||
|
applied against payable
|
– | 793,437 | – | |||||||||
See accompanying notes to financial statements.
99
ACASTI PHARMA INC.
Notes to Financial Statements
Years ended February 28, 2015, 2014 and 2013
1. Reporting entity
Acasti Pharma Inc. (the "Corporation") is incorporated under the Business Corporations Act (Québec) (formerly Part 1A of the Companies Act (Québec)). The Corporation is domiciled in Canada and its registered office is located at 545, Promenade du Centropolis, Laval, Québec, H7T 0A3. The Corporation is a subsidiary of Neptune Technologies and Bioressources Inc. (“Neptune”). The Corporation, the parent and NeuroBioPharm Inc. (“NeuroBioPharm”), a sister corporation, collectively referred to as the “group”.
On August 7, 2008, the Corporation commenced operations after having acquired from Neptune an exclusive worldwide license to use its intellectual property to develop, clinically study and market new pharmaceutical products to treat human cardiovascular conditions. Neptune’s intellectual property is related to the extraction of particular ingredients from marine biomasses, such as krill. The eventual products are aimed at applications in the over-the-counter medicine, medical foods and prescription drug markets.
Operations essentially consist in the development of new products and the conduct of clinical research studies on animals and humans. Almost all research and development, administration and capital expenditures incurred by the Corporation since the start of the operations are associated with the project described above.
The Corporation is subject to a number of risks associated with the successful development of new products and their marketing, the conduct of its clinical studies and their results, the meeting of development objectives set by Neptune in its license agreement, and the establishment of strategic alliances. The Corporation has incurred significant operating losses and negative cash flows from operations since inception. To date, the Corporation has financed its operations through public offering and private placement of common shares, proceeds from exercises of warrants, rights and options and research tax credits. To achieve the objectives of its business plan, the Corporation plans to establish strategic alliances, raise the necessary capital and make sales. It is anticipated that the products developed by the Corporation will require approval from the U.S Food and Drug Administration and equivalent organizations in other countries before their sale can be authorized. The ability of the Corporation to ultimately achieve profitable operations is dependent on a number of factors outside of the Corporation’s control.
2. Basis of preparation
|
|
(a)
|
Statement of compliance:
|
These financial statements have been prepared in accordance with International Financial Reporting Standards (“IFRS”) as issued by the International Accounting Standards Board (“IASB”).
The financial statements were authorized for issue by the Board of Directors on May 27, 2015.
|
|
(b)
|
Basis of measurement:
|
The financial statements have been prepared on the historical cost basis, except for:
|
·
|
Stock-based compensation which is measured pursuant to IFRS 2, Share-based payments (note 3(f) (ii)); and,
|
|
·
|
Derivative warrant liabilities measured at fair value on a recurring basis (note 19).
|
|
|
(c)
|
Functional and presentation currency:
|
These financial statements are presented in Canadian dollars, which is the Corporation’s functional currency.
|
|
(d)
|
Use of estimates and judgments:
|
The preparation of the financial statements in conformity with IFRS requires management to make judgments, estimates and assumptions that affect the application of accounting policies and the reported amounts of assets, liabilities, income and expenses. Actual results may differ from these estimates.
Estimates are based on the management’s best knowledge of current events and actions that the Corporation may undertake in the future. Estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimates are revised and in any future periods affected.
Critical judgments in applying accounting policies that have the most significant effect on the amounts recognized in the financial statements include the following:
|
·
|
Identification of triggering events indicating that the intangible assets might be impaired (Note 3 (e) (ii)).
|
100
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
2. Basis of preparation (continued):
|
|
(d)
|
Use of estimates and judgments (continued):
|
|
·
|
The use of the going concern basis of preparation of the financial statements. At each reporting period, management assesses the basis of preparation of the financial statements. These financial statements have been prepared on a going concern basis in accordance with IFRS. The going concern basis of presentation assumes that the Corporation will continue its operations for the foreseeable future and be able to realize its assets and discharge its liabilities and commitments in the normal course of business.
|
Assumptions and estimation uncertainties that have a significant risk of resulting in a material adjustment within the next financial year include the following:
|
·
|
Measurement of derivative warrant liabilities (Note 19) and stock-based compensation (Note 14).
|
|
·
|
Allocation of shared costs amongst the Neptune group companies (Note 5).
|
Also, management uses judgment to determine which research and development (“R&D”) expenses qualify for R&D tax credits and in what amounts. The Corporation recognizes the tax credits once it has reasonable assurance that they will be realized. Recorded tax credits are subject to review and approval by tax authorities and therefore, could be
different from the amounts recorded.
3. Significant accounting policies:
The accounting policies set out below have been applied consistently to all years presented in these financial statements.
|
|
(a)
|
Financial instruments:
|
|
|
(i)
|
Non-derivative financial assets:
|
The Corporation has the following non-derivative financial assets: cash, short-term investments and receivables.
The Corporation initially recognizes loans and receivables on the date that they are originated.
The Corporation derecognizes a financial asset when the contractual rights to the cash flows from the asset expire, or it transfers the rights to receive the contractual cash flows on the financial asset in a transaction in which substantially all the risks and rewards of ownership of the financial asset are transferred. Any interest in transferred financial assets that is created or retained by the Corporation is recognized as a separate asset or liability.
Financial assets and liabilities are offset and the net amount presented in the statements of financial position when, and only when, the Corporation has a legal right to offset the amounts and intends either to settle on a net basis or to realize the asset and settle the liability simultaneously.
Loans and receivables
Loans and receivables are financial assets with fixed or determinable payments that are not quoted in an active market. Such assets are recognized initially at fair value plus any directly attributable transaction costs. Subsequent to initial recognition, loans and receivables are measured at amortized cost using the effective interest method, less any impairment losses.
Loans and receivables comprise cash, short-term investments, and receivables with maturities of less than one year.
Cash and cash equivalents comprise cash balances and highly liquid investments purchased three months or less from maturity. Bank overdrafts that are repayable on demand form an integral part of the Corporation’s cash management and are included as a component of cash and cash equivalents for the purpose of the statements of cash flows.
|
|
(ii)
|
Non-derivative financial liabilities:
|
The Corporation initially recognizes debt securities issued and subordinated liabilities on the date that they are originated.
The Corporation derecognizes a financial liability when its contractual obligations are discharged, cancelled or expire.
The Corporation has the following non-derivative financial liabilities: trade and other payables and payables to parent corporation.
Such financial liabilities are recognized initially at fair value plus any directly attributable transaction costs. Subsequent to initial recognition, these financial liabilities are measured at amortized cost using the effective interest method.
101
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(a)
|
Financial instruments (continued):
|
|
|
(iii)
|
Share capital:
|
Common shares
Class A common shares are classified as equity. Incremental costs directly attributable to the issue of common shares and share options are recognized as a deduction from equity, net of any tax effects.
|
|
(iv)
|
Derivative financial instruments:
|
The Corporation has issued liability-classified derivatives over its own equity. Derivatives are recognized initially at fair value; attributable transaction costs are recognized in profit and loss as incurred. Subsequent to initial recognition, derivatives are measured at fair value, and all changes in their fair value are recognized immediately in profit or loss.
|
|
(v)
|
Other equity instruments:
|
Warrants, options and rights over the Corporation’s equity issued outside of share-based payment transactions that do not meet the definition of a liability instrument are recognized in equity.
|
|
(b)
|
Inventories:
|
Inventories are measured at the lower of cost and net realizable value. The cost of raw materials is based on the weighted-average cost method. The cost of finished goods and work in progress includes expenditures incurred in acquiring the inventories, production or conversion costs and other costs incurred in bringing them to their existing location and condition, as well as production overheads based on normal operating capacity.
Net realizable value is the estimated selling price in the ordinary course of business, less the estimated costs of completion and selling expenses.
|
|
(c)
|
Equipment:
|
|
|
(i)
|
Recognition and measurement:
|
Equipment is measured at cost less accumulated depreciation and accumulated impairment losses.
Cost includes expenditures that are directly attributable to the acquisition of the asset. The cost of self-constructed assets includes the cost of materials and direct labour, any other costs directly attributable to bringing the assets to a working condition for their intended use, the costs of dismantling and removing the items and restoring the site on which they are located and borrowing costs on qualifying assets.
Purchased software that is integral to the functionality of the related equipment is capitalized as part of that equipment.
When parts of an equipment have different useful lives, they are accounted for as separate items (major components) of equipment.
Gains and losses on disposal of equipment are determined by comparing the proceeds from disposal with the carrying amount of equipment, and are recognized net within ''other income or expenses'' in profit or loss.
|
|
(ii)
|
Subsequent costs:
|
The cost of replacing a part of an equipment is recognized in the carrying amount of the item if it is probable that the future economic benefits embodied within the part will flow to the Corporation, and its cost can be measured reliably. The carrying amount of the replaced part is derecognized. The costs of the day-to-day servicing of equipment are recognized in profit or loss as incurred.
102
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(c)
|
Equipment:
|
|
|
(iii)
|
Depreciation:
|
Depreciation is recognized in profit or loss on either a straight-line basis or a declining basis over the estimated useful lives of each part of an item of equipment, since this most closely reflects the expected pattern of consumption of the future economic benefits embodied in the asset.
The estimated useful lives and rates for the current and comparative years are as follows:
|
Assets
|
Method
|
Period/Rate
|
|
Furniture and office equipment
|
Declining balance
|
20% to 30%
|
|
Computer equipment
|
Straight-line
|
3 - 4 years
|
Depreciation methods, useful lives and residual values are reviewed at each financial year-end and adjusted prospectively if appropriate.
|
|
(d)
|
Intangible assets:
|
|
|
(i)
|
Research and development:
|
Expenditure on research activities, undertaken with the prospect of gaining new scientific or technical knowledge and understanding, is recognized in profit or loss as incurred.
