10-K: Annual report pursuant to Section 13 and 15(d)
Published on June 21, 2022
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM
(Mark One)
For the fiscal year ended
or
For the transition period from |
|
to |
|
Commission file number:
(Exact name of registrant as specified in its charter)
Québec, |
|
|
(State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification Number) |
(Address of principal executive offices, including zip code)
Registrant’s telephone number, including area code:
Securities registered pursuant to Section 12(b) of the Act:
Title of each class |
|
Name of each exchange on which registered |
|
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ☐
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days.
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files).
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
Large accelerated filer |
☐ |
Accelerated filer |
☐ |
|
|
|
|
☒ |
Smaller reporting company |
||
|
|
|
|
|
|
Emerging growth company |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report.
The aggregate market value of the voting and non-voting common shares held by non-affiliates of the registrant, based on the closing sale price of the registrant’s common shares on the last business day of its most recently completed second fiscal quarter, as reported on the NASDAQ Stock Market, was approximately $110,720,458.
The number of outstanding common shares of the registrant, no par value per share, as of June 21, 2022, was
Auditor Firm Id:
Documents Incorporated by Reference
Portions of the registrant’s Definitive Proxy Statement to be filed with the Securities and Exchange Commission pursuant to Regulation 14A in connection with the registrant’s 2022 Annual Meeting of Shareholders, to be filed subsequent to the date hereof, are incorporated by reference into Part III of this annual report. Such Definitive Proxy Statement will be filed with the Securities and Exchange Commission not later than 120 days after the conclusion of the registrant’s fiscal year ended March 31, 2022.
ACASTI PHARMA INC.
FORM 10-K
For the Fiscal Year Ended March 31, 2022
Table of Contents
|
|
|
|
|
Item 1. |
8 |
|
|
Item 1A. |
19 |
|
|
Item 1B. |
39 |
|
|
Item 2. |
39 |
|
|
Item 3. |
39 |
|
|
Item 4. |
39 |
|
|
|
|
|
|
Item 5. |
40 |
|
|
Item 6. |
43 |
|
|
Item 7. |
Management’s Discussion and Analysis of Financial Condition and Results of Operation |
44 |
|
Item 7A. |
54 |
|
|
Item 8. |
54 |
|
|
Item 9. |
Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
54 |
|
Item 9A. |
54 |
|
|
Item 9B. |
54 |
|
|
Item 9C. |
Disclosure Regarding Foreign Jurisdictions that Prevent Inspections |
|
|
|
|
|
|
Item 10. |
55 |
|
|
Item 11. |
55 |
|
|
Item 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Shareholder Matters |
55 |
|
Item 13. |
Certain Relationships and Related Transactions and Director Independence |
55 |
|
Item 14. |
55 |
|
|
|
|
|
|
Item 15. |
56 |
|
|
Item 16. |
56 |
|
|
|
||
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This annual report contains information that may be forward-looking information within the meaning of Canadian securities laws and forward-looking statements within the meaning of U.S. federal securities laws, both of which we refer to in this annual report as forward-looking information. Forward- looking information can be identified by the use of terms such as “may”, “will”, “should”, “expect”, “plan”, “anticipate”, “believe”, “intend”, “estimate”, “predict”, “potential”, “continue” or other similar expressions concerning matters that are not statements about the present or historical facts. Forward-looking information in this annual report includes, among other things, information or statements about:
Although the forward-looking statements in this annual report are based upon what we believe are reasonable assumptions, you should not place undue reliance on those forward-looking statements since actual results may vary materially from them. Important assumptions made by us when making forward-looking statements include, among other things, assumptions by us that:
In addition, the forward-looking statements in this annual report are subject to a number of known and unknown risks, uncertainties and other factors many of which are beyond our control, that could cause our actual results and developments to differ materially from those that are disclosed in or implied by the forward-looking statements, including, among others:
All of the forward-looking statements in this annual report are qualified by this cautionary statement. There can be no guarantee that the results or developments that we anticipate will be realized or, even if substantially realized, that they will have the consequences or effects on our business, financial condition, or results of operations that we anticipate. As a result, you should not place undue reliance on the forward-looking statements. Except as required by applicable law, we do not undertake to update or amend any forward-looking statements, whether as a result of new information, future events or otherwise. All forward-looking statements are made as of the date of this annual report.
We express all amounts in this annual report in U.S. dollars, except where otherwise indicated. References to “$” and “U.S.$” are to U.S. dollars and references to “C$” or “CAD$” are to Canadian dollars.
Except as otherwise indicated, references in this annual report to “Acasti,” “the Corporation,” “we,” “us” and “our” refer to Acasti Pharma Inc. and its consolidated subsidiaries, including Acasti Pharma U.S., which is formerly Grace.
PART I
Item 1. Business
Overview
On August 27, 2021, we completed our acquisition of Grace via a merger following the approval of Acasti’s shareholders and Grace’s stockholders. Following completion of the merger, Grace became a wholly owned subsidiary of Acasti and was renamed Acasti Pharma U.S. Inc.
The successful completion of the merger positions Acasti to build a premier, late-stage specialty pharmaceutical company focused on developing and commercializing products for rare and orphan diseases that have the potential to improve clinical outcomes by using the Company’s novel drug delivery technologies. We seek to apply new proprietary formulations to approved and marketed pharmaceutical compounds to achieve enhanced efficacy, faster onset of action, reduced side effects, and more convenient drug delivery and increased patient compliance; all of which could result in improved patient outcomes. The active ingredients chosen by Acasti for further development may be already approved in a target indication or could be repurposed for use in new indications.
The existing well understood efficacy and safety profiles of these marketed compounds provides the opportunity for us to utilize the Section 505(b)(2) regulatory pathway under the Federal Food, Drug and Cosmetic Act (the “FFDCA”) for our reformulated versions of these drugs, and therefore may provide a potentially shorter path to regulatory approval. Under Section 505(b)(2), if sufficient support of a product’s safety and efficacy either through previous FDA experience or sufficiently within the scientific literature can be established, it may eliminate the need to conduct some of the early studies that new drug candidates might otherwise require.
In connection with the merger, we acquired Grace’s entire therapeutic pipeline, which has the potential to address critical unmet medical needs for the treatment of rare and orphan diseases. The pipeline consists of three unique clinical stage and multiple pre-clinical stage assets supported by an intellectual property portfolio of more than 40 granted and pending patents in various jurisdictions worldwide. These drug candidates aim to improve clinical outcomes by applying proprietary formulation and drug delivery technologies to existing pharmaceutical compounds to achieve improvements over the current standard of care, or to provide treatment for diseases with no currently approved therapies.
Rare disorders represent an attractive area for drug development, and there remains an opportunity for Acasti to utilize already approved drugs that have established safety profiles and clinical experience to potentially address significant unmet medical needs. A key advantage of pursuing therapies for rare disorders is the potential to receive orphan drug designation (“ODD”) from the FDA. ODD provides for seven years of marketing exclusivity in the United States post-launch, provided certain conditions are met. Rare diseases also allow for more manageably scaled clinical trials and provide market opportunities that may require a smaller, more targeted commercial infrastructure.
The specific diseases targeted for drug development by Acasti are well understood although these patient populations may remain poorly served by available therapies or in some cases approved therapies do not yet exist. We aim to effectively treat debilitating symptoms that result from these underlying diseases.
Our three most advanced programs are:
Our management team possesses significant experience in drug delivery research and evaluation, clinical and pharmaceutical development and manufacturing, regulatory affairs, and business development, as well as being well-versed in late-stage drug development and commercialization. The Acasti team has been collectively involved in the development and approval of several successful marketed drugs, including TORADOL, NAPROSYN, ANDROGEL, SUBSYS, MARINOL and KEPPRA XR, Claritin®, Euflex®, Effexor®, Sonata®, Ativan®, RD-Heparin®, Rapamune®, Etodolac Aricept®, Cardizem®, Deflazacort®, Macimorelin®
8
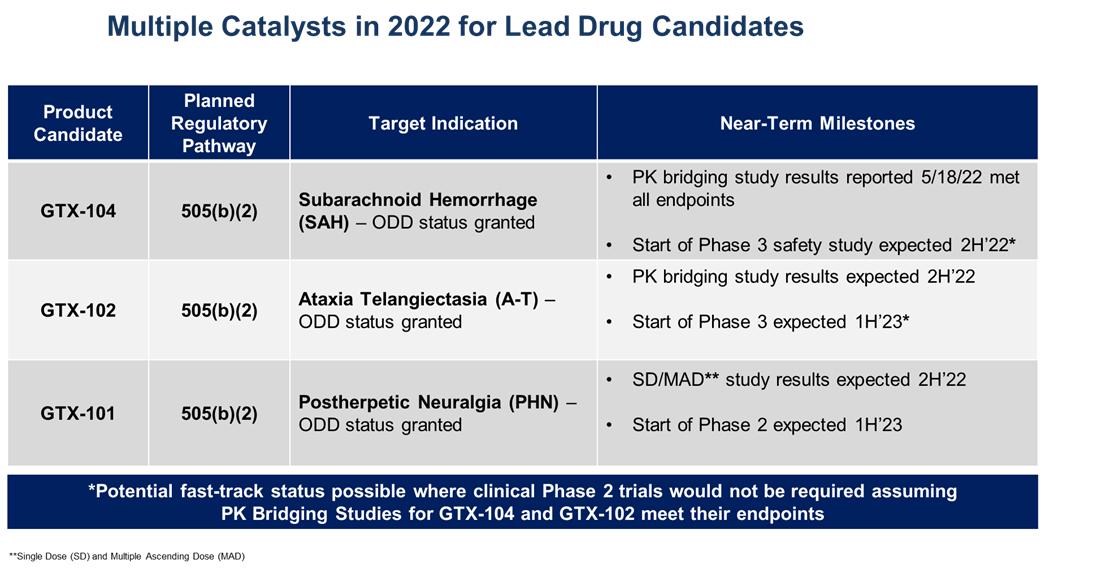
The table below summarizes planned key 2022 calendar year milestones for our three clinical drug candidates:
GTX-104 Overview
Nimodipine was granted FDA approval in 1988, and is the only drug approved to improve neurological outcomes in SAH. It is only available in the United States as a generic oral capsule and as a branded oral liquid solution called NYMALIZE, which is manufactured and sold by Arbor Pharmaceuticals. Nimodipine has poor water solubility and high permeability characteristics as a result of its high lipophilicity. Additionally, orally administered nimodipine has dose-limiting side-effects such as hypotension, poor absorption and low bioavailability resulting from high first-pass metabolism, and a narrow administration window as food effects lower bioavailability significantly. Due to these issues, blood levels of orally administered nimodipine can be highly variable, making it difficult to manage blood pressure in SAH patients. Nimodipine capsules are also difficult to administer, particularly to unconscious patients or those with impaired ability to swallow. Concomitant use with CYP3A inhibitors is contraindicated (NIMODIPINE Capsule PI).
NIMOTOP is an injectable form of nimodipine that is manufactured by Bayer Healthcare. It is approved in Europe and in other regulated markets (but not in the United States), but it has limited utility for SAH patients because of its high organic solvent content, namely 23.7% ethanol and 17% polyethylene glycol 400 (NIMOTOP SmPC).
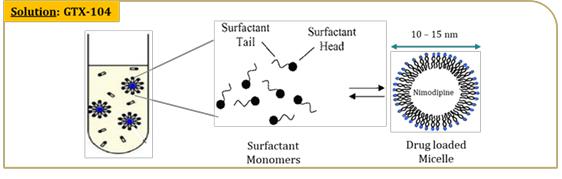
GTX-104 is a clinical stage, novel formulation of nimodipine for IV infusion in SAH patients. It uses surfactant micelles as the drug carrier to solubilize nimodipine. This unique nimodipine injectable formulation is composed of a nimodipine base, an effective amount of polysorbate 80, a non-ionic hydrophilic surfactant, and a pharmaceutically acceptable carrier for injection. GTX-104 is an aqueous solution substantially free of organic solvents, such that the nimodipine is contained in a concentrated injection solution, suspension, emulsion or complex as a micelle, a colloidal particle or an inclusion complex, and the formulation is stable and clear.
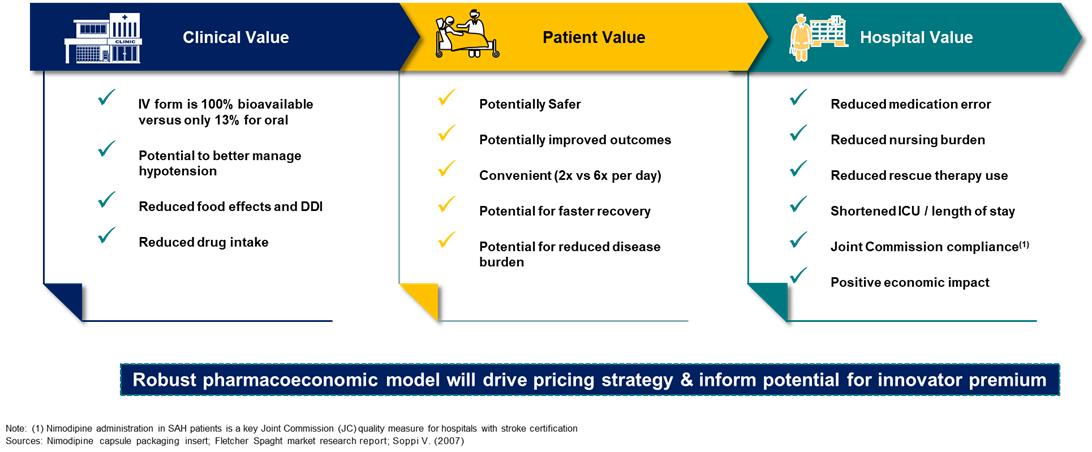
Key Benefits: Novel nanoparticle technology facilitates aqueous formulation of insoluble nimodipine and enables a safe, standard peripheral IV infusion:
9
GTX-104 could provide a more convenient mode of administration as compared to generic nimodipine capsules or NYMALIZE GTX-104 is peripherally infused every four hours as compared to administration via a nasogastric tube in unconscious patients every two to four hours for both NYMALIZE oral solution and nimodipine oral capsules. Therefore, GTX-104 could be considered as a major contribution to patient care by potentially reducing the dosing frequency, and the associated nursing burden. More convenient and less frequent dosing can also reduce the risk of medication errors. In addition, two PK studies conducted with GTX-104 has shown that it has the potential to provide improved bioavailability and lower intra-subject variability compared to oral administration. Because of its IV formulation, we also expect it to reduce certain drug-drug interactions and food effects.
Despite the positive impact it has on recovery, physicians often must discontinue their patients on oral nimodipine, primarily as a result of hypotensive episodes that cannot be controlled by titrating the oral form of drug. Such discontinuation could potentially be avoided by administering GTX-104, which because of its IV administration, may obviate the complexity that results from the need for careful attention to the timing of nimodipine administration at least one hour before or two hours after a meal. Administration of GTX-104 via a peripheral vein is often much more comfortable for the patients compared to administration by central venous access, which can often be a difficult and invasive procedure. Also, unconscious patients will likely receive more consistent concentrations of nimodipine when delivered by the IV route as compared to oral gavage or a nasogastric tube. More consistent dosing is expected to result in a reduction of vasospasm and a better, more consistent management of hypotension. As summarized in the table below, we anticipate reduced use of rescue therapies, such as vasopressors, and expensive hospital resources, such as the angiography suite, are possible by more effectively managing blood pressure with GTX-104. Reduced incidences of vasospasm could result in shorter length of stay and better outcomes.