Development activities involve a plan or design for the production of new or substantially improved products and processes. Development expenditure is capitalized only if development costs can be measured reliably, the product or process is technically and commercially feasible, future economic benefits are probable, and the Corporation intends to and has sufficient resources to complete development and to use or sell the asset. The expenditure capitalized includes the cost of materials, direct labour, overhead costs that are directly attributable to preparing the asset for its intended use, and borrowing costs on qualifying assets. Other development expenditures are recognized in profit or loss as incurred.
Capitalized development expenditure is measured at cost less accumulated amortization and accumulated impairment losses. As of the reporting years presented, the Corporation has not capitalized any development expenditure.
|
|
(ii)
|
Other intangible assets:
|
Patent costs
Patents for technologies that are no longer in the research phase are recorded at cost. Patent costs include legal fees to obtain patents and patent application fees. When the technology is still in the research phase, those costs are expensed as incurred.
Licenses
Licenses that are acquired by the Corporation and have finite useful lives are measured at cost less accumulated amortization and accumulated impairment losses.
|
|
(iii)
|
Subsequent expenditure:
|
Subsequent expenditure is capitalized only when it increases the future economic benefits embodied in the specific asset to which it relates. All other expenditures, including expenditure on internally generated goodwill and brands, are recognized in profit or loss as incurred.
103
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(d)
|
Intangible assets (continued):
|
|
|
(iv)
|
Amortization:
|
Amortization is calculated over the cost of the asset less its residual value.
Amortization is recognized in profit or loss on a straight-line basis over the estimated useful lives of intangible assets from the date that they are available for use, since this most closely reflects the expected pattern of consumption of the future economic benefits embodied in the asset. The estimated useful lives for the current and comparative years are as follows:
|
Assets
|
Period
|
|
Patents
|
20 years
|
|
License
|
8 to 14 years
|
|
|
(e)
|
Impairment:
|
|
|
(i)
|
Financial assets (including receivables):
|
A financial asset not carried at fair value through profit or loss is assessed at each reporting date to determine whether there is objective evidence that it is impaired. A financial asset is impaired if objective evidence indicates that a loss event has occurred after the initial recognition of the asset, and that the loss event had a negative effect on the estimated future cash flows of that asset that can be estimated reliably.
Objective evidence that financial assets are impaired can include default or delinquency by a debtor, restructuring of an amount due to the Corporation on terms that the Corporation would not consider otherwise, indications that a debtor or issuer will enter bankruptcy, or the disappearance of an active market for a security.
The Corporation considers evidence of impairment for receivables at both a specific asset and collective level. All individually significant receivables are assessed for specific impairment. All individually significant receivables found not to be specifically impaired are then collectively assessed for any impairment that has been incurred but not yet identified. Receivables that are not individually significant are collectively assessed for impairment by grouping together receivables with similar risk characteristics.
In assessing collective impairment, the Corporation uses historical trends of the probability of default, timing of recoveries and the amount of loss incurred, adjusted for management’s judgment as to whether current economic and credit conditions are such that the actual losses are likely to be greater or less than suggested by historical trends.
An impairment loss in respect of a financial asset measured at amortized cost is calculated as the difference between its carrying amount and the present value of the estimated future cash flows discounted at the asset’s original effective interest rate. Losses are recognized in profit or loss and reflected in an allowance account against receivables. When a subsequent event causes the amount of impairment loss to decrease, the decrease in impairment loss is reversed through profit or loss.
|
|
(ii)
|
Non-financial assets:
|
The carrying amounts of the Corporation’s non-financial assets, other than inventories and tax credits receivable are reviewed at each reporting date to determine whether there is any indication of impairment. If any such indication exists, then the asset’s recoverable amount is estimated.
The recoverable amount of an asset or cash-generating unit is the greater of its value in use and its fair value less costs to sell. In assessing value in use, the estimated future cash flows are discounted to their present value using a pre-tax discount rate that reflects current market assessments of the time value of money and the risks specific to the asset. For the purpose of impairment testing, assets that cannot be tested individually are grouped together into the smallest group of assets that generates cash inflows from continuing use that are largely independent of the cash inflows of other assets or groups of assets (the “cash-generating unit, or CGU”).
104
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(e)
|
Impairment (continued):
|
|
|
(ii)
|
Non-financial assets (continued):
|
The Corporation’s corporate assets do not generate separate cash inflows. If there is an indication that a corporate asset may be impaired, then the recoverable amount is determined for the CGU to which the corporate asset belongs.
An impairment loss is recognized if the carrying amount of an asset or its CGU exceeds its estimated recoverable amount. Impairment losses are recognized in profit or loss.
Impairment losses recognized in prior years are assessed at each reporting date for any indications that the loss has decreased or no longer exists. An impairment loss is reversed if there has been a change in the estimates used to determine the recoverable amount. An impairment loss is reversed only to the extent that the asset’s carrying amount does not exceed the carrying amount that would have been determined, net of depreciation or amortization, if no impairment loss had been recognized.
|
|
(f)
|
Employee benefits:
|
|
|
(i)
|
Short-term employee benefits:
|
Short-term employee benefit obligations are measured on an undiscounted basis and are expensed as the related service is provided.
A liability is recognized for the amount expected to be paid under short-term cash bonus or profit-sharing plans if the Corporation has a present legal or constructive obligation to pay this amount as a result of past service provided by the employee, and the obligation can be estimated reliably.
|
|
(ii)
|
Share-based payment transactions:
|
The grant date fair value of share-based payment awards granted to employees is recognized as an employee expense, with a corresponding increase in contributed surplus, over the period that the employees unconditionally become entitled to the awards. The grant date fair value takes into consideration market performance conditions when applicable. The amount recognized as an expense is adjusted to reflect the number of awards for which the related service and non-market vesting conditions are expected to be met, such that the amount ultimately recognized as an expense is based on the number of awards that do meet the related service and non-market performance conditions at the vesting date.
Share-based payment arrangements in which the Corporation receives goods or services as consideration for its own equity instruments are accounted for as equity-settled share-based payment transactions, regardless of how the equity instruments are obtained by the Corporation.
Share-based payment transactions include those initiated by Neptune for the benefit of administrators, officers, employees and consultants that provide services to the consolidated group. The Corporation is under no obligation to settle these arrangements and, therefore, also accounts for them as equity-settled share-based payment transactions.
The expense recognized by the Corporation under these arrangements corresponds to the estimated fraction of services that the grantees provide to the Corporation out of the total services they provide to the Neptune group of corporations.
|
|
(iii)
|
Termination benefits:
|
Termination benefits are recognized as an expense when the Corporation is committed demonstrably, without realistic possibility of withdrawal, to a formal detailed plan to either terminate employment before the normal retirement date, or to provide termination benefits as a result of an offer made to encourage voluntary redundancy.
Termination benefits for voluntary redundancies are recognized as an expense if the Corporation has made an offer of voluntary redundancy, it is probable that the offer will be accepted, and the number of acceptances can be estimated reliably. If benefits are payable more than 12 months after the reporting year, then they are discounted to their present value.
105
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(g)
|
Provisions:
|
A provision is recognized if, as a result of a past event, the Corporation has a present legal or constructive obligation that can be estimated reliably, and it is probable that an outflow of economic benefits will be required to settle the obligation. Provisions are determined by discounting the expected future cash flows at a pre-tax rate that reflects current market assessments of the time value of money and the risks specific to the liability. The unwinding of the discount is recognized as finance cost.
|
|
(i)
|
Onerous contracts:
|
A provision for onerous contracts is recognized when the expected benefits to be derived by the Corporation from a contract are lower than the unavoidable cost of meeting its obligations under the contract. The provision is measured at the present value of the lower of the expected cost of terminating the contract and the expected net cost of continuing with the contract. Before a provision is established, the Corporation recognizes any impairment loss on the assets associated with that contract.
|
|
(ii)
|
Contingent liability:
|
A contingent liability is a possible obligation that arises from past events and of which the existence will be confirmed only by the occurrence or non-occurrence of one or more uncertain future events not within the control of the Corporation; or a present obligation that arises from past events (and therefore exists), but is not recognized because it is not probable that a transfer or use of assets, provision of services or any other transfer of economic benefits will be required to settle the obligation; or the amount of the obligation cannot be estimated reliably.
|
|
(h)
|
Revenue:
Sale of goods:
|
Revenue from the sale of goods in the course of ordinary activities is measured at the fair value of the consideration received or receivable, net of returns. Revenue is recognized when the significant risks and rewards of ownership have been transferred to the buyer, recovery of the consideration is probable, the associated costs and possible return of goods can be estimated reliably, there is no continuing management involvement with the goods, and the amount of revenue can be measured reliably. If it is probable that discounts will be granted and the amount can be measured reliably, then the discount is recognized as a reduction of revenue as the sales are recognized.
The timing of the transfers of risks and rewards varies depending on the individual terms of the contract of sale.
|
|
(i)
|
Government grants:
|
Government grants consisting of investment tax credits are recorded as a reduction of the related expense or cost of the asset acquired. Government grants are recognized when there is reasonable assurance that the Corporation has met the requirements of the approved grant program and there is reasonable assurance that the grant will be received.
Grants that compensate the Corporation for expenses incurred are recognized in profit or loss in reduction thereof on a systematic basis in the same years in which the expenses are recognized. Grants that compensate the Corporation for the cost of an asset are recognized in profit or loss on a systematic basis over the useful life of the asset.
|
|
(j)
|
Lease payments:
|
Payments made under operating leases are recognized in profit or loss on a straight-line basis over the term of the lease. Lease incentives received are recognized as an integral part of the total lease expense, over the term of the lease.
Minimum lease payments made under finance leases are apportioned between the finance expense and the reduction of the outstanding liability. The finance expense is allocated to each year during the lease term so as to produce a constant periodic rate of interest on the remaining balance of the liability.
Contingent lease payments are accounted for in the year in which they are incurred.
106
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(k)
|
Foreign currency:
|
Transactions in foreign currencies are translated into the functional currency at exchange rates at the dates of the transactions. Monetary assets and liabilities denominated in foreign currencies at the reporting date are retranslated to the functional currency at the exchange rate at that date. The foreign currency gain or loss on monetary items is the difference between amortized cost in the functional currency at the beginning of the period, adjusted for effective interest and payments during the period, and the amortized cost in foreign currency translated at the exchange rate at the end of the reporting period. Foreign currency differences arising on retranslation are recognized in profit or loss.
|
|
(l)
|
Finance income and finance costs:
|
Finance income comprises interest income on funds invested and changes in the fair value of financial derivative liabilities at fair value through profit or loss. Interest income is recognized as it accrues in profit or loss, using the effective interest method.
Finance costs comprise interest expense on borrowings, unwinding of the discount on provisions, changes in the fair value of financial derivative liabilities at fair value through profit or loss, and impairment losses recognized on financial assets. Borrowing costs that are not directly attributable to the acquisition, construction or production of a qualifying asset are recognized in profit or loss using the effective interest method.
Foreign currency gains and losses are reported on a net basis.
The Corporation recognizes interest income as a component of investing activities and interest expense as a component of financing activities in the statements of cash flows.
|
|
(m)
|
Income tax:
|
Income tax expense comprises current and deferred taxes. Current and deferred taxes are recognized in profit or loss except to the extent that they relate to items recognized directly in equity or in other comprehensive income.
Current tax is the expected tax payable or receivable on the taxable income or loss for the year, using tax rates enacted or substantively enacted at the reporting date, and any adjustment to tax payable in respect of previous years.
Deferred tax is recognized in respect of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for taxation purposes. Deferred tax is not recognized for temporary differences arising from the initial recognition of assets or liabilities in a transaction that is not a business combination and that affects neither accounting nor taxable profit or loss. Deferred tax is measured at the tax rates that are expected to be applied to temporary differences when they reverse, based on the laws that have been enacted or substantively enacted by the reporting date. Deferred tax assets and liabilities are offset if there is a legally enforceable right to offset current tax liabilities and assets, and they relate to income taxes levied by the same tax authority on the same taxable entity, or on different tax entities, but they intend to settle current tax liabilities and assets on a net basis or their tax assets and liabilities will be realized simultaneously. A deferred tax asset is recognized for unused tax losses, tax credits and deductible temporary differences, to the extent that it is probable that future taxable profits will be available against which they can be utilized. Deferred tax assets are reviewed at each reporting date and are reduced to the extent that it is no longer probable that the related tax benefit will be realized.
|
|
(n)
|
Earnings per share:
|
The Corporation presents basic and diluted earnings per share (“EPS”) data for its Class A shares. Basic EPS is calculated by dividing the profit or loss attributable to the holders of Class A shares of the Corporation by the weighted average number of common shares outstanding during the year, adjusted for own shares held. Diluted EPS is determined by adjusting the profit or loss attributable to the holders of Class A shares and the weighted average number of Class A shares outstanding, adjusted for own shares held, for the effects of all dilutive potential common shares, which comprise warrants, rights and share options granted to employees.
|
|
(o)
|
Segment reporting:
|
An operating segment is a component of the Corporation that engages in business activities from which it may earn revenues and incur expenses. The Corporation has one reportable operating segment: the development and commercialization of pharmaceutical applications of its licensed rights for cardiovascular diseases. The majority of the Corporation’s assets are located in Canada.
107
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
3. Significant accounting policies (continued):
|
|
(p)
|
Changes in accounting policies:
|
Future accounting changes:
A number of new standards, and amendments to standards and interpretations, are not yet effective for the year ended February 28, 2015, and have not been applied in preparing these financial statements.
|
|
(i)
|
Financial instruments:
|
On July 24, 2014, the International Accounting Standards Board (IASB) issued the final version of IFRS 9, Financial Instruments, which addresses the classification and measurement of financial assets and liabilities, impairment and hedge accounting, replacing IAS 39, Financial Instruments: Recognition and Measurement. IFRS 9 is effective for annual periods beginning on or after January 1, 2018, with earlier adoption permitted. The Corporation has not yet assessed the impact of adoption of IFRS 9, and does not intend to early adopt IFRS 9 in its financial statements.
|
|
(ii)
|
Revenue:
|
On May 28, 2014 the IASB issued IFRS 15, Revenue from Contracts with Customers. IFRS 15 will replace IAS 18, Revenue, among other standards. The standard contains a single model that applies to contracts with customers and two approaches to recognizing revenue: at a point in time or over time. The model features a contract-based five-step analysis of transactions to determine whether, how much and when revenue is recognized. New estimates and judgmental thresholds have been introduced, which may affect the amount and/or timing of revenue recognized. The new standard applies to contracts with customers. The new standard is effective for annual periods beginning on or after January 1, 2018, with earlier adoption permitted. The Corporation has not yet assessed the impact of adoption of IFRS 15, and does not intend to early adopt IFRS 15 in its financial statements.
4. Trade and other receivables:
|
February 28,
2015
|
February 28,
2014
|
|||||||
|
Trade receivables
|
$ | 250,313 | $ | 395,128 | ||||
|
Sales taxes receivable
|
134,573 | 524,243 | ||||||
| $ | 384,886 | $ | 919,371 | |||||
The Corporation’s exposure to credit and currency risks related to trade and other receivables is presented in Note 17.
5. Related parties:
|
|
(a)
|
Administrative and research and development expenses:
|
The Corporation was charged by Neptune for certain costs incurred by Neptune for the benefit of the Corporation and for royalties, as follows:
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Administrative costs
|
$ | 1,617,108 | $ | 1,037,766 | $ | 943,264 | ||||||
|
Research and development costs, before tax credits
|
681,219 | 545,908 | 678,439 | |||||||||
|
Royalties (note 18)
|
– | 228,219 | 450,342 | |||||||||
| $ | 2,298,327 | $ | 1,811,893 | $ | 2,072,045 | |||||||
108
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
5. Related parties (continued):
|
|
(a)
|
Administrative and research and development expenses:
|
Where Neptune incurs specific incremental costs for the benefit of the Corporation, it charges those amounts directly. Costs that benefit more than one entity of the Neptune group are charged by allocating a fraction of costs incurred by Neptune that is commensurate to the estimated fraction of services or benefits received by each entity for those items.
These charges do not represent all charges incurred by Neptune that may have benefited the Corporation, because, amongst others, Neptune does not allocate certain common office expenses and does not charge interest on indebtedness. Also, these charges do not necessarily represent the cost that the Corporation would otherwise need to incur, should it not receive these services or benefits through the shared resources of Neptune or receive financing from Neptune. As at February 28, 2015, an amount of nil is included in prepaid expenses relating to these charges ($320,349 in 2014).
|
|
(b)
|
Revenue from sales:
|
The Corporation recognized sales to Neptune in the amount of nil during the years ended February 28, 2015 and 2014 ($41,000 in 2013). These transactions are in the normal course of operations.
|
|
(c)
|
Payable to parent corporation:
|
Payable to parent corporation has no specified maturity date for payment or reimbursement and does not bear interest.
|
|
(d)
|
Key management personnel compensation:
|
The key management personnel of the Corporation are the members of the Board of Directors and certain officers. They control 2% of the voting shares of the Corporation (2% in 2014 and 3% in 2013).
Key management personnel compensation includes the following for the years ended February 28, 2015, 2014 and 2013:
|
February 28,
2015
|
February 28,
2014
|
February 28,
2013
|
||||||||||
|
Short-term benefits
|
$ | 741,639 | $ | 680,319 | $ | 887,596 | ||||||
|
Severance
|
174,950 | – | – | |||||||||
|
Share-based compensation costs
|
1,339,361 | 2,439,254 | 1,504,471 | |||||||||
| $ | 2,255,950 | $ | 3,119,573 | $ | 2,392,067 | |||||||
6. Tax credits receivable:
Tax credits comprise research and development investment tax credits receivable from the provincial government which relate to qualifiable research and development expenditures under the applicable tax laws. The amounts recorded as receivables are subject to a government tax audit and the final amounts received may differ from those recorded.
Unrecognized federal tax credits may be used to reduce future income tax and expire as follows:
|
2029
|
$ | 11,000 | ||
|
2030
|
40,000 | |||
|
2031
|
45,000 | |||
|
2032
|
431,000 | |||
|
2033
|
441,000 | |||
|
2034
|
436,000 | |||
|
2035
|
542,000 | |||
| $ | 1,946,000 | |||
109
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
7. Inventories:
|
February 28,
|
February 28,
|
|||||||
|
2015
|
2014
|
|||||||
|
Raw materials
|
$ | 39,195 | $ | 39,753 | ||||
|
Work in progress
|
1,032 | 219,593 | ||||||
|
Finished goods
|
47,143 | 2,085 | ||||||
| $ | 87,370 | $ | 261,431 | |||||
For the year ended February 28, 2015, the cost of sales of $235,091 ($291,853 in 2014 and $406,371 in 2013) was comprised of inventory costs of $233,821 ($284,410 in 2014 and $391,821 in 2013) which consisted of raw materials, changes in work in progress and finished goods, and other costs of $1,270 ($7,443 in 2014 and $14,550 in 2013).