About Subarachnoid Hemorrhage (SAH)
SAH is bleeding over the surface of the brain in the subarachnoid space between the brain and the skull, which contains blood vessels that supply the brain. A primary cause of such bleeding is rupture of an aneurysm. The result is a relatively uncommon type of stroke that accounts for about 5% of all strokes and has an incidence of six per 100,000 person years (Becske, 2018).
In contrast to more common types of stroke in elderly individuals, an SAH often occurs at a relatively young age, with approximately half the affected patients younger than 60 years old (Becske, 2018). Particularly devastating for patients younger than 45, around 10% to 15% of aneurysmal SAH (“aSAH”) patients die before reaching the hospital (Rinkel, 2016), and those who survive the initial hours post hemorrhage are admitted or transferred to tertiary care centers with high risk of complications, including rebleeding and delayed cerebral ischemia (“DCI”). Systemic manifestations affecting cardiovascular, pulmonary, and renal function are common and often complicate management of DCI. Approximately 70% of aSAH patients experience death or a permanent dependence on family members, and half die within one month after the hemorrhage. Of those who survive the initial month, half remain permanently dependent on a caregiver to maintain daily living (Becske, 2018).
Treatment offerings currently include sustained hypervolemia, hemodilution, and/or induced hypertension (Triple-H therapy), calcium antagonists and angioplasty. Because vasospasm may result from an increase of calcium in the vascular smooth-muscle cell, a medical rationale has emerged for the use of calcium antagonists. The addition of calcium antagonists like nimodipine to the treatment arsenal for the prevention of cerebral vasospasm after aSAH is based on the notion that these drugs can counteract the influx of calcium into the vascular smooth-muscle cell (Rinkel, 2002).
10
The incidence of SAH in the United States is approximately 10 in every 100,000 persons per year (Becske, 2016; NINDS, 2016; Ingall, 1989; Schievink, 1995; Schievink, 1997; Zacharia, 2010), based on multiple analyses of the population of Rochester, Minnesota. Ingall (1989) studied the incidence of SAH in this population over the 40-year period from 1945 through 1984. At that time, the population of Rochester lent itself well to epidemiological studies because medical care was provided primarily by the Mayo Clinic. Over this period, the average annual incidence rate of aSAH remained constant at approximately 11 per 100,000 population. More recently, the American Heart Association/American Stroke Association Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage (Connolly, 2012) refer to the 2003 Nationwide Inpatient Sample as providing an annual estimate of 14.5 discharges for aSAH per 100,000 adults, although, because death resulting from aSAH often occurs before hospital admission (in an estimated 10% to 15% of cases), the true incidence may be higher. According to the U.S. Census Bureau, Population Estimates for 2015, the U.S. population was estimated at 321,418,820. Therefore, we estimate that approximately 53,596 individuals experience aSAH each year. The total addressable market for SAH is approximately $300 million in the U.S., and an estimated 50,000 patients in the European Union based on annual inpatient admissions and the average length-of-stay.
GTX-104—R&D History and Clinical Studies to Date
During 2017 and 2018, Acasti Pharma U.S. (formerly Grace) evaluated GTX-104 in a four-part, single center, randomized, safety and dose-escalation and crossover study in over 80 healthy male and female subjects designed to assess the PK, bioavailability (“BA”), and the safety of GTX-104 administered via IV infusion compared to nimodipine oral capsules.
Details of the four-part PK study follow below:
Part One: |
|
|
|
|
|
|
|
|
Primary Objective: |
|
Evaluate the preliminary cardiovascular safety and tolerability of incremental doses of IV GTX-104 in healthy male and female subjects |
|
|
|
Method: |
|
Evaluate incremental dose-escalation of GTX-104 administered at dose levels of 0.3 mg/h to 1.22 mg/h over 16 hours, with dose-escalation occurring every 4 hours (0.3, 0.6, 0.9, and 1.22 mg/h) |
|
|
|
Adverse Events: |
|
Arthralgia, constipation, flatulence, headache, infusion site irritation, peripheral edema, and vomiting—all adverse events (“AEs”) were rated as mild in severity |
Part Two: |
|
|
|
|
|
|
|
|
Primary Objective: |
|
Evaluate the PK and BA of GTX-104 administered via IV infusion compared to the reference product of oral nimodipine capsules and to select the dose of IV GTX-104 with an exposure profile most closely matching that of oral nimodipine capsules |
|
|
|
Method: |
|
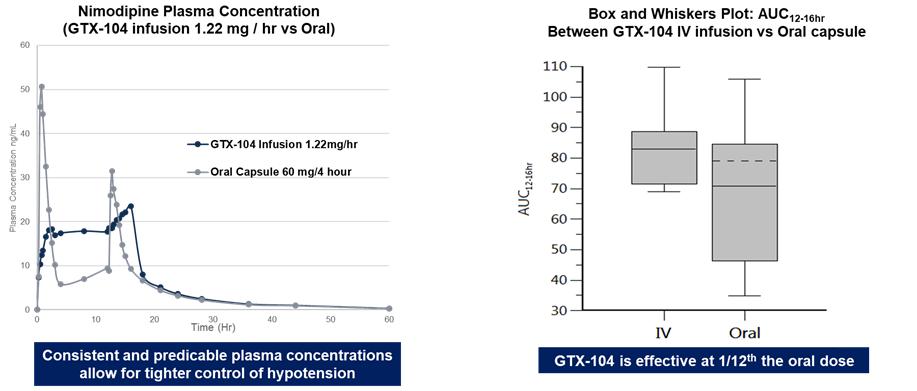
Two-period, crossover BA study. Pilot study that evaluated GTX-104 administered open-label as 1.22 mg/h continuous IV infusion for 16 hours compared to oral nimodipine (60 mg every 4 hours for 12 hours) in 12 subjects |
|
|
|
Adverse Events: |
|
No serious adverse events ("SAEs") in any subjects. 20.0% of subjects reported non-serious AEs following administration of GTX-104 compared to 50.0% of subjects reporting AEs following administration of oral nimodipine |
Part Three: |
|
|
|
|
|
|
|
|
Primary Objective: |
|
Determine the comparative bioavailability of IV GTX-104 versus oral nimodipine capsules and to evaluate the safety and tolerability of IV GTX 104 compared to oral nimodipine capsules in healthy male and female subjects |
|
|
|
Method: |
|
BA study, with GTX-104 administered as 1.1 mg/h continuous IV infusion for 28 hours compared to oral nimodipine capsules administered every four hours for 24 hours at a dose level of 60 mg in approximately 32 subjects |
|
|
|
Adverse Events: |
|
No SAEs; 20.0% of the subjects reported non-serious AEs following administration of GTX-104 whereas 8 (50.0%) subjects reported AEs following administration of oral nimodipine. Fourteen (34.1%) subjects reported AEs following administration of GTX-104 whereas 18 (43.9%) subjects reported AEs following administration of oral nimodipine |
Part Four: |
|
|
|
|
|
|
|
|
Primary Objective: |
|
Determine the comparative BA of IV GTX-104 versus oral nimodipine capsules and to evaluate the safety and tolerability of IV GTX 104 compared to oral nimodipine capsules in healthy male and female subjects |
|
|
|
Method: |
|
BA study: extension study with the same study design as Part Three, where only GTX-104 was administered open-label as a continuous IV infusion of 1.4 mg/h for 36 hours with oral nimodipine administered for 20 hours (approximately 24 subjects) |
|
|
|
Adverse Events: |
|
No SAEs: 10 (41.7%) subjects reported AEs following administration of GTX-104 whereas eight (36.4%) subjects reported AEs following administration of oral nimodipine |
11
GTX-104 Near Term Milestones: - Conduct PK Bridging and Phase 3 Safety Studies
In September 2021, we initiated our pivotal PK bridging study to evaluate the relative bioavailability of GTX-104 compared to currently marketed oral nimodipine capsules in approximately 50 healthy subjects. The PK study was the next required step in our proposed 505(b)(2) regulatory pathway for GTX-104.
Interim results were reported on December 2, 2021, and we believed at the time and it turned out to be correct, that the tight correlation of the primary endpoint data for the first 20 patients was a strong indication that GTX-104 could achieve comparable bioavailability with oral nimodipine in the full study cohort of 50 subjects. As observed in a previous PK study, the inter- and intra-subject variability in the interim analysis was much lower for GTX-104 as compared with oral nimodipine. There were no serious adverse events observed in the first 20 subjects, and only mild adverse events were reported in both groups such as headaches, that were resolved with common medications.
Final results from this pivotal PK study were reported on May 18, 2022, and showed that the bioavailability of IV GTX-104 compared favorably with the oral formulation of nimodipine in all subjects, and no serious adverse events were observed for GTX-104.
The PK study was completed at a single center in Canada and followed a 2-period crossover design where each subject received IV GTX-104 first, followed by oral nimodipine; or oral nimodipine first, followed by IV GTX-104. Fifty-eight subjects were randomized in a ratio of 1:1 between IV GTX-104 first or oral nimodipine first. IV GTX-104 and oral nimodipine was administered to all subjects over a period of 72 hours. A total of 56 and 55 subjects were included in the PK analysis at Day 1 and Day 3, respectively, as two subjects did not complete one of the two periods and one subject was excluded due to a protocol deviation, as prospectively defined in the statistical analysis plan.
The primary PK endpoints were maximum concentration (expressed as Cmax) during the first 4 hours on Day 1 and the total amount of nimodipine in the blood (expressed as the area under the curve (AUCDay 3, 0-24hr)) on Day 3. The secondary endpoint was Cmax measured over 24 hours on Day 3. The ratio of IV/oral is presented below for each endpoint with the corresponding 90% confidence interval (CI). A ratio of 1 indicates no absolute difference between IV GTX-104 and oral nimodipine.
The IV/oral ratio (%) and its corresponding 90% CI (range) for the primary and secondary endpoints in the subjects who completed each treatment period were as follows:
Day 1 Cmax, 0-4hr: 92% (82 – 104)
AUCDay 3, 0-24hr: 106% (99 – 114)
Day 3 Cmax, 0-24hr: 92% (85 – 101)
All three endpoints indicated that statistically there was no difference in exposures between IV GTX-104 and oral nimodipine over the defined time periods for both maximum exposure and total exposure. Plasma concentrations obtained following IV administration showed significantly less variability between subjects as compared to oral administration of capsules, since IV administration is not as sensitive to some of the physiological processes that affect oral administration, such as taking the drug with and without meals, variable gastrointestinal transit time, variable drug uptake from the gastrointestinal tract into the systemic circulation, and variable hepatic blood flow and hepatic first pass metabolism. Previous studies have shown these processes significantly affect the oral bioavailability of nimodipine, and therefore cause oral administration to be prone to larger within and between-subject variability.
The bioavailability of oral nimodipine capsules observed was only 8% compared to IV GTX-104. Consequently, less than one-tenth the amount of nimodipine is delivered with GTX-104 to achieve the same blood levels as with the oral capsules. In addition, the diurnal variation associated with IV GTX-104 was approximately half of that seen with the oral nimodipine capsules. Diurnal variation takes into consideration variation in body functions (blood flow, renal function and hepatic metabolism) over the course of a day.
No serious adverse events and no adverse events leading to withdrawal were reported during the study. More gastro-intestinal disorders were observed with oral nimodipine (16% vs 7% for IV GTX-104), and as expected in the context of a phase I trial conducted in healthy volunteers, more administration and sampling site related events were observed with IV GTX-104 (41% vs 11% for oral nimodipine). The other most frequently observed adverse events (IV/oral) were headache (36%/36%), somnolence (9%/13%) and hot flashes/flushing (10%/11%).
We plan to submit these results to the FDA, along with our proposed study design for the Phase 3 safety study which continues on track to start in the second half of 2022. We expect the safety study to be the final step required to seek approval under the 505(b)(2) regulatory pathway before submitting a New Drug Application to the FDA.
12
GTX-102 Overview
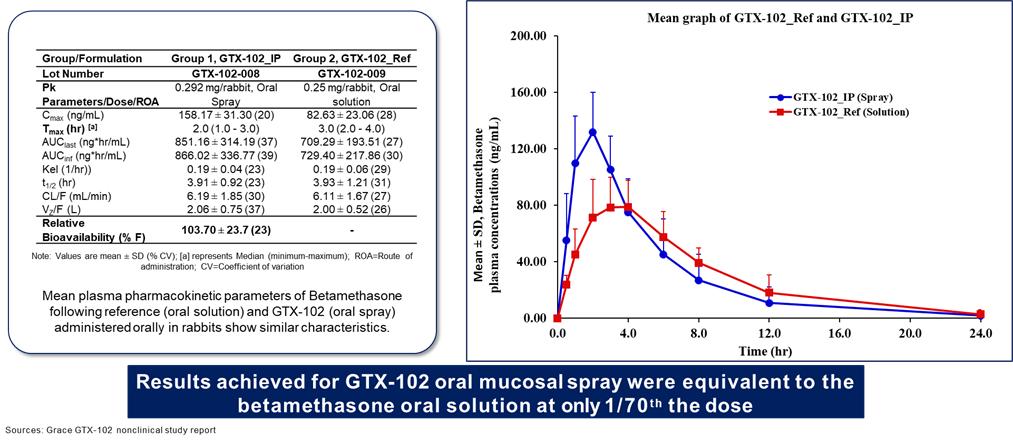
GTX-102 is a novel, concentrated oral-mucosal spray of betamethasone intended to improve neurological symptoms of Ataxia Telangiectasia (“A-T”) for which there are currently no FDA-approved therapies. GTX-102 is a stable, concentrated oral spray formulation comprised of the glucocorticoid betamethasone, that together with other excipients can be sprayed conveniently over the tongue of the A-T patient.
About Ataxia Telangiectasia
A-T is a rare genetic progressive autosomal recessive neurodegenerative disorder that affects children, with the hallmark symptoms of cerebellar ataxia and other motor dysfunction, and dilated blood vessels (telangiectasia) that occur in the sclera of the eyes. A-T is caused by mutations in the ataxia telangiectasia gene, which is responsible for modulating cellular response to stress, including breaks in the double strands of DNA.
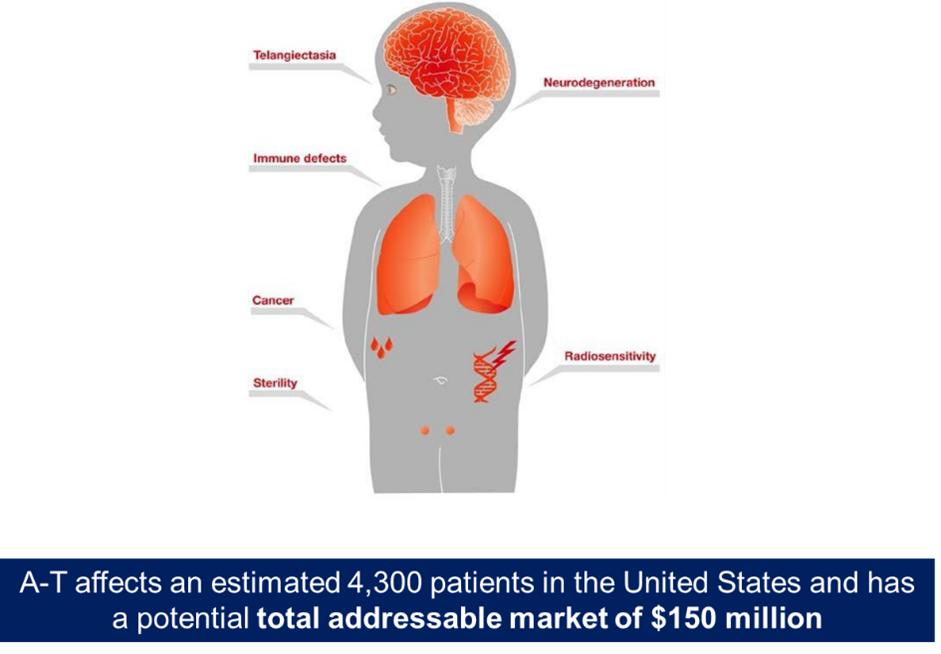
Children with A-T begin to experience balance and coordination problems when they begin to walk (toddler age), and ultimately become wheelchair-bound in their second decade of life. In pre-adolescence (between ages 5 and 8), patients experience oculomotor apraxia, dysarthria, and dysphagia. They also often develop compromised immune systems and are at increased risk of developing respiratory tract infections and cancer (typically lymphomas and leukemia) (U.S. National Cancer Institute A-T, 2015).
A-T is diagnosed through a combination of clinical assessment (especially neurologic and oculomotor deficits), laboratory analysis, and genetic testing. There is no known treatment to slow disease progression, and treatments that are used are strictly aimed at controlling the symptoms (e.g., physical, occupational or speech therapy for neurologic issues), or conditions secondary to the disease (e.g., antibiotics for lung infections, chemotherapy for cancer, etc.) (U.S. National Cancer Institute A-T, 2015). There are no FDA-approved therapeutic options currently available. Patients typically die by age 25 from complications of lung disease or cancer. According to a third-party report commissioned by Acasti Pharma US, A-T affects approximately 4,300 patients per year in the United States and has a potential total addressable market of $150 million, based on the number of treatable patients in the United States.
The U.S. National Institutes of Health (NIH) Genetics Home Reference, the U.S. National Organization for Rare Disorders (NORD), the U.S. National Cancer Institute, and the United States National Ataxia Foundation, all estimate the incidence of A-T worldwide to be between 1:40,000 and 1:100,000 live births. It has been reported in all races throughout the world and is represented equally in males and females (Lavin, 2007; Sedgwick and Boder, 1972).
For the purposes of estimating prevalence, the maximum survival age observed by Crawford et al., 40 years, has been used. Assuming a maximum survival of 40 years, the total number of A-T cases has been calculated from 1975 to 2015. The highest incidence rate reported in the United States of 1:40,000 has been used to obtain an estimate of A-T prevalence today. Between 1975 and 2015, the highest number of births in one year was 4,316,233 in 2007 (Martin, 2010; Martin, 2015) and so for the purposes of this prevalence calculation, this has been taken as the number of births per year.
Total A-T cases/year = 25 A-T births/million live births x 4.32 million live births/year = 108 new A-T cases/year. Assuming that all 108 people possibly born with A-T are still alive today, the total number of individuals with A-T today in the United States, at the very outside estimate = 108 births/year x 40 years = 4320 cases. With a U.S. population of 321,251,852 (United States Census Bureau) the highest estimated prevalence of A-T is 4320:321,251,852 or 1:74,364.
GTX-102—R&D and Clinical Studies to Date
In a multicenter, double-blind, randomized, placebo-controlled crossover trial conducted in Italy, Zannolli et al. studied the effect of an oral liquid solution of betamethasone on the reduction of ataxia symptoms in 13 children (between ages 2 to 8 years) with A-T. Patients were randomly assigned to first receive either betamethasone or placebo at a dose of 0.1 mg/kg/day for 30 days: at full dose for the first 10 days, at a tapered dose on days 11–20 (i.e., for 4 days, 0.075 mg/kg/day; for 4 days, 0.050 mg/kg/day; and for 2 days, 0.025 mg/kg/day); and at full dose for the last 10 days (the full dose was tapered in the middle of the treatment phase to reduce risk from potential functional suppression of the hypothalamus-hypophysis-adrenal axis). Each phase of the trial was followed by a washout period of 30 days. The primary outcome measure was the reduction in ataxia symptoms as assessed by the International Cooperative Ataxia Rating Scale (“ICARS”).
In the trial, oral liquid betamethasone reduced the ICARS total score by a median of 13 points in the intent-to-treat (“ITT”) population and 16 points in the per-protocol (“PP”) population (the median percent decreases of ataxia symptoms of 28% and 31%, respectively). In the ITT population, significant improvements were observed in the posture and gait disturbance (p = 0.02), kinetic function (p = 0.02), and speech disorders ICARS subscales (p = 0.02), but not in the oculomotor disorders subscale (p > 0.05). Similar results were found in the PP population. Adverse events in the trial were minimal, with no compulsory withdrawals and only minor side effects that did not require medical intervention. Small increases in body weight were observed in 12 patients on betamethasone and in 4 patients on placebo. Moon face was present in 8 patients on betamethasone. Clinical study results in A-T patients administered oral betamethasone indicated that betamethasone significantly reduced ICARS total score relative to placebo (P = 0.01). The median ICARS change score (change in score with betamethasone minus change in score with placebo) was -13 points (95% confidence interval for the difference in medians was -19 to -5.5 points).
13
|
|
Clinical Study Results in A-T Patients Administered Oral Betamethasone |
|
|||||||||||||
|
|
Placebo |
|
Betamethasone |
|
Efficacy |
|
|||||||||
ICARS |
|
Day -1 |
|
Day 31 |
|
Day -1 |
|
Day 31 |
|
Db |
|
95% Cl for the |
|
P valuec |
|
|
Total score |
|
46 (14-69) |
|
41.5 (26-68) |
|
50 (20-68) |
|
33 (19-55) |
|
-13 (-28 to 14) |
|
-19 to -5.5 |
|
|
0.01 |
|
I. Posture and gait disturbance |
|
13.5 (3-30) |
|
14.5 (7-30) |
|
18 (7-29) |
|
9 (4-26) |
|
-5 (-15 to 5) |
|
-9.5 to -1.5 |
|
|
0.02 |
|
II. Kinetic function |
|
22 (6-32) |
|
20.5 (13-31) |
|
23 (10-33) |
|
18 (8-28) |
|
-8 (-15 to 10) |
|
-10 to -0.5 |
|
|
0.02 |
|
III. Speech disorder |
|
3 (1-5) |
|
2.5 (2-5) |
|
3 (2-5) |
|
2 (1-5) |
|
-1 (-3 to 1) |
|
-2.5 to -0.5 |
|
|
0.02 |
|
IV. Oculomotor disorders |
|
3 (2-5) |
|
3.5 (1·5) |
|
3 (1-5) |
|
3 (1-5) |
|
0 (-2 to 2) |
|
-2 to 1 |
|
|
0.43 |
|
Betamethasone significantly reduced ICARS total score relative to placebo (P = .01). The median ICARS change score (change in score with Betamethasone minus change in score with placebo) was -13 points (95% CI for the difference in medians was -19 to -5.5 points).
Based on the Zannolli data, we believe GTX-102 concentrated oral spray has the potential to provide clinical benefits in decreasing A-T symptoms, including assessments of posture and gait disturbance and kinetic, speech and oculomotor functions. In addition, GTX-102 may ease drug administration for patients experiencing A-T given its application of 1-3x/day of 140µL of concentrated betamethasone liquid spray onto the tongue using a more convenient metered dose spray, as these A-T patients typically have difficulty swallowing (lefton-greif 2000).
GTX-102 PK Data to Date:
GTX-102 administered as a concentrated oral spray achieves similar blood levels at only 1/70th the volume of an oral solution of betamethasone. This is important for A-T patients who have difficulties swallowing large volumes of liquids, and it could help to reduce the side effects common with chronic use of a glucocorticosteroid drug.
GTX-102 Near-Term Milestones: Conduct PK Bridging and Confirmatory Phase 3 Clinical Trials
Acasti Pharma US has licensed the data from the multicenter, double-blinded, randomized, placebo-controlled crossover trial from Azienda Ospedaliera Universitaria Senese, Siena, Italy, where Dr. Zannolli et. al. studied the effect of oral liquid solution of betamethasone to reduce ataxia symptoms in patients with A-T. Note that this oral liquid solution is not approved in the United States, and therefore is not available for clinical use. Betamethasone is only available in the United States as an injectable or as a topical cream. However, this license gives Acasti Pharma US the right to reference the study’s data in its NDA filing. On November 12, 2015, Acasti Pharma US submitted the data from the Zannolli study to the FDA’s Division of Neurology at a pre-Investigational New Drug (“IND”) meeting and received guidance from the agency on the regulatory requirements to seek approval.
Based on such FDA guidance, we plan to initiate a PK bridging study of our proprietary concentrated oral spray as compared to the oral liquid solution of betamethasone used in the Zannolli study and against the injectable form of betamethasone that is approved in the U.S. in the second calendar quarter of 2022. We expect to report the results of this study before the end of 2022. Based on the FDA’s guidance and assuming the PK bridging study meets its primary endpoint, we plan to conduct a confirmatory Phase 3 safety and efficacy trial in A-T patients. The Phase 3 study is expected to be initiated in the first half of 2023. If both studies meet their primary endpoints, an NDA filing under Section 505(b)(2) would follow.
14
GTX-101 Overview
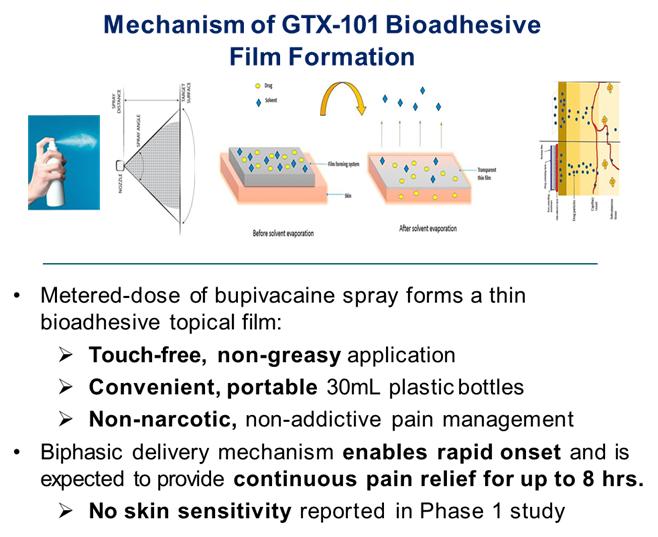
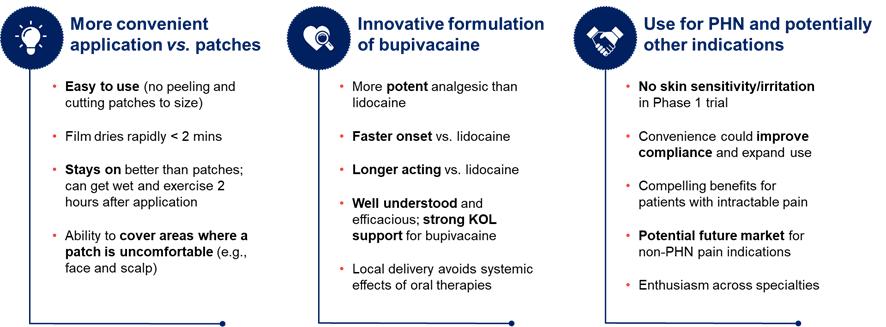
GTX-101 is a non-narcotic, topical bio-adhesive film-forming bupivacaine spray designed to ease the symptoms of patients suffering with postherpetic neuralgia (“PHN”). GTX-101’s metered-dose of bupivacaine spray forms a thin bio-adhesive topical film on the surface of the patient’s skin, which enables a touch-free, non-greasy application. It also comes in convenient, portable 30 ml plastic bottles. Unlike oral gabapentin and lidocaine patches, we believe that the biphasic delivery mechanism of GTX-101 has the potential for rapid onset and continuous pain relief for up to eight hours. No skin sensitivity was reported in a Phase 1 study.
Source: Third party primary market research (2022)
About Postherpetic Neuralgia (PHN)
PHN is neuropathic pain due to damage caused by the varicella zoster virus (“VZV”). Infection with the VZV causes two distinct clinical conditions. Primary VZV infection causes varicella (i.e., chickenpox), a contagious rash illness that typically occurs among young children. Secondary VZV can reactivate clinically, decades after initial infection, to cause herpes zoster (“HZ”), otherwise known as shingles. Acute HZ arises when dormant virus particles, persisting within an affected sensory ganglion from the earlier, primary infection with VZV become reactivated when cellular immunity to varicella decreases. Viral particles replicate and may spread to the dorsal root, into the dorsal horn of the spinal cord, and through peripheral sensory nerve fibers down to the level of the skin. Viral particles also may circulate in the blood. This reactivation is accompanied by inflammation of the skin, immune response, hemorrhage, and destruction of peripheral and central neurons and their fibers. Following such neural degeneration, distinct types of pathophysiological mechanisms involving both the central and peripheral nervous systems may give rise to the severe nerve pain associated with PHN.
While the rash associated with HZ typically heals within two to four weeks, the pain may persist for months or even years, and this PHN manifestation is the most common and debilitating complication of HZ. There is currently no consensus definition for PHN, but it has been suggested by the Centers for Disease Control and Prevention (“CDC”) that PHN is best defined as pain lasting at least three months after resolution of the rash.
PHN is associated with significant loss of function and reduced quality of life, particularly in the elderly. It has a detrimental effect on all aspects of a patients’ quality of life. The nature of PHN pain varies from mild to excruciating in severity, constant, intermittent, or triggered by trivial stimuli. Approximately half of patients with PHN describe their pain as “horrible” or “excruciating,” ranging in duration from a few minutes to constant on a daily or almost daily basis (Katz, 2004). The pain can disrupt sleep, mood, work, and activities of daily living, adversely impacting the quality of life and leading to social withdrawal and depression. PHN is the number-one cause of intractable, debilitating pain in the elderly, and has been cited as the leading cause of suicide in chronic pain patients over the age of 70 (Hess, 1990).
15
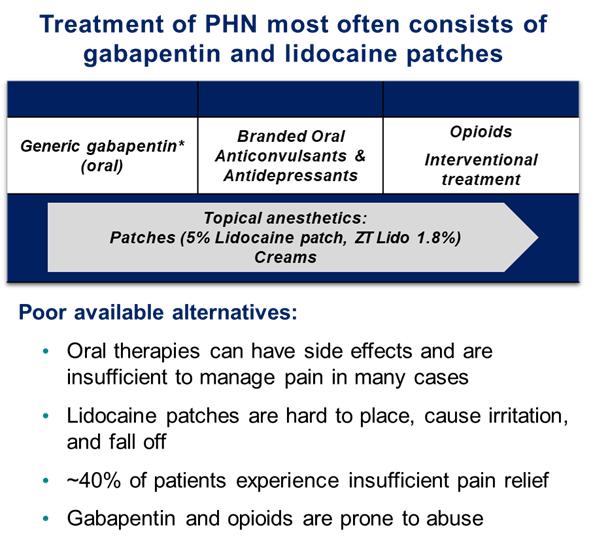
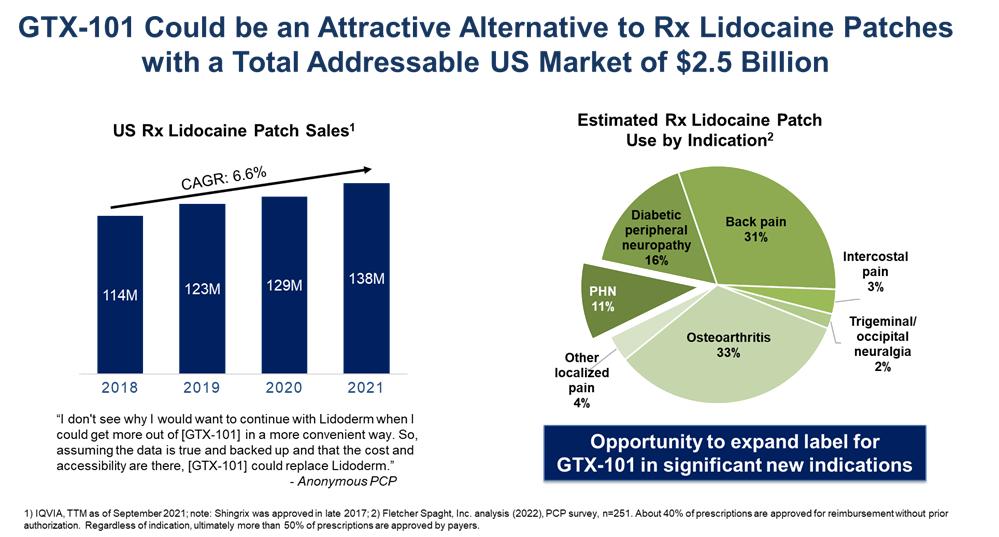
Current treatment of PHN most often consists of oral gabapentin (first line) and prescription lidocaine patches (second line), and refractory cases may be prescribed opioids to address persistent pain. Gabapentin and opioid abuse have continued to proliferate, and lidocaine patches are suboptimal for many reasons. An independent third party market research firm commissioned by Acasti interviewed more than 250 physicians who regularly treat PHN patients, and found that approximately 40% of patients using lidocaine patches experience insufficient pain relief. Lidocaine patches are difficult to use, fall off, and look unsightly with possible skin sensitivity and irritation. Additionally, it can take up to two weeks for an optimal analgesic effect to be achieved. Prescription lidocaine patches are only approved for PHN, and the market is currently made up of both branded and generic offerings. It is estimated that PHN affects approximately 120,000 patients per year in the United States. According to the third-party report commissioned by Acasti, the total addressable market for GTX-101 could be as large as $2.5 billion, consisting of approximately $200 million for PHN pain and $2.3 billion for non-PHN pain.