8. Equipment:
|
|
Furniture
and office
|
Computer
equipment
|
Deposit on
equipment
|
Total
|
||||||||||||
|
Cost:
|
||||||||||||||||
|
Balance at February 29, 2012 and February 28, 2013
|
$ | 58,706 | $ | 3,691 | $ | – | $ | 62,397 | ||||||||
|
Additions
|
– | – | 25,000 | 25,000 | ||||||||||||
|
Balance at February 28, 2014
|
58,706 | 3,691 | 25,000 | 87,397 | ||||||||||||
|
Additions
|
– | – | 34,650 | 34,650 | ||||||||||||
|
Balance at February 28, 2015
|
58,706 | 3,691 | 59,650 | 122,047 | ||||||||||||
|
Accumulated depreciation:
|
||||||||||||||||
|
Balance at February 29, 2012
|
32,781 | 2,452 | – | 35,233 | ||||||||||||
|
Depreciation for the year
|
6,952 | 934 | – | 7,886 | ||||||||||||
|
Balance at February 28, 2013
|
39,733 | 3,386 | – | 43,119 | ||||||||||||
|
Depreciation for the year
|
5,032 | 305 | – | 5,337 | ||||||||||||
|
Balance at February 28, 2014
|
44,765 | 3,691 | – | 48,456 | ||||||||||||
|
Depreciation for the year
|
3,654 | – | – | 3,654 | ||||||||||||
|
Balance at February 28, 2015
|
$ | 48,419 | $ | 3,691 | $ | – | $ | 52,110 | ||||||||
|
Net carrying amounts:
|
||||||||||||||||
| February 28, 2014 | $ | 13,941 | $ | – | $ | 25,000 | $ | 38,941 | ||||||||
| February 28, 2015 | 10,287 | – | 59,650 | 69,937 | ||||||||||||
Depreciation expense for the years ended February 28, 2015, 2014 and 2013 has been recorded in “general and administrative expenses” in the statements of earnings and comprehensive loss.
110
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
9. Intangible assets:
|
Patents
|
License
|
Total
|
||||||||||
|
Cost:
|
||||||||||||
|
February 29, 2012
|
$ | – | $ | 9,200,000 | $ | 9,200,000 | ||||||
|
Additions
|
103,068 | – | 103,068 | |||||||||
|
Balance at February 28, 2013
|
103,068 | 9,200,000 | 9,303,068 | |||||||||
|
Additions (note 18)
|
123,610 | 15,129,932 | 15,253,542 | |||||||||
|
Balance at February 28, 2014
|
226,678 | 24,329,932 | 24,556,610 | |||||||||
|
Additions
|
51,270 | – | 51,270 | |||||||||
|
Balance at February 28, 2015
|
277,948 | 24,329,932 | 24,607,880 | |||||||||
|
Accumulated amortization:
|
||||||||||||
|
Balance at February 29, 2012
|
– | 2,354,762 | 2,354,762 | |||||||||
|
Amortization for the year
|
– | 657,144 | 657,144 | |||||||||
|
Balance at February 28, 2013
|
– | 3,011,906 | 3,011,906 | |||||||||
|
Amortization for the year
|
906 | 1,767,594 | 1,768,500 | |||||||||
|
Balance at February 28, 2014
|
906 | 4,779,500 | 4,780,406 | |||||||||
|
Amortization for the year
|
8,741 | 2,322,828 | 2,331,569 | |||||||||
|
Balance at February 28, 2015
|
$ | 9,647 | $ | 7,102,328 | $ | 7,111,975 | ||||||
|
Net carrying amounts:
|
||||||||||||
|
February 28, 2014
|
$ | 225,772 | $ | 19,550,432 | $ | 19,776,204 | ||||||
|
February 28, 2015
|
268,301 | 17,227,604 | 17,495,905 | |||||||||
Amortization expense for the years ended February 28, 2015, 2014 and 2013 has been recorded in “general and administrative expenses” in the statements of earnings and comprehensive loss.
10. Trade and other payables:
|
February 28,
|
February 28,
|
|||||||
|
2015
|
2014
|
|||||||
|
Trade payables
|
$ | 246,516 | $ | 319,683 | ||||
|
Accrued liabilities and other payables
|
661,625 | 613,526 | ||||||
|
Employee salaries and benefits payable
|
175,706 | 237,619 | ||||||
| $ | 1,083,847 | $ | 1,170,828 | |||||
The Corporation’s exposure to currency and liquidity risks related to trade and other payables is presented in Note 17.
111
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
11. Capital and other components of equity
|
|
(a)
|
Share capital:
|
Authorized capital stock:
Unlimited number of shares:
|
|
Ø
|
Class A shares, voting (one vote per share), participating and without par value
|
|
|
Ø
|
Class B shares, voting (ten votes per share), non-participating, without par value and maximum annual non-cumulative dividend of 5% on the amount paid for said shares. Class B shares are convertible, at the holder’s discretion, into Class A shares, on a one-for-one basis, and Class B shares are redeemable at the holder’s discretion for $0.80 per share, subject to certain conditions. 1
|
|
|
Ø
|
Class C shares, non-voting, non-participating, without par value and maximum annual non-cumulative dividend of 5% on the amount paid for said shares. Class C shares are convertible, at the holder’s discretion, into Class A shares, on a one-for-one basis, and Class C shares are redeemable at the holder’s discretion for $0.20 per share, subject to certain conditions. 1
|
|
|
Ø
|
Class D and E shares, non-voting, non-participating, without par value and maximum monthly non-cumulative dividend between 0.5% and 2% on the amount paid for said shares. Class D and E shares are convertible, at the holder’s discretion, into Class A shares, on a one-for-one basis, and Class D and E shares are redeemable at the holder’s discretion, subject to certain conditions. 1
|
1 None issued and outstanding
|
|
(b)
|
Public offering:
|
On December 3, 2013, the Corporation closed a public offering issuing 18,400,000 units of Acasti (“Units”) at a price of US$1.25 per Unit for gross proceeds of $24,492,700 (US$23,000,000). Each Unit consists of one Class A share and one Common Share purchase warrant (“Warrant”) of Acasti. Each Warrant entitles the holder to purchase one Class A share at an exercise price of US$1.50, subject to adjustment, at any time until December 3, 2018.
The Warrants forming part of the Units are derivative liabilities (“Derivative warrant liabilities”) for accounting purposes due to the currency of the exercise price being different from the Corporation’s functional currency. The proceeds of the offering are required to be split between the Derivative warrant liabilities and the equity-classified Class A share at the time of issuance of the Units. The fair value of the Derivative warrant liabilities at the time of issuance was determined to be $10,674,045 and the residual of the proceeds was allocated to the Class A share. Total issue costs related to this transaction amounted to $2,539,500. The issue costs have been allocated between the Warrants and Class A shares based on relative value. The portion allocated to the Warrants was recognized in finance costs whereas the portion allocated to Class A shares was recognized as a reduction to share capital.
The fair value of the public offering warrants 2014 was estimated according to the Black-Scholes option pricing model and based on the following assumptions:
|
February 28, 2015
|
February 28, 2014
|
|||||||
|
Exercise price
|
$ | US1.50 | $ | US1.50 | ||||
|
Share price
|
$ | 0.55 | $ | 1.27 | ||||
|
Dividend
|
– | – | ||||||
|
Risk-free interest
|
1.20 | % | 1.41 | % | ||||
|
Estimated life
|
3.76 years
|
4.76 years
|
||||||
|
Expected volatility
|
62.94 | % | 66.47 | % | ||||
The fair value of the Warrants issued was determined to be $0.13 per warrant as at February 28, 2015 ($0.61 per warrant – 2014). Changes in the fair value of the Warrants are recognized in finance income or costs.
112
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
11. Capital and other components of equity (continued):
|
|
(c)
|
Private placement 2014:
|
On February 7, 2014, the Corporation closed a private placement financing for gross proceeds of $2,150,000 from The Fiera Capital QSSO II Investment Fund Inc. for 1,616,542 Units at $1.33 per Unit. Each Unit consists of one Class A share and one Common Share purchase warrant (“Warrant”) of Acasti. Each Warrant entitles the holder to purchase one Class A share at an exercise price of $1.60, subject to adjustment, at any time until December 3, 2018. The Class A shares and Warrants are equity-classified for accounting purposes. The proceeds were allocated to Share Capital. Total issue costs related to this transaction amounted to $82,395 and were recognized as a reduction to share capital.
|
|
(d)
|
Warrants:
|
The warrants of the Corporation are composed of the following as at February 28, 2015, 2014 and 2013:
|
February 28,
|
February 28,
|
|||||||||||||||
|
2015
|
2014
|
|||||||||||||||
|
Number
|
Number
|
|||||||||||||||
|
outstanding
|
Amount
|
outstanding
|
Amount
|
|||||||||||||
|
Liability
|
||||||||||||||||
|
Series 8 Public offering warrants 2014 (b)
|
18,400,000 | $ | 2,357,408 | 18,400,000 | $ | 11,181,475 | ||||||||||
| 18,400,000 | 2,357,408 | 18,400,000 | 11,181,475 | |||||||||||||
|
Equity
|
||||||||||||||||
|
Private placement warrants
|
||||||||||||||||
|
Series 9 Private placement warrants 2014 (c)
|
1,616,542 | – | 1,616,542 | – | ||||||||||||
|
Series 6 warrants – expired unexercised February 10, 2015
|
– | – | 375,000 | 306,288 | ||||||||||||
|
Series 7 warrants – expired unexercised February 10, 2015
|
– | – | 375,000 | 100,399 | ||||||||||||
| 1,616,542 | $ | – | 2,366,542 | $ | 406,687 | |||||||||||
|
February 28,
|
||||||||||||||||
| 2013 | ||||||||||||||||
|
Number
|
||||||||||||||||
|
outstanding
|
Amount
|
|||||||||||||||
|
Liability
|
||||||||||||||||
|
Series 8 Public offering warrants 2014 (b)
|
– | $ | – | |||||||||||||
| – | – | |||||||||||||||
|
Equity
|
||||||||||||||||
|
Series 4 warrants
|
5,432,350 | – | ||||||||||||||
|
Private placement warrants
|
||||||||||||||||
|
Series 9 Private placement warrants 2014 (c)
|
– | – | ||||||||||||||
|
Series 6 warrants – expired unexercised February 10, 2015
|
375,000 | 306,288 | ||||||||||||||
|
Series 7 warrants – expired unexercised February 10, 2015
|
375,000 | 100,399 | ||||||||||||||
| 6,182,350 | $ | 406,687 | ||||||||||||||
113
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
12. Personnel expenses:
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Salaries and other short-term employee benefits
|
$ | 1,618,049 | 1,368,141 | $ | 1,486,391 | |||||||
|
Share-based compensation
|
1,553,543 | 3,423,243 | 1,871,224 | |||||||||
| $ | 3,171,592 | $ | 4,791,384 | $ | 3,357,615 | |||||||
Share-based compensation does not include compensation to consultants. For the year ended February 28, 2015, the share-based compensation to consultants is nil (2014 - $18,476 and 2013 $45,993).
13. Finance income and finance costs:
|
|
(a)
|
Finance income:
|
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Interest income
|
$ | 87,009 | $ | 32,256 | 47,241 | |||||||
|
Foreign exchange gain
|
1,832,721 | 781,586 | 42,817 | |||||||||
|
Change in fair value of Derivative warrant liabilities (Note 11 (b))
|
8,824,067 | – | – | |||||||||
| $ | 10,743,797 | $ | 813,842 | $ | 90,058 | |||||||
|
|
(b)
|
Finance costs:
|
|
February 28,
|
February 28,
|
February 28,
|
||||||||||
|
2015
|
2014
|
2013
|
||||||||||
|
Interest charges
|
$ | (4,060 | ) | $ | (975 | ) | $ | (2,685 | ) | |||
|
Warrants issue cost (Note 11 (b))
|
– | (1,117,380 | ) | – | ||||||||
|
Change in fair value of Derivative warrant liabilities (Note 11 (b))
|
– | (507,430 | ) | – | ||||||||
| $ | (4,060 | ) | $ | (1,625,785 | ) | $ | (2,685 | ) | ||||
14. Share-based payments:
At February 28, 2015, the Corporation has the following share-based payment arrangements:
|
|
(a)
|
Corporation stock option plan:
|
The Corporation has established a stock option plan for directors, officers, employees and consultants of the Corporation. The plan provides for the granting of options to purchase Acasti Class A shares. The exercise price of the stock options granted under this plan is not lower than the closing price of the shares listed on the eve of the grant. Under this plan, the maximum number of options that can be issued is 10% of the number of Acasti Class A shares issued and outstanding from time to time. The terms and conditions for acquiring and exercising options are set by the Corporation’s Board of Directors, subject, among others, to the following limitations: the term of the options cannot exceed ten years and every stock option granted under the stock option plan will be subject to conditions no less restrictive than a minimum vesting period of 18 months, a gradual and equal acquisition of vesting rights at least on a quarterly basis. The total number of shares issued to a single person cannot exceed 5% of the Corporation’s total issued and outstanding shares, with the maximum being 2% for any one consultant.
114
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
14. Share-based payments (continued):
|
|
(a)
|
Corporation stock option plan (continued):
|
Activities within the plan are detailed as follows:
| Year ended | Year ended | |||||||||||||||
| February 28, 2015 | February 28, 2014 | |||||||||||||||
|
Weighted average
|
Number of
|
Weighted average
|
Number or
|
|||||||||||||
|
exercise price
|
options
|
exercise price
|
options
|
|||||||||||||
|
Outstanding at beginning of year
|
$ | 1.57 | 4,911,000 | $ | 1.55 | 5,216,250 | ||||||||||
|
Granted
|
0.95 | 512,500 | 2.23 | 297,500 | ||||||||||||
|
Exercised
|
0.25 | (200,000 | ) | 1.37 | (296,500 | ) | ||||||||||
|
Forfeited
|
1.49 | (227,250 | ) | 2.06 | (306,250 | ) | ||||||||||
|
Expired
|
1.8 | (100,000 | ) | – | – | |||||||||||
|
Cancelled (note 18)
|
1.75 | (600,000 | ) | – | – | |||||||||||
|
Outstanding at end of year
|
$ | 1.53 | 4,296,250 | $ | 1.57 | 4,911,000 | ||||||||||
|
Exercisable at end of year
|
$ | 1.55 | 3,320,375 | $ | 1.39 | 3,412,165 | ||||||||||
| Year ended | ||||||||||||||||
| February 28, 2013 | ||||||||||||||||
|
Weighted average
|
Number or
|
|||||||||||||||
|
exercise price
|
options
|
|||||||||||||||
|
Outstanding at beginning of year
|
$ | 1.15 | 3,347,500 | |||||||||||||
|
Granted
|
2.14 | 2,350,000 | ||||||||||||||
|
Exercised
|
1.20 | (117,500 | ) | |||||||||||||
|
Forfeited
|
1.8 | (363,750 | ) | |||||||||||||
|
Outstanding at end of year
|
$ | 1.55 | 5,216,250 | |||||||||||||
|
Exercisable at end of year
|
$ | 1.14 | 2,421,832 | |||||||||||||
| 2015 | ||||||||||||||||
| Options outstanding | Exercisable options | |||||||||||||||
|
Weighted
|
Weighed
|
|||||||||||||||
|
remaining
|
Number of
|
average
|
Number of
|
|||||||||||||
|
contractual life
|
options
|
exercise price
|
options
|
|||||||||||||
|
Exercise price
|
outstanding
|
outstanding
|
$ |
exercisable
|
||||||||||||
|
$0.25 - $1.00
|
3.93 | 662,500 | 0.25 | 432,500 | ||||||||||||
|
$1.01 - $1.50
|
1.46 | 1,891,250 | 1.39 | 1,561,875 | ||||||||||||
|
$1.51 - $2.00
|
1.88 | 15,000 | 1.75 | 7,500 | ||||||||||||
|
$2.01 - $2.50
|
1.89 | 1,672,500 | 2.13 | 1,264,750 | ||||||||||||
|
$2.51 - $2.75
|
0.82 | 55,000 | 2.75 | 53,750 | ||||||||||||
| 2 | 4,296,250 | 1.55 | 3,320,375 | |||||||||||||
115
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
14. Share-based payments (continued):
|
|
(a)
|
Corporation stock option plan (continued):
|
The fair value of options granted has been estimated according to the Black-Scholes option pricing model and based on the weighted average of the following assumptions for options granted during the year:
|
2015
|
2014
|
2013
|
||||||||||
|
Exercise price
|
$ | 0.95 | $ | 2.23 | $ | 2.14 | ||||||
|
Share price
|
$ | 0.92 | $ | 1.88 | $ | 2.13 | ||||||
|
Dividend
|
– | – | – | |||||||||
|
Risk-free interest
|
1.14 | % | 1.11 | % | 1.32 | % | ||||||
|
Estimated life
|
3.00 years | 2.49 years | 4.04 years | |||||||||
|
Expected volatility
|
60.34 | % | 64.81 | % | 71.48 | % | ||||||
The weighted average of the fair value of the options granted to employees during the year ended February 28, 2015 is $0.35 (2014 - $0.67 and 2013 - $1.14). There were no options granted to non-employees during the years ended February 28, 2015, 2014 and 2013.
The weighted average share price at the date of exercise for share options exercised during the year ended February 28, 2015 was $0.92 (2014 - $3.77 and 2013 - $2.44). The portion of services employees provided to the Corporation was estimated to be 50% of services provided to the group (2014 – 49% and 2013 – 50%). Accordingly, stock-based compensation recognized under this plan amounted to $525,826 for the year ended February 28, 2015 (2014 - $501,479 and 2013 - $977,690).
|
|
(b)
|
Corporation equity incentive plan:
|
The Corporation established an equity incentive plan for employees, directors and consultants of the group. The plan provides for the issuance of restricted share units, performance share units, restricted shares, deferred share units and other share-based awards, subject to restricted conditions as may be determined by the Board of Directors. Upon fulfillment of the restricted conditions, as the case may be, the plan provides for settlement of the outstanding awards through shares.
The Corporation’s RSUs vest gradually over time with an expiry date of no later than January 15, 2017, based on a specific rate, depending on each holder’s category. The fair value of the APO RSUs is determined to be the share price at date of grant and is recognized as stock-based compensation, through contributed surplus, over the vesting period. The fair value of the RSUs granted was $2.89 per unit.
Activities within the plan are detailed as follows:
|
2015
|
2014
|
|||||||
|
RSUs outstanding at beginning of year
|
775,001 |
‒
|
||||||
|
Granted
|
– | 1,060,000 | ||||||
|
Released
|
(381,833 | ) | (259,249 | ) | ||||
|
Forfeited
|
(18,334 | ) | (25,750 | ) | ||||
|
Cancelled (note 18)
|
(190,834 | ) | – | |||||
|
RSUs outstanding at end of year
|
184,000 | 775,001 | ||||||
The portion of services employees provided to the Corporation was estimated to be 43% of services provided to the group (2014 – 44%). Accordingly, stock-based compensation recognized under this plan amounted to $466,370 for the year ended February 28, 2015 (2014 – $745,556).