GTX-101 R&D History and Clinical Studies Completed to Date
To date, Acasti Pharma US has conducted three Phase I studies in healthy volunteers to assess the PK, safety and tolerability of GTX-101 and to determine the plasma levels of bupivacaine HCl administered as a single dose in various concentrations, namely 30 mg (three sprays), 50 mg (five sprays), 70 mg (seven sprays) or 100 mg (ten sprays).
The initial study was conducted to determine the PK levels of GTX-101 following a single dose of either 30 mg, 50 mg or 70 mg, and to compare the plasma levels to those produced by a single 30 mg dose of injectable bupivacaine (SENSORCAINETM). In this study, the plasma levels of bupivacaine were below the limit of quantitation (limit of quantitation (“LOQ”) was 1.00 ng/mL) for almost all subjects administered GTX-101, and at almost all time points. Mean Cmax and AUC0-T for injectable bupivacaine were 129.3 ng/mL and 517.7 ng/mL, respectively. Bupivacaine was not detected due to assay sensitivity limited to 1ng/ml.
The second study investigated the PK, safety, and tolerability of a single 100 mg dose (ten sprays) of GTX-101. The mean bupivacaine Cmax in this study was 1.249 ng/mL for the first set of samples and 1.067 ng/mL for the second set of samples; the two mean values differing from each other by less than 20%. The LOQ of the bioanalytical method used for this study was 5 pg/mL. This study confirmed the Cmax values as being similar from two sets of samples collected from the same patients at the same time points.
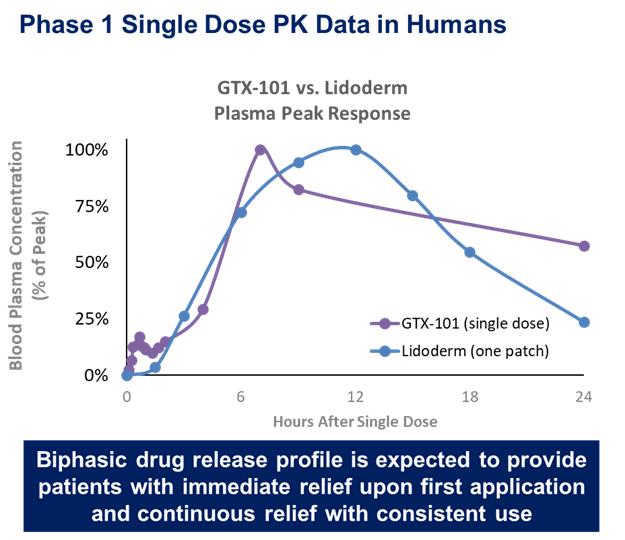
In the third study, the PK, safety, and tolerability of a single 100 mg dose (ten sprays) of GTX-101 were again investigated. This study was a single-center, non-randomized, single dose, open-label, 1-period, 1-treatment design in 10 healthy male and female subjects. The PK results show the maximum observed plasma concentration of bupivacaine was reached within 20 to 48 hours for all subjects. The maximum concentration reached was 19.59 ng/mL. This study confirmed that bupivacaine delivered as a spray (GTX-101) is well absorbed through the skin, as demonstrated in the graph below, while very little is absorbed systemically.
16
In all three studies, the administration of GTX-101 to healthy volunteers was safe and well tolerated. In addition, no evidence of skin irritation was observed at the application site following the spray administrations.
GTX-101 Near-Term Milestones: Conduct Dose Ranging Phase 1 Clinical Trials of GTX-101
We believe that the PHN pain market will continue to grow, and non-opioid products like GTX-101 that can relieve PHN pain more quickly and in a sustained manner by means of a more efficient delivery system, will be an attractive therapy option for patients and physicians. GTX-101 is administered by spraying a proprietary bupivacaine formulation over the affected area, which we believe has the potential to provide several advantages over currently marketed products such as the lidocaine patch, including faster onset of action, sustained pain relief, possibly lower dosing requirements and improved dosing convenience, all which could lead to increased patient compliance.
The data from the single dose Phase 1 clinical trial for topical bupivacaine spray along with regulatory guidance from the FDA’s Division of Anesthesiology that was received at a pre-IND meeting on April 18, 2018 has informed the design of additional preclinical toxicology studies and a clinical and regulatory pathway to approval. We expect to report the results of a minipig skin sensitivity study in the third calendar quarter of 2022. We also plan to initiate a single dose and a multiple ascending dose study in healthy human volunteers in the third calendar quarter of 2022. We expect to report both of these results for these studies before the end of 2022. Results from these pre-clinical and clinical studies are required before we can initiate our program in PHN patients, which we expect will start in early 2023.
Overall Commercialization Strategy
We plan to retain our worldwide commercialization rights for some of our key drug candidates, while for other drug candidates we might consider collaboration opportunities to maximize market penetration and returns. If we receive regulatory approval, we expect to build a small and focused commercial organization in the United States to market and sell GTX-104 and GTX-102. We believe the patient populations and medical specialists for these indications are sufficiently concentrated to allow us to cost-effectively promote these drug products following approval for commercial sale. Given that GTX-101 will be targeted to a larger primary care and pain specialist market, if GTX-101 receives regulatory approval, it is likely we will seek commercial partnerships to fully exploit the market potential of this drug product.
As product candidates advance through the pipeline, our commercial plans may change. Clinical data, the size of the development programs, the size of the target market, the size of a commercial infrastructure and manufacturing needs may all have influence on U.S., European Union, and rest-of-world strategies.
Manufacturing and Supply
We currently do not own any manufacturing facilities. The manufacture of our pipeline of drug candidates is highly reliant on complex techniques and personnel aseptic techniques, which present significant challenges and require specialized expertise. Further, these processes undergo a high level of scrutiny by regulatory agencies. Consequently, we utilize a network of third-party contract manufacturers (“CMOs”) for manufacturing of our drug candidates. All CMOs are monitored and evaluated by us to assess compliance with regulatory requirements.
We work with and regularly inspect our manufacturers to review the manufacturing process for our drug candidates and to provide input on quality issues. We have addressed the risk of supply chain disruptions through risk management strategies designed to mitigate the effects of any disruptions. While this strategy creates additional effort and requires maintaining dialogue and traveling to and overseeing production at multiple facilities, we believe our manufacturing risks are better managed by utilizing a range of specialized third-party manufacturers at diverse locations.
17
Intellectual Property Portfolio
We have a strong and multi-layered intellectual property protection strategy, which we believe will create barriers to entry and solidify our position in the market. All of our leading pipeline products have received orphan status designation from the FDA, which could result in 7 years of marketing exclusivity in the United States and 10 years in Europe, provided they receive the final marketing authorizations from the applicable government agencies, and they can meet the conditions for receiving such marketing exclusivity. In addition, we protect our drug candidates through a well-defined patent filing strategy. Our patent estate includes more than 40 granted and pending patents in various global jurisdictions, including 4 U.S. issued patents and 7 filed U.S. patent applications. We believe that our intellectual property portfolio, consisting primarily of composition and method-of-use patents, will protect the market value of our products by extending exclusivity beyond what is granted through the orphan designation. We intend to continue to build our patent portfolio by filing for patent protection on new developments with respect to our product candidates. We expect that these patents will, if and when issued, allow us to list our own patents in the Orange Book: Approved Drug Products with Therapeutic Equivalence issued by the FDA, to which potential competitors will be required to certify upon submission of their applications referencing our drug products, if approved.
We strive to protect and enhance the proprietary technology, inventions, and improvements that are commercially important to the development of our business, including seeking, maintaining, and defending patent rights, whether developed internally or licensed from third parties. We also rely on trade secrets relating to manufacturing know-how, continuing technological innovation and in-licensing opportunities to develop, strengthen, and maintain our proprietary position. We may also rely on regulatory protections afforded through orphan drug status, data exclusivity, market exclusivity, and patent term extensions, where available.
We are actively seeking U.S. and international patent protection for a variety of technologies and intend to seek patent protection or rely upon trade secret rights to protect other technologies that may be used to discover and validate targets and that may be used to identify and develop novel pharmaceutical products. We seek these protections, in part, through confidentiality and proprietary information agreements.
Individual patents extend for varying periods depending on the date of filing or the date of issuance, and the legal term of patents in the countries in which they are obtained. Generally, utility patents issued for applications filed in the United States are granted a term of 20 years from the earliest effective filing date of a non-provisional patent application. In addition, in certain instances, a patent term can be extended to recapture a portion of the U.S. Patent and Trademark Office delay in issuing the patent as well as a portion of the term effectively lost as a result of the FDA regulatory review period. However, as to the FDA component, the restoration period cannot be longer than 5 years and the total patent term including the restoration period must not exceed 14 years following FDA approval. The duration of foreign patents varies in accordance with provisions of applicable local law, but typically is also 20 years from the earliest effective filing date. The actual protection afforded by a patent may vary on a product-by-product basis from country to country and can depend upon many factors, including the type of patent, the scope of its coverage, the availability of regulatory-related extensions, the availability of legal remedies in a particular country and the validity and enforceability of the patent.
Acasti Pharma US has several issued U.S. patents and patent applications as well as patents and patent applications in other jurisdictions. Four patents for GTX-104 have been granted in the United States. One patent for GTX-101 has been granted in Europe, China, Mexico, Japan and South Africa. One patent for GTX-102 has been granted in Japan.
Recent Developments
On March 22, 2022 we announced the awards of several patents relating to our three lead drug candidates. The European Patent Office provided notice of intention to grant the Company’s composition of matter patent for GTX-104. The patent is expected to be valid until 2037. The United States Patent and Trademark Office also issued a notice of allowance for our composition of matter patent for GTX-102. The patent is expected to be valid until 2037. Finally, the Japanese Patent Office granted a composition of matter patent for our GTX 101 topical spray. The granted patent is valid until 2036.
On March 25, 2022 we announced the appointment of Michael L. Derby to our board of directors, filling the remaining seat on our board of directors recommended by the former Grace stockholders as contemplated by the merger agreement for the Grace transaction.
On May 18, 2022, we announced that the top line results of the PK bridging study with IV GTX-104, our lead drug candidate for the treatment of SAH, met all its planned study endpoints. The primary objective of the study was to evaluate the relative bioavailability of IV GTX-104 compared to oral nimodipine in healthy adult male and female subjects, while the secondary objective was to assess its safety and tolerability.
On May 23, 2022 we announced that we have retained one of the industry's leading investor relations firms, Lytham Partners, LLC, to lead a strategic investor relations and shareholder communication program for the Company.
On June 14, 2022 we announced the issuance of additional patents for GTX-104 and GTX-101. Three composition of matter patents were issued for GTX-104 by The United States Patent and Trademark Office, the Japanese Patent Office, and the Australian Patent Office. Additionally, one new patent for GTX-104 was awarded by the Indian Patent Office. These granted patents are all valid until 2037.
COVID-19 Update
To date, the ongoing COVID-19 pandemic has not caused significant disruptions to our business operations and research and development activities.
The extent to which the COVID-19 pandemic impacts our business and prospects and the timing and completion of future clinical trials for our new drug candidates will depend on future developments, which are highly uncertain and cannot be predicted, including new information which may emerge concerning the severity of the COVID-19 pandemic and the actions to contain the COVID-19 pandemic or treat its impact, among others.
Corporate Structure
Acasti was incorporated on February 1, 2002 under Part 1A of the Companies Act (Québec) under the name “9113-0310 Québec Inc.” On February 14, 2011, the Business Corporations Act (Québec), or QBCA, came into effect and replaced the Companies Act (Québec). We are now governed by the QBCA. On August 7, 2008, pursuant to a Certificate of Amendment, we changed our name to “Acasti Pharma Inc.”, our share capital description, the provisions regarding the restriction on securities transfers and our borrowing powers. On November 7, 2008, pursuant to a Certificate of Amendment, we changed the provisions regarding our borrowing powers. We became a reporting issuer in the Province of Québec on November 17, 2008. On December 18, 2019, we incorporated a new wholly owned subsidiary named Acasti Innovation AG, or AIAG, under the laws of Switzerland for the purpose of future development of our intellectual property and for global distribution of our products. AIAG currently does not have any operations. On August 27, 2021, Acasti completed its acquisition of Grace via a merger following the approval of Acasti’s shareholders and Grace’s stockholders. Following completion of the merger, Grace became a wholly owned subsidiary of Acasti and was renamed Acasti Pharma U.S. Inc.
18
Available Information
This annual report on Form 10-K, our quarterly reports on Form 10-Q, our current reports on Form 8-K, and any amendments to these reports are filed, or will be filed, as applicable, with the SEC, and the Canadian Securities Administrators, or CSA. These reports are available free of charge on our website, www.acastipharma.com, as soon as reasonably practicable after we electronically file such reports with or furnish such reports to the SEC and the CSA. Information contained on, or accessible through, our website is not a part of this annual report, and the inclusion of our website address in this document is an inactive textual reference.
Additionally, our filings with the SEC may be accessed through the SEC’s website at www.sec.gov and our filings with the CSA may be accessed through the CSA’s System for Electronic Document Analysis and Retrieval at www.sedar.com.
Item 1A. Risk Factors
Summary of Risk Factors
We are providing the following summary of the risk factors contained in this Annual Report on Form 10-K to enhance the readability and accessibility of our risk factor disclosures. This summary does not address all of the risks that we face. We encourage you to carefully review the full risk factors contained in this Annual Report on Form 10-K in their entirety for additional information regarding the material factors that make an investment in our securities speculative or risky. The primary categories by which we classify risks include: (i) general risks related to our company; (ii) risks relating to our business; (iii) risks relating to the development, testing and commercialization of our products; (iv) risks relating to our intellectual property; (v) risks relating to our dependence on third parties; and (vi) risks relating to ownership of our common shares. Set forth below within each of these categories is a summary of the principal factors that make an investment in our common shares speculative or risky.