116
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
14. Share-based payments (continued):
|
|
(c)
|
Neptune stock-based compensation plan:
|
Neptune maintains various stock-based compensation plans for the benefit of directors, officers, employees and consultants that provide services to its consolidated group, including the Corporation. The Corporation records as stock-based compensation expense a portion of the expense being recorded by Neptune that is commensurate to the fraction of overall services that the grantees provide directly to the Corporation.
|
|
(i)
|
Neptune stock options:
|
During the year ended February 28, 2015, Neptune granted 2,805,000 Neptune stock options to group employees (2014 – 1,640,000 and 2013 – 5,520,000). The options granted are vesting over a minimum period of 18 months, subject to continued service. The fair value of the options granted has been estimated according to the Black-Scholes option pricing model based on the following weighted average assumptions:
|
2015
|
2014
|
2013
|
||||||||||
|
Exercise price
|
$ | 2.36 | $ | 3.11 | $ | 3.23 | ||||||
|
Share price
|
$ | 2.32 | $ | 2.94 | $ | 3.06 | ||||||
|
Dividend yield
|
– | – | – | |||||||||
|
Risk-free interest rate
|
1.04 | % | 0.50 | % | 1.15 | % | ||||||
|
Estimated life
|
2.79 years
|
1.99 years
|
2.71 years
|
|||||||||
|
Expected volatility
|
58.42 | % | 64.42 | % | 65.18 | % | ||||||
The weighted average of the fair value of the options granted during the year is $0.88 per share (2014 - $0.84 and 2013 -$1.15). The portion of services provided to the Corporation was estimated to be 5% of the total services provided to the group (2014 - 18% and 2013 - 13%), representing stock-based compensation in the amount of $72,112 for the year ended February 28, 2015 (2014 - $782,285 and 2013 - $663,484).
|
|
(ii)
|
Neptune equity incentive plan:
|
Neptune has established an equity incentive plan for employees, directors and consultants of the group. The plan provides for the issuance of restricted share units, performance share units, restricted shares, deferred share units and other share-based awards, subject to restricted conditions as may be determined by the Board of Directors. Upon fulfillment of the restricted conditions, as the case may be, the plan provides for settlement of the outstanding awards through shares.
Neptune RSUs vest gradually overtime with an expiry date of no later than January 15, 2017, based on a specific rate, depending on each holder’s category. The fair value of the RSUs is determined to be the share price at date of grant and is recognized as stock-based compensation, through contributed surplus, over the vesting period. The fair value of the RSUs granted was $3.32 per unit.
The portion of services provided to the Corporation was estimated to be 35% of the total services provided to the group (2014 – 30%), representing stock-based compensation in the amount of $337,061 for the year ended February 28, 2015 (2014 – $832,261).
|
|
(iii)
|
Neptune-owned NeuroBioPharm warrants and call-options:
|
On February 20, 2015, Neptune and NeuroBioPharm completed an arrangement agreement (the “Arrangement”) which resulted in the direct acquisition by Neptune of all issued and outstanding shares of NeuroBioPharm. Holders of options, warrants or call-options convertible into Class A shares of NeuroBioPharm will maintain equivalent rights to receive common shares of Neptune upon exercise, as adjusted under the Arrangement to reflect the conversion ratio of the Class A shares of NeuroBioPharm, which was determined to be 21.5.
The stock-based compensation recognized for services provided to the Corporation amounts to $737 for the year ended February 28, 2015 (2014 - $2,969 and 2013 - $24,415).
117
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
14. Share-based payments (continued):
|
|
(c)
|
Neptune stock-based compensation plan (continued):
|
|
|
(iv)
|
Neptune-owned Acasti warrants:
|
During the years ended February 28, 2015, 2014 and 2013, no rights were granted over Neptune-owned Acasti warrants or shares to group employees. The rights granted in the year ended February 29, 2012 had a weighted average exercise price of $1.42 per share and were vesting gradually until February 10, 2015, subject to continued service or having reached four years of continued service for directors.
The portion of services those employees provide to the Corporation was estimated to be 100% of the total services they provide to the group (2014 - 100% and 2013 – 88%), representing stock-based compensation in the amount of nil for the year ended February 28, 2015 (2014 - $1,471 and 2013 - $144,438).
|
|
(v)
|
Neptune-owned Acasti call-options:
|
During the year ended February 28, 2014, Neptune granted 1,975,000 call-options on Acasti shares to group employees (2013 – 2,345,000). There were no grants in 2015. The fair value of the call-options granted during the year has been estimated according to the Black-Scholes option pricing model based on the weighted average of the following assumptions:
|
2014
|
2013
|
|||||||
|
Exercise price
|
$ | 3.00 | $ | 2.75 | ||||
|
Share price
|
$ | 2.89 | $ | 2.69 | ||||
|
Dividend yield
|
– | – | ||||||
|
Risk-free interest rate
|
1.26 | % | 1.13 | % | ||||
|
Estimated life
|
2.45 years
|
2.89 years
|
||||||
|
Expected volatility
|
62.63 | % | 82.25 | % | ||||
The weighted average of the fair value of the call-options granted to employees during the year ended February 28, 2014 is $1.08 per share (2013 - $1.39). The portion of services those employees provide to the Corporation was estimated to be 35% of the total services they provide to the group (2014 – 36% and 2013 – 26%), representing stock-based compensation in the amount of $141,490 for the year ended February 28, 2015 (2014 - $562,407 and 2013 - $107,190).
|
|
(d)
|
NeuroBioPharm Share Bonus plan:
|
NeuroBioPharm had established an equity incentive plan for group employees, directors and consultants of NeuroBioPharm. The plan provided for the issuance of share bonus awards, under restricted conditions as may be determined by the Board of Directors. Upon fulfillment of the restricted conditions, as the case may be, the plan provided for settlement of the award through shares.
As part of the Arrangement with Neptune on February 20, 2015, the release of all NeuroBioPharm share bonus awards was accelerated and therefore there were no such awards outstanding as at February 28, 2015. The stock-based compensation expense related to this plan was also accelerated accordingly. The stock-based compensation recognized for services provided to the Corporation under this plan amounts to $9,947 for the year ended February 28, 2015 (2014 - $13,291 and 2013 - nil).
15. Loss per share:
The calculation of basic loss per share at February 28, 2015 was based on the net loss attributable to holders of Class A shares of the Corporation of $1,654,724 (2014 - $11,611,649, 2013 - $6,892,360) and a weighted average number of common shares outstanding of 106,177,039 (2014 – 84,368,933, 2013 – 72,754,436).
Diluted loss per share was the same amount as basic loss per share, as the effect of options, RSUs and warrants would have been anti-dilutive, because the Corporation incurred losses in each of the years presented. All outstanding options, RSUs and warrants could potentially be dilutive in the future.
118
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
16. Income taxes:
Deferred tax expense:
|
2015
|
2014
|
2013
|
||||||||||
|
Origination and reversal of temporary differences
|
$ | 2,221,229 | $ | 1,932,370 | $ | 1,235,673 | ||||||
|
Change in unrecognized deductible temporary differences
|
(2,221,229 | ) | (1,932,370 | ) | (1,235,673 | ) | ||||||
|
Deferred tax expense
|
$ | – | $ | – | $ | – | ||||||
Reconciliation of effective tax rate:
|
2015
|
2014
|
2013
|
||||||||||
|
Loss before income taxes
|
$ | (1,654,724 | ) | $ | (11,611,649 | ) | $ | (6,892,360 | ) | |||
|
Income tax at the combined Canadian statutory rate of 26.9%
|
$ | (445,121 | ) | $ | (3,123,534 | ) | $ | (1,854,045 | ) | |||
|
Increase resulting from:
|
||||||||||||
|
Change in unrecognized deductible temporary differences
|
2,221,229 | 1,932,370 | 1,235,673 | |||||||||
|
Non-deductible stock-based compensation
|
417,903 | 925,823 | 515,732 | |||||||||
|
Non-deductible change in fair value
|
(2,373,674 | ) | 136,499 | – | ||||||||
|
Permanent differences and other
|
179,663 | 128,842 | 102,640 | |||||||||
|
Total tax expense
|
$ | – | $ | – | $ |
‒
|
||||||
Unrecognized deferred tax assets:
At February 28, 2015 and 2014, the deferred tax assets, which have not been recognized in these financial statements because the criteria for recognition of these assets were not met, were as follows:
|
2015
|
2014
|
|||||||
|
Tax losses carried forward
|
$ | 4,492,000 | $ | 3,295,000 | ||||
|
Research and development expenses
|
3,332,000 | 2,196,000 | ||||||
|
Property, plant and equipment and intangible assets
|
282,000 | 240,000 | ||||||
|
Other deductible temporary differences
|
441,000 | 594,000 | ||||||
|
Unrecognized deferred tax assets
|
$ | 8,547,000 | $ | 6,325,000 | ||||
119
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
16. Income taxes (continued):
As at February 28, 2015, the amounts and expiry dates of tax attributes and temporary differences, which are available to reduce future years’ taxable income, were as follows:
|
Federal
|
Provincial
|
|||||||
|
Tax losses carried forward
|
||||||||
|
2029
|
$ | 714,000 | $ | 714,000 | ||||
|
2030
|
1,627,000 | 1,621,000 | ||||||
|
2031
|
2,071,000 | 2,063,000 | ||||||
|
2032
|
2,262,000 | 2,241,000 | ||||||
|
2033
|
1,854,000 | 1,825,000 | ||||||
|
2034
|
3,597,000 | 3,597,000 | ||||||
|
2035
|
4,600,000 | 4,600,000 | ||||||
| $ | 16,725,000 | $ | 16,661,000 | |||||
|
Research and development expenses, without time limitation
|
$ | 11,900,000 | $ | 13,003,000 | ||||
|
Other deductible temporary differences, without time limitation
|
$ | 2,687,000 | $ | 2,687,000 | ||||
17. Financial instruments:
This note provides disclosures relating to the nature and extent of the Corporation’s exposure to risks arising from financial instruments, including credit risk, foreign currency risk, interest rate risk and liquidity risk, and how the Corporation manages those risks.
|
(a)
|
Credit risk:
|
Credit risk is the risk of a loss if a customer or counterparty to a financial asset fails to meet its contractual obligations, and arises primarily from the Corporation’s trade receivables. The Corporation may also have credit risk relating to cash and short-term investments, which it manages by dealing only with highly-rated Canadian institutions. The carrying amount of financial assets, as disclosed in the statements of financial position, represents the Corporation’s credit exposure at the reporting date. The Corporation’s trade receivables and credit exposure fluctuate throughout the year. The Corporation’s average trade receivables and credit exposure during the year may be higher than the balance at the end of that reporting year.
The Corporation’s credit risk for trade receivables is concentrated, as the majority of its sales are to one customer. As at February 28, 2015, the Corporation has one trade debtor. Most sales' payment terms are set in accordance with industry practice. One customer represents 100% of total trade accounts included in trade and other receivables as at February 28, 2015 and February 28, 2014.
Most of the Corporation's customers are distributors for a given territory and are privately-held enterprises. The profile and credit quality of the Corporation’s retail customers vary significantly. Adverse changes in a customer’s financial position could cause the Corporation to limit or discontinue conducting business with that customer, require the Corporation to assume more credit risk relating to that customer’s future purchases or result in uncollectible accounts receivable from that customer. Such changes could have a material adverse effect on business, results of operations, financial condition and cash flows.
Customers do not provide collateral in exchange for credit, except in unusual circumstances. Receivables from selected customers are covered by credit insurance, with coverage amount usually of 100% of the invoicing, with the exception of some customers under specific terms. The information available through the insurers is the main element in the decision process to determine the credit limits assigned to customers.
120
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
17. Financial instruments (continued):
|
(a)
|
Credit risk (continued):
|
The Corporation’s extension of credit to customers involves considerable judgment and is based on an evaluation of each customer’s financial condition and payment history. The Corporation has established various internal controls designed to mitigate credit risk, including a credit analysis by the insurer which recommends customers' credit limits and payment terms that are reviewed and approved by the Corporation. The Corporation reviews periodically the insurer's maximum credit quotation for each of its clients. New clients are subject to the same process as regular clients. The Corporation has also established procedures to obtain approval by senior management to release goods for shipment when customers have fully-utilized approved insurers credit limits. From time to time, the Corporation will temporarily transact with customers on a prepayment basis where circumstances warrant. The Corporation’s credit controls and processes cannot eliminate credit risk.
The Corporation provides for trade receivables to their expected realizable value as soon as the account is determined not to be fully collectible, with such write-offs charged to earnings unless the loss has been provided for in prior years, in which case the write-off is applied to reduce the allowance for doubtful accounts. The Corporation updates its estimate of the allowance for doubtful accounts, based on evaluations of the collectability of trade receivable balances at each reporting date, taking into account amounts which are past due, and any available information indicating that a customer could be experiencing liquidity or going concern problems.
The aging of trade receivable balances and the allowance for doubtful accounts as at February 28, 2015 and 2014 were as follows:
|
2015
|
2014
|
|||||||
|
|
||||||||
|
Current
|
$ | – | $ | 196,010 | ||||
|
Past due 0-30 days
|
226,628 | – | ||||||
|
Past due 31-120 days
|
– | 24,006 | ||||||
|
Past due 121-180 days
|
89,325 | 177,682 | ||||||
|
Trade receivables
|
315,953 | 397,698 | ||||||
|
Less allowance for doubtful accounts
|
(65,640 | ) | (2,570 | ) | ||||
| $ | 250,313 | $ | 395,128 | |||||
The allowance for doubtful accounts is for customer accounts over 121 days past due.
During the year ended February 28, 2015, the Corporation recorded a bad debt expense of $63,070 (2014 - nil) related to one significant customer, for which total trade receivable due at February 28, 2015 is $315,953.
The movement in allowance for doubtful accounts in respect of trade receivables was as follows:
|
February 28,
|
February 28,
|
|||||||
|
2015
|
2014
|
|||||||
|
Balance, beginning of year
|
$ | 2,570 | $ | 2,570 | ||||
|
Bad debt expenses
|
66,161 | – | ||||||
|
Write-off against reserve
|
(3,091 | ) | – | |||||
|
Balance, end of year
|
$ | 65,640 | $ | 2,570 | ||||
121
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
17. Financial instruments (continued):
|
(b)
|
Currency risk:
|
The Corporation is exposed to the financial risk related to the fluctuation of foreign exchange rates and the degrees of volatility of those rates. Foreign currency risk is limited to the portion of the Corporation's business transactions denominated in currencies other than the Canadian dollar. Fluctuations related to foreign exchange rates could cause unforeseen fluctuations in the Corporation's operating results.
All of the Corporation’s revenues are in US dollars. A portion of the expenses, mainly related to research contracts, is made in US dollars. There is a financial risk involved related to the fluctuation in the value of the US dollar in relation to the Canadian dollar.
The following table provides an indication of the Corporation’s significant foreign exchange currency exposures as stated in Canadian dollars at the following dates:
|
|
February 28, 2015
|
28-Feb-14
|
||||||
|
US$
|
US$
|
|||||||
|
Cash
|
1,102,908 | 360,691 | ||||||
|
Short-term investments
|
15,007,176 | 15,504,707 | ||||||
|
Trade and other receivables
|
250,313 | 397,743 | ||||||
|
Trade and other payables
|
(398,648 | ) | (260,218 | ) | ||||
| 15,961,749 | 16,002,923 | |||||||
The following exchange rates are those applicable to the following periods and dates:
|
February 28,
|
February 28,
|
|||||||||||||||
|
2015
|
2014
|
|||||||||||||||
|
Average
|
Reporting
|
Average
|
Reporting
|
|||||||||||||
|
US$ per CAD
|
1.1266 | 1.2503 | 1.0466 | 1.1074 | ||||||||||||
Based on the Corporation’s foreign currency exposures noted above, varying the above foreign exchange rates to reflect a 5% strengthening of the US dollar would have increased the net profit as follows, assuming that all other variables remained constant:
|
February 28,
|
February 28,
|
|||||||
|
2015
|
2014
|
|||||||
|
US$
|
US$
|
|||||||
|
Increase in net profit
|
638,317 | 722,545 | ||||||
An assumed 5% weakening of the foreign currency would have had an equal but opposite effect on the basis that all other variables remained constant.
122
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
17. Financial instruments (continued):
|
|
(c)
|
Interest rate risk:
|
Interest rate risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market rates.
The Corporation’s exposure to interest rate risk as at February 28, 2015 and 2014 is as follows:
|
Cash
|
Short-term fixed interest rate
|
|
Short-term investments
|
Short-term fixed interest rate
|
The capacity of the Corporation to reinvest the short-term amounts with equivalent return will be impacted by variations in short-term fixed interest rates available on the market. Management believes that the risk that the Corporation will realize a loss as a result of the decline in the fair value of its short-term investments is limited because these investments have short-term maturities and are generally held to maturity.
|
|
(d)
|
Liquidity risk:
|
Liquidity risk is the risk that the Corporation will not be able to meet its financial obligations as they fall due. The Corporation manages liquidity risk through the management of its capital structure and financial leverage, as outlined in Note 20. It also manages liquidity risk by continuously monitoring actual and projected cash flows. The Board of Directors reviews and approves the Corporation's operating budgets, and reviews material transactions outside the normal course of business.
The following are the contractual maturities of financial liabilities as at February 28, 2015 and 2014:
|
February 28,
|
||||||||||||||||||||
|
2015
|
||||||||||||||||||||
|
Required payments per year
|
Carrying
|
Less than
|
1 to
|
More than
|
||||||||||||||||
|
(in thousands of dollars)
|
Total
|
amount
|
1 year
|
5 years
|
5 years
|
|||||||||||||||
|
Trade and other payables
|
$ | 1,084 | $ | 1,084 | $ | 1,084 | $ | – | $ | – | ||||||||||
|
Payable to parent corporation
|
538 | 538 | 538 | – | – | |||||||||||||||
| $ | 1,622 | $ | 1,622 | $ | 1,622 | $ | – | $ | – | |||||||||||
|
February 28,
|
||||||||||||||||||||
| 2014 | ||||||||||||||||||||
|
Required payments per year
|
Carrying
|
Less than
|
1 to
|
More than
|
||||||||||||||||
|
(in thousands of dollars)
|
Total
|
amount
|
1 year
|
5 years
|
5 years
|
|||||||||||||||
|
Trade and other payables
|
$ | 1,171 | $ | 1,171 | $ | 1,171 | $ | – | $ | – | ||||||||||
The Derivative warrant liabilities are excluded from the above tables as they will be settled in shares and not by the use of liquidities.
123
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
17. Financial instruments (continued):
|
|
(e)
|
Short-term investments
|
As at February 28, 2015, short-term investments consisting of term deposits are with a Canadian financial institution having a high credit rating. Short-term investments include two investments with maturity dates from June 30, 2015 to September 2, 2015, bearing an interest rate from 0.15% to 1.05% per annum, cashable at any time at the discretion of the Corporation, under certain conditions.
As at February 28, 2014, short-term investments consisting of term deposits are with a Canadian financial institution having a high credit rating. Short-term investments include four investments with maturity dates from May 8, 2014 to February 18, 2015, bearing an interest rate from 0.15% to 1.15% per annum, cashable at any time at the discretion of the Corporation, under certain conditions.
18. Commitments and contingencies:
License agreement:
The Corporation was initially committed under a license agreement to pay Neptune until the expiration of Neptune’s patents on licensed intellectual property, a royalty in relation to sales of products in the licensed field. In 2014, the Corporation exercised its option under the License Agreement to pay in advance all of the future royalties’ payable under the license by issuing 6,750,000 Class A shares, at a price of $2.30 per share to Neptune.