General Risks Related to the Company
Risk Factors Relating to our Business
Risks Related to Development, Testing and Commercialization of Our Products
19
Risks Relating to our Intellectual Property
20
Risks Related to Our Dependence on Third Parties
Risks related to Tax
Risks Relating to Ownership of our Common Shares
Any investment in our common shares involves a high degree of risk. The following risk factors and other information included in this annual report on Form 10-K should be carefully considered. If any of these risks actually occur, our business, financial condition, prospects, results of operations or cash flow could be materially and adversely affected, and you could lose all or a part of the value of your investment. Additional risks or uncertainties not currently known to us, or that we deem immaterial, may also negatively affect our business operations.
General Risks Related to the Company
We may not achieve our publicly announced milestones on time, or at all.
From time to time, we may publicly announce the timing of certain events that we expect to occur, such as the anticipated timing of results from our clinical trials and the timing of an upcoming NDA filing. These statements are forward-looking and are based on the best estimate of management at the time relating to the occurrence of the events. However, the actual timing of these events may differ from what has been publicly disclosed. The timing of events such as completion of a clinical trial, discovery of a new product candidate, filing of an application to obtain regulatory approval, beginning of commercialization of products, completion of a strategic partnership, or announcement of additional clinical trials for a product candidate may ultimately vary from what is publicly disclosed. These variations in timing may occur as a result
21
of different events, including the nature of the results obtained during a clinical trial or during a research phase, problems with a supplier or a distribution partner or any other event having the effect of delaying the publicly announced timeline. We undertake no obligation to update or revise any forward-looking information, whether as a result of new information, future events or otherwise, except as otherwise required by law. Any variation in the timing of previously announced milestones could have a material adverse effect on our business, financial condition or operating results and the trading price of our common shares.
We are heavily dependent on the success of our lead drug candidates, GTX-104, GTX-102 and GTX-101.
Our business and future success are substantially dependent on our ability to successfully and timely develop, obtain regulatory approval for, and commercialize our lead product candidate, GTX-104. Any delay or setback in the development of GTX-104 could adversely affect our business. Our planned development, approval and commercialization of GTX-104 may fail to be completed in a timely manner or at all. Our other product candidates, GTX-102 and GTX-101, are at an earlier development stage and we will require additional time and resources to develop and seek regulatory approval for such drug candidates and, if we are successful, to proceed with commercialization. We cannot provide assurance that we will be able to obtain approval for any of our drug candidates from the FDA or any foreign regulatory authority or that we will obtain such approval in a timely manner.
We may not be able to maintain our operations and advance our research and development and commercialization of our lead drug candidates without additional funding.
We have incurred operating losses and negative cash flows from operations since our inception. To date, we have financed our operations through public offerings and private placements of securities, proceeds from exercises of warrants, rights and options, and receipt of research tax credits and research grant programs. Our cash and cash equivalents and short-term investments (including restricted investments) were $43.7 million as of March 31, 2022 and $60.7 million as of March 31, 2021.
Our current assets, as of March 31, 2022, are projected to support our current liabilities as at that date when combined with the projected level of our expenses for the next twelve months, including fully funding the completion of our Phase 3 program for GTX-104. We expect that additional time and capital will be required by us to file an NDA to obtain FDA approval for GTX-104 in the United States, to further scale up our manufacturing capabilities, and to complete marketing and other pre-commercialization activities. Consequently, we expect to require additional capital to fund our daily operating needs beyond the next twelve months. Based on a conservative estimate, we believe that our existing cash and cash equivalents will enable us to fund our operating expenses and capital expenditure requirements beyond the completion of our Phase 3 trials for GTX-104. To fully execute our business plan, we plan to raise the necessary capital primarily through additional securities offerings and multiple sources of non-dilutive capital, such as grants or loans and strategic alliances. If we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we may have to significantly delay the research and development and commercial launch of our lead drug candidates. Unexpected negative results in our clinical programs for our lead drug candidates may affect our ability to raise additional capital and/or complete strategic development and/or distribution partnerships to support the commercial launch of our drug candidates. Additional funding from third parties may not be available on acceptable terms or at all to enable us to continue with the research and development and commercialization of our lead drug candidates.
Our future results will suffer if we do not effectively manage our expanded operations.
As a result of the merger, we have become a larger company than either of Acasti or Grace prior to the merger, and our business has become more complex. There can be no assurance that we will effectively manage the increased complexity without experiencing operating inefficiencies or control deficiencies. Significant management time and effort is required to effectively manage the increased complexity of the larger organization and if we fail to successfully do so it could have a material adverse effect on our business, financial condition, results of operations and growth prospects. In addition, as a result of the merger, our financial statements and results of operations in prior years may not provide meaningful guidance to form an assessment of our prospects or the potential success of our future business operations.
Business disruptions could seriously harm our future revenue and financial condition and increase our costs and expenses.
Our operations, and those of our suppliers, third party manufacturers and other contractors and consultants could be subject to earthquakes, power shortages, telecommunications failures, water shortages, floods, hurricanes, typhoons, fires, extreme weather conditions, medical pandemics and other natural or man-made disasters or business interruptions, for which we are predominantly self-insured. The occurrence of any of these business disruptions could seriously harm our operations and financial condition and increase our costs and expenses. We rely on third-party manufacturers to manufacture our products. Our ability to obtain supplies of candidate products could be disrupted if the operations of our manufacturers and suppliers are affected by a man-made or natural disaster or other business interruption.
We may be subject to foreign exchange rate fluctuations.
Our reporting currency is the U.S. dollar. However, many of our expenses currently are and/or are expected to be, denominated in foreign currencies, including Canadian dollars. As we previously completed financings in both Canadian and U.S. dollars, both currencies are maintained and used to make required payments in the applicable currency. Though we plan to implement measures designed to reduce our foreign exchange rate exposure, the U.S. dollar/Canadian dollar and U.S. dollar /European euro exchange rates have fluctuated significantly in the recent past and may continue to do so, which could have a material adverse effect on our business, financial position and results of operations.
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our share price and trading volume could decline.
The trading market for our common shares will depend in part on the research and reports that securities or industry analysts publish about us or our business. We do not currently have limited research coverage by securities and industry analysts. If few or no securities or industry analysts commence coverage of our company, the trading price for our common shares could be negatively impacted. If one or more of the analysts who covers us downgrades our common shares or publishes inaccurate or unfavorable research about our business, our share price would likely decline. If one or more of these analysts ceases coverage of us or fails to publish reports on us regularly, demand for our common shares could decrease, which could cause our share price and trading volume to decline.
Lawsuits have been filed, and other lawsuits may be filed, against us and members of our board of directors challenging the Grace merger, and an adverse ruling in any such lawsuit may result in an award of damages against us.
In connection with the Grace merger, four shareholder lawsuits were filed. Two of the lawsuits have been voluntarily dismissed without prejudice and the remaining two have been consolidated. The lawsuits generally allege that our public disclosures pertaining to the Grace merger omit material facts in purported violation of Section 14(a) of the Exchange Act and Rule 14a-9 promulgated thereunder, and that members of our board of directors are liable for those purported omissions under Section 20(a) of the Exchange Act. The relief sought in the lawsuits includes, among other things, to enjoin the consummation of the merger, to award damages purportedly caused by the alleged omissions, and to award plaintiffs’ attorneys’ fees and other costs. It is possible that additional lawsuits asserting similar claims could be filed. We strongly believe the allegations in the lawsuits are frivolous and without merit, and are vigorously defending against them. The results of complex legal proceedings are difficult to predict.
22
Moreover, the pending litigation is, and any future additional litigation could be, time consuming and expensive and could divert management’s attention away from its regular business.
Risk Factors Relating to our Business
Our future success depends on our ability to retain key executives and to attract, retain and motivate qualified personnel.
We are highly dependent on the principal members of our executive team. Any of our executive officers could leave our employment at any time, as all of our employees are “at will” employees. Recruiting and retaining other qualified employees for our business, including scientific and technical personnel, will also be critical to our success. There is currently a shortage of skilled executives and other personnel in our industry, which is likely to continue. As a result, competition for skilled personnel is intense and the turnover rate can be high. We may not be able to attract and retain personnel on acceptable terms given the competition among numerous pharmaceutical companies for individuals with similar skill sets. In addition, failure to succeed in clinical studies may make it more challenging to recruit and retain qualified personnel. The inability to recruit key executives or the loss of the services of any executive or key employee might impede the progress of our development and commercialization objectives.
We will need to expand our organization, and we may experience difficulties in managing this growth, which could disrupt our operations and our ability to compete.
As our company matures, we expect to expand our employee base to increase our managerial, scientific, engineering, operational, sales, marketing, financial and other resources and to hire more consultants and contractors. Future growth would impose significant additional responsibilities on our management, including the need to identify, recruit, maintain, motivate, and integrate additional employees, consultants and contractors. We may not be able to effectively manage the expansion of our operations, which may result in weaknesses in our infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among remaining employees. Future growth could require significant capital expenditures and may divert financial resources from other projects, such as the development of our existing or future product candidates. Our future financial performance and our ability to sell and commercialize our product candidates, if approved, and compete effectively will depend, in part, on our ability to effectively manage any future growth.
We face potential product liability, and if claims are brought against us, we may incur substantial liability.
The use of our product candidates in clinical trials, and the sale of any drug candidates for which we obtain marketing approval, exposes us to the risk of product liability claims. Product liability claims might be brought against us by consumers, healthcare providers, pharmaceutical companies or others selling or otherwise coming into contact with our product candidates. If we cannot successfully defend against product liability claims, we could incur substantial liability and costs. In addition, regardless of merit or eventual outcome, product liability claims may result in:
Our current product liability insurance coverage may not be sufficient to reimburse us for any expenses or losses we may suffer. Moreover, insurance coverage is becoming increasingly expensive, and, in the future, we may not be able to maintain insurance coverage at a reasonable cost or in sufficient amounts to protect us against losses due to liability. A successful product liability claim or series of claims brought against us could cause our share price to decline and, if judgments exceed our insurance coverage, could adversely affect our results of operations and business.
We rely significantly on information technology and any failure, inadequacy, interruption, or security lapse of that technology, including any cybersecurity incidents, could harm our ability to operate our business effectively.
Despite the implementation of security measures, our internal computer systems, and those of third parties with which we contract are vulnerable to damage from cyber-attacks, computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. System failures, accidents or security breaches could cause interruptions in our operations and could result in a material disruption of our drug product development and clinical activities and business operations, in addition to possibly requiring substantial expenditures of resources to remedy. The loss of drug product development or clinical trial data could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and our development programs, and the development of our product candidates could be delayed.
Risks Related to Development, Testing and Commercialization of Our Products
Even if our drug candidates receive regulatory approval in the United States, we may never obtain regulatory approval or successfully commercialize our products outside of the United States.
Our business plan is highly dependent upon our ability to obtain regulatory approval to market and commercialize our lead drug candidates, GTX-104, GTX-102 and GTX-101 in the United States. The failure to do so would have a material adverse effect on our ability to execute on our business plan and generate revenue. In addition, even if we obtain U.S. regulatory approvals to commercialize GTX-104, GTX-102 and GTX-101, we may not be able to do so in other international jurisdictions.
We are subject to uncertainty relating to healthcare reform measures and reimbursement policies which, if not favorable to our drug candidates, could hinder or prevent our drug candidates’ commercial success.
Our ability to commercialize our drug candidates successfully will depend in part on the extent to which governmental authorities, private health insurers and other third-party payors establish appropriate coverage and reimbursement levels for our drug candidates and related treatments. As a threshold for coverage and reimbursement, third-party payors generally require that drug products have been approved for marketing by the FDA. Third-party payors are increasingly imposing additional
23
requirements and restrictions on coverage and limiting reimbursement levels for medical products. These restrictions and limitations influence the purchase of healthcare services and products. The cost containment measures that healthcare payors and providers are instituting and the effect of any healthcare reform could significantly reduce our revenues from the sale of any approved drug. We cannot provide any assurances that we will be able to obtain third-party coverage or reimbursement for our drug candidates in whole or in part.
In the United States, there have been a number of legislative and regulatory changes to the healthcare system in ways that could affect our future revenues and profitability and the future revenues and profitability of our potential customers. Under the prescription drug benefit, Medicare beneficiaries can obtain prescription drug coverage from private sector plans that are permitted to limit the number of prescription drugs that are covered in each therapeutic category and class on their formularies. If our products are not widely included on the formularies of these plans, our ability to market our products to the Medicare population could be harmed.
There also have been, and likely will continue to be, legislative and regulatory proposals at the federal and state levels directed at containing or lowering the cost of healthcare. We cannot predict the initiatives that may be adopted in the future. The continuing efforts of the government, insurance companies, managed care organizations and other payors of healthcare costs to contain or reduce costs of healthcare may adversely affect one or more of the following:
Any of these scenarios could harm our ability to market our products and generate revenues. It is also possible that other proposals having a similar effect will be adopted.
Our commercial success depends upon attaining significant market acceptance of our drug candidates and drug products, if approved, among physicians, nurses, pharmacists, patients and the medical community.
Even if we obtain regulatory approval for our drug product candidates, our drug product candidates may not gain market acceptance among physicians, nurses, pharmacists, patients, the medical community or third-party payors, which is critical to commercial success. Market acceptance of our drug candidates and any drug product for which we receive approval depends on a number of factors, including:
If our drug candidates or drug products, if approved, fail to achieve an adequate level of acceptance by physicians, nurses, pharmacists, patients, and the medical community, we will be unable to generate significant revenues, and we may not become or remain profitable.
Guidelines and recommendations published by government agencies can reduce the use of our drug candidates and drug products, if approved and negatively impact our ability to gain market acceptance and market share.
Government agencies promulgate regulations and guidelines applicable to certain drug classes which may include our drug products and product candidates that we are developing. Recommendations of government agencies may relate to such matters as usage, dosage, route of administration and use of concomitant therapies. Regulations or guidelines suggesting the reduced use of certain drug classes which may include our drug products and product candidates that we are developing or the use of competitive or alternative drug products as the standard of care to be followed by patients and healthcare providers could result in decreased use of our drug candidates or negatively impact our ability to gain market acceptance and market share.
If we are unable to establish sales and marketing capabilities or enter into agreements with third parties to market and sell our drug candidates, we may be unable to generate any revenue.
Although we intend to establish a small, focused, specialty sales and marketing organization to promote GTX-104 and GTX-102, if approved for marketing in the United States, we currently have no such organization and the cost of establishing and maintaining such an organization may exceed the benefit of doing so. Given the size of its potential market, we anticipate that to commercialize GTX-101, we would seek to enter into a strategic partnership with a larger marketing partner, if GTX-101 is approved by the FDA for marketing, and we may not be successful in doing so. If we are unable to establish adequate sales, marketing and distribution capabilities, whether independently or with third parties, we may not be able to generate sufficient product revenue and may not become profitable. We will be competing with many companies that currently have extensive and well-funded marketing and sales operations. Without an internal team or the support of a third party to perform marketing and sales functions, we may be unable to compete successfully against these more established companies.
24
If we obtain approval to commercialize any approved drug products outside of the United States, a variety of risks associated with international operations could materially adversely affect our business.
If any of our drug candidates are approved for commercialization, we may enter into agreements with third parties to market these drug products outside the United States. We expect that we will be subject to additional risks related to entering into international business relationships, including:
If we are unable to differentiate our drug candidates from branded reference drugs or existing generic therapies for similar treatments, or if the FDA or other applicable regulatory authorities approve generic products that compete with any of our drug candidates, our ability to successfully commercialize our drug candidates would be adversely affected.
Although we believe that our drug candidates will be clinically differentiated from branded reference drugs and their generic counterparts, if any, it is possible that such differentiation will not impact our market position. If we are unable to achieve significant differentiation for our product candidates against other drugs, the opportunity for our product candidates to achieve premium pricing and be commercialized successfully would be adversely affected.
In addition to existing branded reference drugs and the related generic products, the FDA or other applicable regulatory authorities may approve generic products that compete directly with our drug candidates, if approved. Once an NDA, including a 505(b)(2) application, is approved, the product covered thereby becomes a “listed drug” which can, in turn, be cited by potential competitors in support of approval of an abbreviated new drug application (“ANDA”). The Federal Food, Drug, and Cosmetic Act, FDA regulations and other applicable regulations and policies provide incentives to manufacturers to create modified, non-infringing versions of a drug to facilitate the approval of an ANDA for generic substitutes. These manufacturers might only be required to conduct a relatively inexpensive study to show that their product has the same active ingredient(s), dosage form, strength, route of administration and conditions of use or labeling as our product candidate and that the generic product is bioequivalent to ours, meaning it is absorbed in the body at the same rate and to the same extent as our drug product. These generic equivalents, which must meet the same quality standards as branded pharmaceuticals, would be significantly less costly than ours to bring to market and companies that produce generic equivalents are generally able to offer their drug products at lower prices. After the introduction of a generic competitor, a significant percentage of the sales of any branded drug product is typically lost to the generic drug product. Accordingly, competition from generic equivalents of our drug candidates would materially adversely impact our ability to successfully commercialize our drug candidates.
We face significant competition from other biotechnology and pharmaceutical companies, and our operating results will suffer if we fail to compete effectively.
The biopharmaceutical industry is intensely competitive and subject to rapid and significant technological change. We expect to have competitors both in the United States and internationally, including major multinational pharmaceutical companies, biotechnology companies and universities and other research institutions.
Many of our competitors have substantially greater financial, technical and other resources, such as larger research and development staff and experienced marketing and manufacturing organizations. If our competitors market products that are more effective, safer or less expensive than our drug products, if any, or that reach the market sooner than our drug products, if any, we may enter the market too late in the cycle and may not achieve commercial success. In addition, the biopharmaceutical industry is characterized by rapid technological change. If we fail to stay at the forefront of technological change, we may be unable to compete effectively. Technological advances or drug products developed by our competitors may render our drug products, if any, or drug candidates obsolete, less competitive or not economical.
We could incur substantial costs and disruption to our business and delays in the launch of our drug candidates if our competitors and/or collaborators bring legal actions against us, which could harm our business and operating results.
We cannot predict whether our competitors or potential competitors, may bring legal actions against us based on our research, development, and commercialization activities, as well as any drug candidates or drug products resulting from these activities, claiming, among other things, infringement of their intellectual property rights, breach of contract or other legal theories. If we are forced to defend any such lawsuits, whether they are with or without merit or are ultimately determined in our favor, we may face costly litigation and diversion of technical and management personnel. These lawsuits could hinder our ability to enter the market early with our drug candidates and thereby hinder our ability to influence usage patterns when fewer, if any, of our potential competitors have entered such market, which could adversely impact our potential revenue from such drug candidates. Some of our competitors have substantially greater resources than we do and could be able to sustain the cost of litigation to a greater extent and for longer periods of time than we could. Furthermore, an adverse outcome of a dispute may require us: to pay damages, potentially including treble damages and attorneys’ fees, if we are found to have willfully infringed a party’s patent or other intellectual property rights; to cease making, licensing or using products that are alleged to incorporate or make use of the intellectual property of others; to expend additional development resources to reformulate our products or prevent us from marketing a certain drug; and to enter into potentially unfavorable royalty or license agreements in order to obtain the rights to use necessary technologies. Royalty or licensing agreements, if required, may be unavailable on terms acceptable to us, or at all.
25
The COVID-19 pandemic, or a similar pandemic, epidemic, or outbreak of an infectious disease, may materially and adversely affect our business and our financial results and could cause a disruption to the development of our drug candidates.
Public health crises such as pandemics or similar outbreaks could adversely impact our business. The coronavirus pandemic is evolving, and has led to the implementation of various responses, including government-imposed quarantines, travel restrictions and other public health safety measures. While to date, the coronavirus pandemic has not had a material adverse effect on our business, any negative impact COVID-19 has to patient enrollment or treatment, or the research and development of our drug candidates could cause costly delays to clinical trial activities, which could adversely affect our ability to obtain regulatory approval for and to commercialize our drug candidates, increase our operating expenses, and have a material adverse effect on our financial results.
Additionally, timely enrollment in planned clinical trials is dependent upon clinical trial sites which could be adversely affected by global health matters, such as pandemics. We plan to conduct clinical trials for our drug candidates in geographies which are currently being affected by the COVID-19 pandemic. Some factors from the COVID-19 pandemic that could delay or otherwise adversely affect enrollment in the clinical trials of our drug candidates, as well as our business generally, include:
These factors arising from COVID-19 could worsen in countries that are already afflicted with COVID-19 or could continue to spread to additional countries. Any of these factors, and other factors related to any such disruptions that are unforeseen, could have a material adverse effect on our business and our results of operation and financial condition. Further, uncertainty around these and related issues could lead to adverse effects on the economy of the United States and other economies, which could impact our ability to raise the necessary capital needed to develop and commercialize our programs and drug candidates.
We are subject to numerous complex regulatory requirements and failure to comply with these regulations, or the cost of compliance with these regulations, may harm our business.
The research, testing, development, manufacturing, quality control, approval, labeling, packaging, storage, record-keeping, promotion, advertising, marketing, distribution, possession and use of our drug candidates, among other things, are subject to regulation by numerous governmental authorities in the United States and elsewhere. The FDA regulates drugs under the Federal Food, Drug, and Cosmetic Act, and implementing regulations. Non-compliance with any applicable regulatory requirements can result in refusal of the governmental authority to approve products for marketing, criminal prosecution and fines, warning letters, product recalls or seizure of products, total or partial suspension of production, prohibitions or limitations on the commercial sale of products or refusal to allow the entering into of federal and state supply contracts. FDA and comparable governmental authorities have the authority to withdraw product approvals that have been previously granted. In addition, the regulatory requirements relating to our drug candidates and drug products, if any, may change from time to time and it is impossible to predict what the impact of any such changes may be.
If the FDA does not conclude that our drug candidates satisfy the requirements for the 505(b)(2) regulatory approval pathway, or if the requirements for approval of any of our drug candidates under Section 505(b)(2) are not as we expect, the approval pathway for our drug candidates will likely take significantly longer, cost significantly more and encounter significantly greater complications and risks than anticipated, and in any case may not be successful.
We intend to seek FDA approval through the 505(b)(2) regulatory pathway for GTX-104, GTX-101 and GTX-102. The Drug Price Competition and Patent Term Restoration Act of 1984, also known as the Hatch-Waxman Act, added Section 505(b)(2) to the Federal Food, Drug and Cosmetic Act (“FDCA”). Section 505(b)(2) permits the filing of an NDA where at least some of the information required for approval comes from studies that were not conducted by or for the applicant.
If the FDA does not allow us to pursue the 505(b)(2) regulatory pathway for GTX-104, GTX-101 or GTX-102 as anticipated, we may need to conduct additional clinical trials, provide additional data and information and meet additional standards for regulatory approval. If this were to occur, the time and financial resources required to obtain FDA approval for our drug candidates would likely substantially increase. Moreover, an inability to pursue the 505(b)(2) regulatory pathway could result in new competitive products reaching the market faster than our drug candidates, which could materially adversely impact our competitive position and prospects. Even if we are allowed to pursue the 505(b)(2) regulatory pathway for a drug candidate, we cannot assure you that we will receive the requisite or timely approvals for commercialization of such drug candidate.
In addition, it is possible that our competitors may file citizens’ petitions with the FDA in an attempt to persuade the FDA that our drug candidates, or the clinical studies that support their approval, contain deficiencies. Such actions by our competitors could delay or even prevent the FDA from approving any NDA that we submit under Section 505(b)(2).
26
Clinical development is a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results. Failure can occur at any stage of clinical development.
Clinical testing, even when utilizing the 505(b)(2) pathway, is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process, even with active ingredients that have previously been approved by the FDA as safe and effective. The results of preclinical studies and early clinical trials of our drug candidates may not be predictive of the results of later stage clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials.
Our drug candidates are in various stages of development. Clinical trial failures may occur at any stage and may result from a multitude of factors both within and outside our control, including flaws in formulation, adverse safety or efficacy profile and flaws in trial design, among others. If the trials result in negative or inconclusive results, we or our collaborators may decide, or regulators may require us, to discontinue trials of our drug candidates or conduct additional clinical trials or preclinical studies. In addition, data obtained from trials and studies are susceptible to varying interpretations, and regulators may not interpret our data as favorably as we do, which may delay, limit or prevent regulatory approval. For these reasons, our future clinical trials may not be successful.
Delays in clinical trials are common and have many causes, and any delay could result in increased costs to us and could jeopardize or delay our ability to obtain regulatory approval and commence drug product sales. We may also find it difficult to enroll patients in our clinical trials, which could delay or prevent development of our drug candidates.
We may experience delays in clinical trials of our drug candidates. Our planned clinical trials may not begin on time, have an effective design, enroll a sufficient number of patients or be completed on schedule, if at all. Our clinical trials can be delayed for a variety of reasons, including:
If initiation or completion of our planned clinical trials is delayed for any of the above reasons or other reasons, our development costs may increase, our regulatory approval process could be delayed and our ability to commercialize and commence sales of our drug candidates could be materially harmed, which could have a material adverse effect on our business.
In addition, identifying and qualifying patients to participate in clinical trials of our drug candidates is critical to our success. The timing of our clinical trials depends on the speed at which we can recruit patients to participate in testing our drug candidates as well as completion of required follow-up periods. We may not be able to identify, recruit and enroll a sufficient number of patients, or those with required or desired characteristics or to complete our clinical trials in a timely manner. Patient enrollment is and completion of the trials are affected by a variety of factors, including:
27
Our drug products or drug candidates may cause adverse effects or have other properties that could delay or prevent their regulatory approval or limit the scope of any approved label or market acceptance, or result in significant negative consequences following marketing approval, if any.
As with many pharmaceutical and biological products, treatment with our drug products or drug candidates may produce undesirable side effects or adverse reactions or events. Although the nature of our drug products or drug candidates as containing active ingredients that have already been approved means that the side effects arising from the use of the active ingredient or class of drug in our drug products or drug candidates is generally known, our drug products or drug candidates may still cause undesirable side effects, which may harm our business, financial condition and prospects significantly.
Further, if any of our drug products cause serious or unexpected side effects after receiving market approval, a number of potentially significant negative consequences could result, including:
Any of these events could prevent us from achieving or maintaining market acceptance of the affected drug product or drug candidate and could substantially increase the costs of commercializing our drug products and drug candidates.
The regulatory approval processes of the FDA and comparable foreign authorities are lengthy, time consuming and inherently unpredictable, and if we are ultimately unable to obtain regulatory approval for our drug candidates, our business will be substantially harmed.
The time required to obtain approval by the FDA and comparable foreign authorities is unpredictable but typically takes many years following the commencement of clinical trials and depends upon numerous factors, including the substantial discretion of the regulatory authorities. In addition, approval policies, regulations or the type and amount of clinical data necessary to gain approval may change during the course of a drug candidate’s clinical development and may vary among jurisdictions. It is possible that none of our existing drug candidates or any drug candidates we may seek to develop will ever obtain regulatory approval in the United States or other jurisdictions.
Our drug candidates could fail to receive regulatory approval for many reasons, including the following:
This lengthy approval process as well as the unpredictability of future clinical trial results may result in us failing to obtain regulatory approval to market our drug candidates, which would harm our business, results of operations and prospects significantly.
We have limited experience using the 505(b)(2) regulatory pathway to submit an NDA or any similar drug approval filing to the FDA, and we cannot be certain that any of our drug candidates will receive regulatory approval. If we do not receive regulatory approvals for our drug candidates, we may not be able to continue our operations. Even if we successfully obtain regulatory approvals to market one or more of our drug candidates, our revenue will be dependent, to a significant extent, upon the size of the markets in the territories for which we gain regulatory approval. If the markets for patients or indications that we are targeting are not as significant as we estimate, we may not generate significant revenue from sales of such drug products, if approved.
An NDA submitted under Section 505(b)(2) subjects us to the risk that we may be subject to a patent infringement lawsuit that would delay or prevent the review or approval of our drug candidate. The FDA and other regulatory agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses.
Our drug candidates will be submitted to the FDA for approval under Section 505(b)(2) of the FDCA. Section 505(b)(2) permits the submission of an NDA where at least some of the information required for approval comes from studies that were not conducted by, or for, the applicant and on which the applicant has not obtained a right of reference. The 505(b)(2) application would enable us to reference published literature and/or the FDA’s previous findings of safety and effectiveness for the branded reference drug. For NDAs submitted under Section 505(b)(2) of the FDCA, the patent certification and related provisions of the Hatch-Waxman Act apply. In accordance with the Hatch-Waxman Act, such NDAs may be required to include certifications, known as paragraph IV certifications, that certify that any patents listed in the Patent and Exclusivity Information Addendum of the FDA’s publication, Approved Drug Products with Therapeutic Equivalence Evaluations, commonly known as the Orange Book, with respect to any product referenced in the 505(b)(2) application, are invalid, unenforceable or will not be infringed by the manufacture, use or sale of the product that is the subject of the 505(b)(2) NDA.
28
Companies that produce branded reference drugs routinely bring litigation against 505(b)(2) applicants that seek regulatory approval to manufacture and market generic and reformulated forms of their branded products. These companies often allege patent infringement or other violations of intellectual property rights as the basis for filing suit against a 505(b)(2) applicant. Likewise, patent holders may bring patent infringement suits against companies that are currently marketing and selling their approved generic or reformulated products. When a drug, such as GTX-104, has orphan drug exclusivity, the FDA may not approve any other application to market the same drug for the same indication for a period of up to seven years, except in limited circumstances, such as a showing of clinical superiority over the drug product with orphan exclusivity. In the United States, pediatric exclusivity adds six months to any existing exclusivity period.
Our business is subject to extensive regulatory requirements and our drug candidates that obtain regulatory approval will be subject to ongoing and continued regulatory review, which may result in significant expense and limit our ability to commercialize such products.
Even after a drug product is approved, we will remain subject to ongoing FDA and other regulatory requirements governing the labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, import, export, record-keeping and reporting of safety and other post-market information. The holder of an approved NDA is obligated to monitor and report adverse events, and any failure of a drug product to meet the specifications in the NDA. The holder of an approved NDA must also submit new or supplemental applications and obtain FDA approval for certain changes to the approved drug product, product labeling or manufacturing process. Advertising and promotional materials must comply with FDA laws and regulations and are subject to FDA review, in addition to other potentially applicable federal and state laws. In addition, the FDA may impose significant restrictions on the approved indicated uses for which the drug product may be marketed or on the conditions of approval. For example, a product’s approval may contain requirements for potentially costly post-approval studies and surveillance to monitor the safety and efficacy of the drug product, or the imposition of a REMS program.
In addition, the FDA’s regulations, policies, or guidance may change and new or additional statutes or government regulations in the United States and other jurisdictions may be enacted that could prevent or delay regulatory approval of our drug product candidates or further restrict or regulate post-approval activities. We cannot predict the likelihood, nature or extent of adverse government regulation that may arise from pending or future legislation or administrative action, either in the United States or abroad. If we are not able to achieve and maintain regulatory compliance, we may not be permitted to market our drug products and/or drug candidates, which would adversely affect our ability to generate revenue and achieve or maintain profitability.
Our employees, independent contractors, principal investigators, consultants, commercial partners and vendors may engage in misconduct or other improper activities, including non-compliance with regulatory standards and requirements.