The value of the prepayment, determined with the assistance of outside valuations specialists, using the pre-established formula set forth in the license agreement (adjusted to reflect the royalties of $395,068 accrued from December 4, 2012, the date at which the Corporation entered into the prepayment agreement to July 12, 2013, the date of issuance of the shares) totalling $15,129,932, was recognized as an intangible asset. The shares issued as a result of this transaction corresponded to an increase in share capital of $15,525,000, net of $29,000 of share issue costs. The Corporation no longer has a royalty payment commitment under the License Agreement.
Research and development agreements:
In the normal course of business, the Corporation has signed agreements with various partners and suppliers for them to execute research projects and to produce and market certain products. The Corporation has reserved certain rights relating to these projects.
The Corporation initiated research and development projects that will be conducted over a 12 to 24 month period for a total cost of $10,562,442, of which an amount of $6,299,274 has been paid to date. As at February 28, 2015, an amount of $432,446 is included in ''Trade and other payables'' in relation to these projects.
Contingencies:
|
i.
|
On May 29, 2014, Neptune and its subsidiaries, including the Corporation, were served with a lawsuit from Mr. Henri Harland, former President and Chief Executive Officer of Neptune and its subsidiaries who resigned from all his duties on April 25, 2014. Mr. Harland alleges in his complaint that he was forced to resign and is claiming inter alia, the acknowledgment of the relevant sections of his employment contract, the payment of a sum of approximately $8,500,000 and the issuance of 500,000 shares of each Neptune, Acasti and NeuroBioPharm, as well as two blocks of 1,000,000 call-options each on the shares held by Neptune in Acasti and NeuroBioPharm in his name. Neptune and its subsidiaries believe the claim as formulated is without merit or cause. On December 11, 2014 Neptune, Acasti and NeuroBioPharm filed their defence and counterclaim alleging inter alia that Mr. Harland’s contract is null and void and that he is owed nothing following his resignation. Should the Court determine that the contract is nonetheless valid, Neptune and its subsidiaries’ position, as stated in the defence and counterclaim, is that there was also enough evidence discovered after Mr. Harland’s resignation that would have justified a dismissal for cause and that again, nothing is owed to the plaintiff. No trial date has been set. All outstanding share-based payments held by Mr. Harland have been cancelled during the year ended February 28, 2015. As of the date of these financial statements, no agreement has been reached and no provision has been recognized in respect of this claim. Neptune and its subsidiaries also filed an additional claim to recover certain amounts from Mr. Harland.
|
|
ii.
|
In the normal course of operations, the Corporation is involved in various claims and legal proceedings. Although the outcome of these pending cases as at February 28, 2015 cannot be determined with certainty, based on currently available information, management believes that the ultimate outcome of these matters, individually and in aggregate, will not have a material adverse effect on the Corporation’s financial position or overall trends in results of operations.
|
124
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
19. Determination of fair values:
Certain of the Corporation’s accounting policies and disclosures require the determination of fair value, for both financial and non-financial assets and liabilities. Fair values have been determined for measurement and/or disclosure purposes based on the following methods.
Financial and non-financial assets and liabilities:
In establishing fair value, the Corporation uses a fair value hierarchy based on levels as defined below:
|
·
|
Level 1: defined as observable inputs such as quoted prices in active markets.
|
|
·
|
Level 2: defined as inputs other than quoted prices in active markets that are either directly or indirectly observable.
|
|
·
|
Level 3: defined as inputs that are based on little or no little observable market data, therefore requiring entities to develop their own assumptions.
|
The Corporation has determined that the carrying values of its short-term financial assets and liabilities approximate their fair value given the short-term nature of these instruments.
Derivative warrant liabilities:
The Corporation measured its derivative warrant liabilities at fair value on a recurring basis. These financial liabilities were measured using level 3 inputs. The inputs used in the determination of the fair values of the warrant liabilities are disclosed in note 11(b).
The effect of an increase or a decrease of 5% of the volatility used, which is the significant unobservable input in the fair value estimate, would result in a loss of $414,116 or a gain of $406,485 respectively.
The reconciliation of changes in level 3 fair value measurements of financial liabilities for the year ended February 28, 2015 and 2014 is presented in the following table:
|
2015
|
2014
|
|||||||
|
Balance – beginning of year
|
$ | 11,181,475 | $ | – | ||||
|
Recognition of derivative warrant liabilities
|
– | 10,674,045 | ||||||
|
Change in fair value of derivative warrant liabilities (Note 11 (b))
|
(8,824,067 | ) | 507,430 | |||||
|
Closing balance
|
2,357,408 | $ | 11,181,475 | |||||
Share-based payment transactions:
The fair value of share-based payment transaction is measured based on the Black-Scholes valuation model. Measurement inputs include share price on measurement date, exercise price of the instrument, expected volatility (based on weighted average historic volatility), weighted average expected life of the instruments (based on historical experience and general option holder behaviour), expected dividends, and the risk-free interest rate (based on government bonds). Service and non-market performance conditions attached to the transactions, if any, are not taken into account in determining fair value.
20. Capital management:
Since inception, the Corporation’s objective in managing capital is to ensure sufficient liquidity to finance its research and development activities, general and administrative expenses, expenses associated with intellectual property protection and its overall capital expenditures. The Corporation is not exposed to external requirements by regulatory agencies or third parties regarding its capital.
Since the beginning of its operations, the Corporation has financed its liquidity needs from funding provided by a public offering, a private placement, its parent corporation, from the exercise of warrants that were distributed to its parent corporation’s shareholders, from a rights offering and from the issuance of options to employees. The Corporation attempts to optimize its liquidity needs with non-dilutive sources whenever possible, including from research and development tax credits.
The Corporation defines capital to include total shareholders’ equity and derivative warrant liabilities.
The Corporation’s policy is to maintain a minimal level of debt.
125
ACASTI PHARMA INC.
Notes to Financial Statements, Continued
Years ended February 28, 2015, 2014 and 2013
20. Capital management (continued):
As of February 28, 2015, cash amounted to $1,310,556, short-term investments amounted to $17,071,344 and tax credits receivable amounted to $419,992, for a total of $18,801,892.
21. Operating segments:
The Corporation has one reportable operating segment: the development and commercialization of pharmaceutical applications of its licensed rights for cardiovascular diseases.
The majority of the Corporation’s assets are located in Canada.
The Corporation’s sales are attributed based on the customer’s area of residence. All of the sales during the years ended February 28, 2015 and 2014 were made to the United States. All of the sales during the year ended February 28, 2013, except for the sale made to Neptune in the amount of $41,000, were made to the United States.
During the year ended February 28, 2015, the Corporation realized sales amounting to $224,324 (2014: $473,180 and 2013: $640,975) from one customer accounting for 83% (2014: 94% and 2013: 89%) of sales.
22. Subsequent event:
On April 29, 2015, the Corporation announced the departure of Mr. André Godin as Chief Financial Officer of Acasti.
126
|
Item 18.
|
Financial Statements
|
See Item 17.
|
Item 19.
|
Exhibits
|
EXHIBITS INDEX
|
Exhibit
Number
|
Description of Document
|
|
|
1.1
|
Articles of Incorporation (incorporated by reference to Exhibit 4.1 from Form S-8 (File No. 333-191383) filed with the Commission on September 25, 2013)
|
|
|
1.2
|
Bylaw No. 1 (incorporated by reference to Exhibit 4.2 from Form S-8 (File No. 333-191383) filed with the Commission on September 25, 2013)
|
|
|
1.3
|
Bylaw No. 2013-1 (incorporated by reference to Exhibit 4.3 from Form S-8 (File No. 333-191383) filed with the Commission on September 25, 2013)
|
|
|
2.1
|
Specimen Certificate for Common Shares of Acasti Pharma Inc. (incorporated by reference to Exhibit 2.1 from Form 20-F (File No. 001-35776) filed with the Commission on June 6, 2014)
|
|
|
2.2
|
Warrant Indenture dated December 3, 2013 between Acasti Pharma Inc. and Computershare Trust Company of Canada (incorporated by reference to Exhibit 99.1 from Form 6-K (File No. 001-35776) filed with the Commission on December 3, 2013)
|
|
|
4.1
|
Prepayment Agreement, dated December 4, 2012, between Neptune Technologies & Bioressources Inc. and Acasti Pharma Inc. (incorporated by reference to Exhibit 99.1 from Form 6-K (File No. 001-35776) filed with the Commission on October 29, 2013)
|
|
|
4.2
|
Equity Incentive Plan (incorporated by reference to Exhibit 4.4 from Form S-8 (File No. 333-191383) filed with the Commission on September 25, 2013)
|
|
|
4.3
|
Stock Option Plan (incorporated by reference to Exhibit 4.5 from Form S-8 (File No. 333-191383) filed with the Commission on September 25, 2013)
|
|
|
11.1
|
Code of Business Conduct and Ethics for Directors, Officers and Employees (incorporated by reference to Exhibit 99.4 from Form 40-F (File No. 001-35776) filed with the Commission on May 30, 2013)
|
|
|
12.1*
|
Principal Executive Officer Certification Pursuant to Section 302 of the Sarbanes-Oxley Act of 2002
|
|
|
12.2*
|
Principal Financial Officer Certification Pursuant to Section 302 of the Sarbanes-Oxley Act of 2002
|
|
|
13.1*
|
Principal Executive Officer Certification Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002
|
|
|
13.2*
|
Principal Financial Officer Certification Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002
|
|
*
|
- filed herewith
|
127
The registrant hereby certifies that it meets all of the requirements for filing on this Annual Report and that it has duly caused and authorized the undersigned to sign this Annual Report on its behalf.
|
ACASTI PHARMA INC.
|
||
|
By:
|
/s/ Jim Hamilton__________________________ | |
|
Name:
|
Jim Hamilton
|
|
|
Title:
|
Person acting in the capacity of
Principal Executive Officer
|
|
Date: June 16, 2015
128