We are exposed to the risk that our employees, independent contractors, principal investigators, consultants, commercial partners, and vendors may engage in fraudulent conduct or other illegal activity. Misconduct by these parties could include intentional, reckless and/or negligent conduct that violates (1) the laws of the FDA and similar foreign regulatory bodies, including those laws requiring the reporting of true, complete, and accurate information to such regulatory bodies; (2) healthcare fraud and abuse laws of the United States and similar foreign fraudulent misconduct laws; and (3) laws requiring the reporting of financial information or data accurately. Specifically, the promotion, sales and marketing of health care items and services, as well as certain business arrangements in the healthcare industry are subject to extensive laws designed to prevent misconduct, including fraud, kickbacks, self-dealing and other abusive practices. These laws may restrict or prohibit a wide range of pricing, discounting, marketing, structuring and commission(s), certain customer incentive programs and other business arrangements generally. Activities subject to these laws also involve the improper use of information obtained in the course of patient recruitment for clinical trials. It is not always possible to identify and deter employee and other third-party misconduct. The precautions we take to detect and prevent inappropriate conduct may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to comply with these laws. If any such actions are instituted against us, and we are not successful in defending ourselves, those actions could have a significant impact on our business, including the imposition of civil, criminal and administrative penalties, damages, monetary fines, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings, and curtailment of our operations, any of which could adversely affect our ability to operate our business and our results of operations.
Any relationships with healthcare professionals, principal investigators, consultants, customers (actual and potential) and third-party payors are and will continue to be subject, directly or indirectly, to federal and state healthcare fraud and abuse laws, false claims laws, marketing expenditure tracking and disclosure, or sunshine laws, government price reporting and health information privacy and security laws. If we are unable to comply, or have not fully complied, with such laws, we could face penalties, including, without limitation, civil, criminal, and administrative penalties, damages, monetary fines, disgorgement, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings and curtailment or restructuring of our operations.
Our business operations and activities may be directly or indirectly, subject to various federal, state, and local fraud and abuse laws, including, without limitation, the federal Anti-Kickback Statute and the federal False Claims Act. These laws may impact, among other things, our current activities with principal investigators and research subjects, as well as proposed and future sales, marketing, and education programs. In addition, we may be subject to patient privacy regulation by the federal government, state governments and foreign jurisdictions in which we conduct our business. The laws that may affect our ability to operate include, but are not limited to:
29
In addition, any sales of our drug products or drug candidates, if and once commercialized outside the United States will also likely subject us to foreign equivalents of the healthcare laws mentioned above, among other foreign laws.
If our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to, without limitation, civil, criminal and administrative penalties, damages, monetary fines, disgorgement, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings and curtailment or restructuring of our operations, any of which could adversely affect our ability to operate.
We are required to obtain regulatory approval for each of our drug candidates in each jurisdiction in which we intend to market such products, and the inability to obtain such approvals would limit our ability to realize their full market potential.
In order to market drug products outside of the United States, we must comply with numerous and varying regulatory requirements of other countries regarding safety and efficacy. Clinical trials conducted in one country may not be accepted by regulatory authorities in other countries, and regulatory approval in one country does not mean that regulatory approval will be obtained in any other country. However, the failure to obtain regulatory approval in one jurisdiction may adversely impact our ability to obtain regulatory approval in another jurisdiction. Approval processes vary among countries and can involve additional product testing and validation and additional administrative review periods. Seeking foreign regulatory approval could result in difficulties and costs for us and require additional non-clinical studies or clinical trials which could be costly and time consuming. Regulatory requirements can vary widely from country to country and could delay or prevent the introduction of our drug products in those countries. If we fail to comply with regulatory requirements in international markets or to obtain and maintain required approvals, or if regulatory approval in international markets is delayed, our target market will be reduced and our ability to realize the full market potential of our drug products will be harmed.
Risks Relating to Our Intellectual Property
If we are sued for infringing intellectual property rights of third parties, it will be costly and time consuming, and an unfavorable outcome in that litigation would have a material adverse effect on our business.
Our commercial success also depends upon our ability and the ability of our future collaborators to develop, manufacture, market and sell our drug candidates and to use our proprietary technologies without infringing the proprietary rights of third parties. Numerous U.S. and foreign issued patents and pending patent applications, which are owned by third parties, exist in the fields in which we are developing drug candidates. Because patent applications can take many years to issue, there may be currently pending applications, which may later result in issued patents that our product candidates or proprietary technologies may infringe. Similarly, there may be issued patents relevant to our drug candidates of which we are not aware.
There is a substantial amount of litigation involving patent and other intellectual property rights in the biotechnology and biopharmaceutical industries generally. In particular, the generic drug industry is characterized by frequent litigation between generic drug companies and branded drug companies. If a third-party claims that we infringe its intellectual property rights, we may face a number of issues, including, but not limited to:
We have not conducted an extensive search of patents issued to third parties, and no assurance can be given that third party patents containing claims covering our drug candidates, technology or methods do not exist, have not been filed, or could not be filed or issued. Because of the number of patents issued and patent applications filed in our technical areas or fields, we believe there is a significant risk that third parties may allege they have patent rights encompassing our products, technology, or methods. Other drug candidates that we may in-license or acquire could be subject to similar risks and uncertainties.
30
We may be subject to claims that our employees, consultants, or independent contractors have wrongfully used or disclosed alleged confidential information or trade secrets of their other clients or former employers to us.
As is common in the biotechnology and pharmaceutical industry, certain of our employees were formerly employed by other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Moreover, we engage the services of consultants to assist us in the development of our drug candidates, many of whom were previously employed at or may have previously been or are currently providing consulting services to, other biotechnology or pharmaceutical companies, including our competitors or potential competitors. We may be subject to claims that these employees and consultants or we have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers or their former or current customers. Litigation may be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial costs and be a distraction to management. Any such litigation would be protracted, expensive, and potentially subject to an unfavorable outcome.
Our success depends in part upon our ability to protect our intellectual property for our branded products and drug candidates, such as GTX-104, GTX-102 and GTX-101.
Our commercial success with respect to our drug products and drug candidates, including GTX-104, GTX-102 and GTX-101, depends on obtaining and maintaining patent protection in the United States and in other countries and trade secret protection for our drug candidates, proprietary technologies and their uses. Our ability to protect our drug products from unauthorized or infringing use by third parties depends in substantial part on our ability to obtain and maintain valid and enforceable patents.
Due to evolving legal standards relating to patentability, validity and enforceability of patents covering pharmaceutical inventions and the scope of claims made under these patents, our ability to maintain, obtain and enforce patents is uncertain and involves complex legal and factual questions. The patent positions of pharmaceutical and biotechnology companies can be highly uncertain and involve complex legal and factual questions for which important legal principles remain unresolved. Changes in either the patent laws or in the interpretations of patent laws in the United States and other countries may diminish the value and the scope of our intellectual property. Accordingly, we cannot predict the breadth of claims that may be allowed or enforced in our patents or in third-party patents.
The degree of future protection for our proprietary rights is uncertain. Only limited protection may be available and may not adequately protect our rights or permit us to gain or keep our competitive advantage. For example:
Proprietary trade secrets and unpatented know-how are also very important to our business. Although we have taken steps to protect our trade secrets and unpatented know-how, including entering into confidentiality agreements with third parties, and confidential information and inventions agreements with certain of our employees, consultants, and advisors, third parties may still obtain this information, or we may be unable to protect our rights. Enforcing a claim that a third party illegally obtained and is using our trade secrets or unpatented know-how is expensive and time consuming, and the outcome is unpredictable. In addition, courts outside the United States may be less willing to protect trade secret information. Moreover, our competitors may independently develop equivalent knowledge, methods, and know-how, and we would not be able to prevent their use.
Our drug development strategy relies heavily upon the 505(b)(2) regulatory pathway, which requires us to certify that we do not infringe upon third-party patents covering approved drugs. Such certifications often result in third-party claims of intellectual property infringement, the defense of which will be costly and time consuming, and an unfavorable outcome in any litigation may prevent or delay our development and commercialization efforts which would harm our business.
Litigation or other proceedings to enforce or defend intellectual property rights are often complex in nature, may be very expensive and time-consuming, may divert our management’s attention from other aspects of our business and may result in unfavorable outcomes that could adversely impact our ability to launch and market our drug candidates, or to prevent third parties from competing with our drug products and drug candidates.
In particular, our commercial success depends in large part on our avoiding infringement of the patents and proprietary rights of third parties for existing approved drug products. Because we intend to utilize the 505(b)(2) regulatory pathway for the approval of our drug products and drug candidates, we rely in whole or in part on studies conducted by third parties related to those approved drug products.
Because patent applications can take many years to issue, there may be currently pending or subsequently filed patent applications which may later result in issued patents that may be infringed by our drug products or drug candidates. If any third-party patents were held by a court of competent jurisdiction to cover aspects of our drug candidates, including the formulation, method of use, any method or process involved in the manufacture of any of our drug candidates, any molecules or intermediates formed during such manufacturing process or any other attribute of the final product itself, the holders of any such patents may be able to block our ability to commercialize our drug candidates unless we obtain a license under the applicable patents, or until such patents expire. In either case, such a license may not be available on commercially reasonable terms or at all.
31
Parties making claims against us may request and/or obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our drug candidates on a temporary or permanent basis. Defense of these claims, regardless of their merit, would involve substantial litigation expense and would be a substantial diversion of employee resources from our business. In the event of a successful claim of infringement against us, we may have to pay substantial damages, including treble damages and attorneys’ fees for wilful infringement, obtain one or more licenses from third parties, pay royalties or redesign our infringing products or manufacturing processes, which may be impossible or require substantial time and monetary expenditure. We cannot predict whether any such license would be available at all or whether it would be available on commercially reasonable terms. Furthermore, even in the absence of litigation, we may need to obtain licenses from third parties to advance our research, manufacture clinical trial supplies or allow commercialization of our drug candidates. We may fail to obtain any of these licenses at a reasonable cost or on reasonable terms, if at all. In that event, we would be unable to further develop and commercialize one or more of our drug candidates, which could harm our business significantly. We cannot provide any assurances that third party patents do not exist which might be enforced against our products, resulting in either an injunction prohibiting our sales, or, with respect to our sales, an obligation on our part to pay royalties and/or other forms of compensation to third parties.
If we fail to comply with our obligations in the agreements under which we license rights to technology from third parties, or if the license agreements are terminated for other reasons, we could lose license rights that are important to our business.
We may be a party to a number of technology licenses that are important to our business and expect to enter into additional licenses in the future. Our existing license agreements impose, and we expect that future license agreements will impose, on us, various development, regulatory and/or commercial diligence obligations, payment of milestones and/or royalties and other obligations. Under these agreements, we must rely on our licensor to comply with their obligations under the primary license agreements under which such third party obtained rights in the applicable intellectual property, where we may have no relationship with the original licensor of such rights. If our licensors fail to comply with their obligations under these upstream license agreements, the original third-party licensor may have the right to terminate the original license, which may terminate our sublicense. If this were to occur, we would no longer have rights to the applicable intellectual property unless we are able to secure our own direct license with the owner of the relevant rights, which we may not be able to do at a reasonable cost or on reasonable terms, which may impact our ability to continue to develop and commercialize our drug candidates and companion diagnostic incorporating the relevant intellectual property. If we fail to comply with our obligations under our license agreements, or we are subject to a bankruptcy or insolvency, the licensor may have the right to terminate the license. In the event that any of our important technology licenses were to be terminated by the licensor, we would likely cease further development of the related program or be required to spend significant time and resources to modify the program to not use the rights under the terminated license.
We may be subject to claims that our employees, consultants, or independent contractors have wrongfully used or disclosed confidential information of third parties.
We employ individuals who were previously employed at other biotechnology or pharmaceutical companies. We may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed confidential information of our employees’ former employers or other third parties. We may also be subject to claims that former employers or other third parties have an ownership interest in our patents. Litigation may be necessary to defend against these claims. There is no guarantee of success in defending these claims, and if we are successful, litigation could result in substantial cost and be a distraction to our management and other employees.
We may be subject to claims challenging the inventorship or ownership of our patents and other intellectual property.
We may also be subject to claims that former employees, collaborators or other third parties have an ownership interest in our patents or other intellectual property. We may be subject to ownership disputes in the future arising, for example, from conflicting obligations of consultants or others who are involved in developing our drug candidates and companion diagnostic. Litigation may be necessary to defend against these and other claims challenging inventorship or ownership. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Intellectual property rights do not necessarily address all potential threats to our competitive advantage.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations and may not adequately protect our business or permit us to maintain our competitive advantage. The following examples are illustrative:
Should any of these events occur, they could significantly harm our business, results of operations and prospects.
Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect any of our other future drug candidates.
Numerous recent changes to the patent laws and proposed changes to the rules of the various patent offices around the world may have a significant impact on our ability to protect our technology and enforce our intellectual property rights. These changes may lead to increasing uncertainty with regard to the scope and value of our issued patents and to our ability to obtain patents in the future.
32
Once granted, patents may remain open to opposition, re-examination, post-grant review, inter partes review, nullification derivation and opposition proceedings in court or before patent offices or similar proceedings for a given period after allowance or grant, during which time third parties can raise objections against the initial grant. In the course of any such proceedings, which may continue for a protracted period of time, the patent owner may be compelled to limit the scope of the allowed or granted claims attacked or may lose the allowed or granted claims altogether. Depending on decisions by authorities in various jurisdictions, the laws and regulations governing patents could change in unpredictable ways that may weaken our and our licensors’ ability to obtain new patents or to enforce existing patents we and our licensors or partners may obtain in the future.
We may not be able to protect our intellectual property rights throughout the world.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of some countries, particularly certain developing countries, do not favor the enforcement of patents, trade secrets and other intellectual property protection, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate, and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license.
If our estimates or judgments relating to our critical accounting policies for intangible assets prove to be incorrect, impairment charges could result.
We carry a significant amount of intangible assets on our consolidated balance sheet, associated with acquired in process research and development. In the ordinary course of business, circumstances may arise, including manifestation of any of the risks identified in this section, that could result in recognition that the carrying values of our assets may not be recovered from future operations. Under such circumstances, it is possible we may be required to impair our asset values to the extent that their remaining value after any such impairment can be recovered by our business going forward. Intangible assets with an indefinite useful life are subject to an impairment review at least annually.
Risks Related to Our Dependence on Third Parties
We do not have internal manufacturing capabilities, and if we fail to develop and maintain supply relationships with various third-party manufacturers, we may be unable to develop or commercialize our drug candidates.
Our ability to develop and commercialize our drug candidates depends, in part, on our ability to outsource their manufacturing at a competitive cost, in accordance with regulatory requirements and in sufficient quantities for clinical testing and eventual commercialization. All of our manufacturing is outsourced to third parties, and we do not plan to build manufacturing capabilities.
Our contract manufacturers may encounter manufacturing failures that could delay the clinical development or regulatory approval of our drug candidates, or their commercial production, if approved.
Any performance failure on the part of any of our manufacturers could delay the clinical development or regulatory approval of our drug candidates. Our manufacturers may encounter difficulties involving, among other things, production yields, regulatory compliance, quality control and quality assurance, as well as shortages of qualified personnel. Approval of our drug candidates could be delayed, limited, or denied if the FDA does not approve and maintain the approval of our contract manufacturer’s processes or facilities. Moreover, our contract manufacturers may encounter difficulties that have a negative impact on our operations and business. Our manufacturers may encounter difficulties with the manufacturing processes required to manufacture commercial quantities of our drug candidates or the quantities needed for our pre-clinical studies or clinical trials. Such difficulties could result in delays in our pre-clinical studies, clinical trials, and regulatory submissions, in the commercialization of our drug candidates. Further, development of large-scale manufacturing processes may require additional validation studies, which the FDA must review and approve. If any of our manufacturers fail to deliver the required commercial quantities or quantities needed for our pre-clinical studies and clinical trials on a timely basis and upon terms that we find acceptable, we may be unable to meet demand for any of our drug candidates that are approved and could lose potential revenue.
Certain changes in the manufacturing process or procedure, including a change in the location where the drug candidate is manufactured or a change of a third-party manufacturer, generally require prior FDA, or foreign regulatory authority, review and/or approval of the manufacturing process and procedures in accordance with cGMP. We may need to conduct additional pre-clinical studies and clinical trials to support approval of such changes. This review may be costly and time-consuming and could delay or prevent the launch of a drug candidate.
We rely on third parties to conduct our preclinical studies and clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize our drug candidates and our business could be substantially harmed.
We have relied upon and plan to continue to rely upon third party CROs to monitor and manage data for our preclinical and clinical programs. We rely on these parties for execution of our preclinical studies and clinical trials, and control only certain aspects of their activities. Nevertheless, we are responsible for ensuring that each of our trials is conducted in accordance with the applicable protocol, legal, regulatory, and scientific standards and our reliance on the CROs does not relieve us of our regulatory responsibilities. We and our CROs are required to comply with FDA laws and regulations regarding current good clinical practice (“GCP”), which are also required by the Competent Authorities of the Member States of the European Economic Area and comparable foreign regulatory authorities in the form of International Conference on Harmonization, guidelines for all of our drug candidates in clinical development. Regulatory authorities enforce GCP through periodic inspections of trial sponsors, principal investigators, and trial sites. If we or any of our CROs fail to comply with applicable GCP, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials comply with GCP regulations. In addition, our clinical trials must be conducted with product produced under cGMP regulations. While we have agreements governing activities of our CROs, we have limited influence over their actual performance. In addition, portions of the clinical trials for our drug candidates are expected to be conducted outside of the United States, which will make it more difficult for us to monitor CROs and perform visits of our clinical trial sites and will force us to rely heavily on CROs to ensure the proper and timely conduct of our clinical trials and compliance with applicable regulations, including GCP. Failure to comply with applicable regulations in the conduct of the clinical trials for our drug candidates may require us to repeat clinical trials, which would delay the regulatory approval process.
33
We rely on third parties to manufacture commercial and clinical supplies of our drug candidates, and we intend to rely on third parties to manufacture commercial supplies of any approved drug products. The commercialization of any of our drug products could be stopped, delayed, or made less profitable if those third parties fail to provide us with sufficient quantities of active pharmaceutical ingredients, excipients, or drug products, or fail to do so at acceptable quality levels or prices or fail to maintain or achieve satisfactory regulatory compliance.
We do not own any manufacturing facilities, and we do not currently, and do not expect in the future, to independently conduct any aspects of our product manufacturing and testing, or other activities related to the clinical development and commercialization of our drug candidates. We currently rely, and expect to continue to rely, on third parties with respect to these items, and control only certain aspects of their activities.
Any of these third parties may terminate their engagements with us at any time. If we need to enter into alternative arrangements, it could delay our drug candidate development and commercialization activities. Our reliance on these third parties reduces our control over these activities but does not relieve us of our responsibility to ensure compliance with all required legal, regulatory, and scientific standards and any applicable trial protocols. If these third parties do not successfully carry out their contractual duties, meet expected deadlines or conduct our studies in accordance with regulatory requirements or our stated study plans and protocols, we will not be able to complete, or may be delayed in completing, clinical trials required to support future regulatory submissions and approval of our drug candidates.
More generally, manufacturers of pharmaceutical products often encounter difficulties in production, particularly in scaling up and validating initial production. These problems include difficulties with production costs and yields, quality control, including stability of the product, quality assurance testing, shortages of qualified personnel, as well as compliance with strictly enforced federal, state, and foreign regulations. Additionally, our manufacturers may experience manufacturing difficulties due to resource constraints or as a result of labor disputes or unstable political environments. If our manufacturers were to encounter any of these difficulties, or otherwise fail to comply with their contractual obligations, our ability to make product candidates available for clinical trials and development purposes or to commercialize any of our product candidates in the United States would be jeopardized. Any delay or interruption in our ability to meet commercial demand may result in the loss of potential revenues and could adversely affect our ability to gain market acceptance for approved products. In addition, any delay or interruption in the supply of clinical trial supplies could delay the completion of clinical trials, increase the costs associated with maintaining clinical trial programs and, depending upon the period of delay, require us to commence new clinical trials at additional expense or terminate clinical trials completely. Additionally, if supply from one approved manufacturer is interrupted, there could be a significant disruption in commercial supply. Regulatory agencies may also require additional studies if a new manufacturer is relied upon for commercial production. Switching manufacturers may involve substantial costs and is likely to result in a delay in our desired clinical and commercial timelines.
The design, development, manufacture, supply, and distribution of our drug candidates is highly regulated and technically complex.
All entities involved in the preparation of therapeutics for clinical trials or commercial sale, including our existing contract manufacturers for our drug candidates, are subject to extensive regulation. Components of a finished therapeutic product approved for commercial sale or used in late-stage clinical trials must be manufactured in accordance with cGMP and equivalent foreign standards. These regulations govern manufacturing processes and procedures (including record-keeping) and the implementation and operation of quality systems to control and assure the quality of investigational products and products approved for sale. Poor control of production processes can lead to the introduction of adventitious agents or other contaminants, or to inadvertent changes in the properties or stability of our drug candidates that may not be detectable in final product testing. The development, manufacture, supply, and distribution of our drug candidates is highly regulated and technically complex. We, along with our third-party providers, must comply with all applicable regulatory requirements of the FDA and foreign authorities.
Regulatory authorities also may, at any time following approval of a drug product for sale, audit our manufacturing facilities or those of our third-party contractors. If any such inspection or audit identifies a failure to comply with applicable regulations or if a violation of our product specifications or applicable regulations occurs independent of such an inspection or audit, we or the relevant regulatory authority may require remedial measures that may be costly and/or time-consuming for us or a third party to implement and that may include the temporary or permanent suspension of a clinical trial or commercial sales or the temporary or permanent closure of a facility. Any such remedial measures imposed upon us or third parties with whom we contract could materially harm our business. If we or any of our third-party manufacturers fail to maintain regulatory compliance, the FDA can impose regulatory sanctions including, among other things, refusal to approve a pending application for a new drug product or biological product or revocation of a pre-existing approval. As a result, our business, financial condition, and results of operations may be materially harmed.
We may not be successful in establishing development and commercialization collaborations which could adversely affect, and potentially prohibit, our ability to develop our drug candidates.
Because developing pharmaceutical products, conducting clinical trials, obtaining regulatory approval, establishing manufacturing capabilities and marketing approved products are expensive, we are exploring collaborations with third parties outside of the United States that have more resources and experience. In situations where we enter into a development and commercial collaboration arrangement for a drug candidate, we may also seek to establish additional collaborations for development and commercialization in territories outside of those addressed by the first collaboration arrangement for such drug candidate. There are a limited number of potential partners, and we expect to face competition in seeking appropriate partners. If we are unable to enter into any development and commercial collaborations and/or sales and marketing arrangements on acceptable terms, if at all, we may be unable to successfully develop and seek regulatory approval for our drug candidates and/or effectively market and sell future approved drug products, if any, in all of the territories outside of the United States where it may otherwise be valuable to do so.
We may not be successful in maintaining development and commercialization collaborations, and any partner may not devote sufficient resources to the development or commercialization of our drug candidates or may otherwise fail in development or commercialization efforts, which could adversely affect our ability to develop certain of our drug candidates and our financial condition and operating results.
Even if we are able to establish collaboration arrangements, any such collaboration may not ultimately be successful, which could have a negative impact on our business, results of operations, financial condition and prospects. If we partner with a third party for development and commercialization of a drug candidate, we can expect to relinquish some or all of the control over the future success of that drug candidate to the third party. It is possible that a partner may not devote sufficient resources to the development or commercialization of our drug candidate or may otherwise fail in development or commercialization efforts, in which event the development and commercialization of such drug candidate could be delayed or terminated, and our business could be substantially harmed. In addition, the terms of any collaboration or other arrangement that we establish may not prove to be favorable to us or may not be perceived as favorable, which may negatively impact the trading price of our common shares. In some cases, we may be responsible for continuing development of a product candidate or research program under a collaboration, and the payment we receive from our partner may be insufficient to cover the cost of this development. Moreover, collaborations and sales and marketing arrangements are complex and time consuming to negotiate, document and implement, and they may require substantial resources to maintain.
34
We are subject to a number of additional risks associated with our dependence on collaborations with third parties, the occurrence of which could cause our collaboration arrangements to fail. Conflicts may arise between us and our partners, such as conflicts concerning the interpretation of clinical data, the achievement of milestones, the interpretation of financial provisions or the ownership of intellectual property developed during the collaboration. If any such conflicts arise, a partner could act in its own self-interest, which may be adverse to our interests. Any such disagreement between us and a partner could result in one or more of the following, each of which could delay or prevent the development or commercialization of our drug candidates and harm our business:
Risks related to Tax
There is a significant risk that we may be classified as a PFIC for U.S. federal income tax purposes.
Current or potential investors in our common shares who are U.S. Holders (as defined below) should be aware that, based on our most recent financial statements and projections and given uncertainty regarding the composition of our future income and assets, there is a significant risk that we may have been classified as a "passive foreign investment company" or "PFIC" for the 2021 taxable year and may be classified as a PFIC for our current taxable year and possibly subsequent years. Each current or potential investor who is a U.S. Holder should consult his, her or its own tax advisor regarding the U.S. federal, state and local, and non-U.S. tax consequences of the acquisition, ownership, and disposition of our common shares, the U.S. federal tax consequences of the PFIC rules, and the availability of any election that may be available to the holder to mitigate adverse U.S. federal income tax consequences of holding shares of a PFIC.
The rules governing PFICs can have adverse tax effects on U.S. shareholders, which effects may be mitigated by making certain elections for U.S. federal income tax purposes, which elections may or may not be available. If we are a PFIC in any year, a U.S. shareholder in such year will be required to file an annual information return with the IRS on IRS Form 8621 regarding distributions received on their common shares, any gain realized on disposition of such common shares and any other information required by such form. Additionally, if we are classified as a PFIC in any taxable year with respect to which a U.S. shareholder owns common shares, we generally will continue to be treated as a PFIC with respect to such U.S. shareholder in all succeeding taxable years, regardless of whether we continue to meet the tests described above, unless the U.S. shareholder makes a “deemed sale election.”
We may not be able to use our net operating loss carry forwards to offset future taxable income for Canadian or U.S. federal income tax purposes.
At March 31, 2022, Acasti Pharma U.S. had net operating loss carry forwards (“NOLs”) for U.S. federal income tax purposes of approximately $12 million, which have no expiry.
Acasti Pharma U.S. underwent an “ownership change” within the meaning of Section 382 of the Code as a result of the merger, and therefore Acasti Pharma U.S. may become subject to an annual limit on the amount of NOLs that may be used to offset future taxable income of Acasti Pharma U.S. for U.S. federal income tax purposes. Such annual limit is generally equal to the product of (i) the total value of the loss company’s (in this case, Acasti Pharma U.S.) outstanding equity immediately prior to an “ownership change” (subject to certain adjustments); and (ii) the applicable federal long-term tax-exempt interest rate for the month that includes the “ownership change”.
At March 31, 2022, we had NOLs for Canadian federal income tax purposes of approximately $119.4 million, which expire at various dates through 2042. The extent to which we can utilize any or all of our NOLs will depend on many factors, including the jurisdiction applicable to any of our future taxable revenue.
Our ability to use NOLs will also depend on the amount of taxable income generated in future periods. The NOLs may expire before we can generate sufficient taxable income to use the NOLs.
The IRS may not agree that we should be treated as a foreign corporation for U.S. federal tax purposes.
Although we are incorporated in Quebec, Canada, the Internal Revenue Service (the "IRS") may assert that we should be treated as a U.S. corporation (and, therefore, a U.S. tax resident) for U.S. federal tax purposes pursuant to Section 7874 of the U.S. Internal Revenue Code of 1986, as amended (the "Code"). For U.S. federal tax purposes, a corporation generally is considered a tax resident in the jurisdiction of its organization or incorporation. Because we are an entity incorporated in Canada, we would generally be classified as a foreign corporation (and, therefore, not a U.S. tax resident) for U.S. federal tax purposes. Section 7874 of the Code provides an exception under which a foreign corporation may, in certain circumstances, be treated as a U.S. corporation for U.S. federal tax purposes.
Under Section 7874, if (1) former Grace shareholders owned (within the meaning of Section 7874) 80% or more (by vote or value) of our ordinary shares after the merger by reason of holding Grace common stock (such ownership percentage, the "Section 7874 ownership percentage"), and (2) our "expanded affiliated group" did not have "substantial business activities" in Canada ("the substantial business activities test"), we will be treated as a U.S. corporation for U.S. federal tax purposes. If the Section 7874 ownership percentage of the former Grace shareholders after the merger was less than 80% but greater than or equal to 60%, and the substantial business activities test was not met, we and our U.S. affiliates may, in some circumstances, be subject to certain adverse U.S. federal income tax provisions (which, among other things, could limit their ability to utilize certain U.S. tax attributes such as NOLs to offset U.S. taxable income or gain resulting from certain transactions). The application of these rules could result in significant additional U.S. tax liability and limit our ability to restructure or access cash earned by certain of our non-U.S. subsidiaries, in each case, without incurring substantial U.S. tax liabilities.
Based on the terms of the merger, the rules for determining share ownership under Section 7874 and certain factual assumptions, we believe that former Grace shareholders owned (within the meaning of Section 7874) less than 60% (by both vote and value) of our ordinary shares after the merger by reason of holding shares of Grace common stock. Therefore, under current law, we believe that we should not be treated as a U.S. corporation for U.S. federal tax purposes and that Section 7874 should otherwise not apply to us or our affiliates as a result of the merger with Grace.
35
Risks Relating to Our Common Shares
We do not expect to pay any cash dividends for the foreseeable future.
The continued operation and expansion of our business will require substantial funding. Accordingly, we do not anticipate that we will pay any cash dividends on our common shares for the foreseeable future. Any determination to pay dividends in the future will be at the discretion of our board of directors and will depend upon our results of operations, financial condition, contractual restrictions, restrictions imposed by applicable law and other factors our board of directors deems relevant.
The price of our common shares may be volatile.
Market prices for securities of pharmaceutical companies can fluctuate significantly. Factors such as the announcement to the public or in various scientific or industry forums of technological innovations; new commercial products; patents or exclusive rights obtained by us or others; disputes or other developments relating to proprietary rights, including patents, litigation matters and our ability to obtain patent protection for our technologies; the commencement, enrollment or announcement of results of clinical trials we conduct, or changes in the development status of our drug candidates; results or delays of pre-clinical and clinical studies by us or others; any delay in our regulatory filings for our drug candidates and any adverse development or perceived adverse development with respect to the applicable regulatory authority’s review of such filings; a change of regulations; additions or departures of key scientific or management personnel; overall performance of the equity markets; general political and economic conditions; publications; failure to meet the estimates and projections of the investment community or that we may otherwise provide to the public; research reports or positive or negative recommendations or withdrawal of research coverage by securities analysts; actual or anticipated variations in quarterly operating results; announcements of significant acquisitions, strategic partnerships, joint ventures or capital commitments by us or our competitors; public concerns over the risks of pharmaceutical products and dietary supplements; unanticipated serious safety concerns related to the use of our drug candidates or drug products; our access to financial resources, future sales of securities by us or our shareholders; and many other factors, many of which are beyond our control, could have considerable effects on the price of our common shares. The price of our common shares has fluctuated significantly in the past and there can be no assurance that the market price of our common shares will not experience significant fluctuations in the future.
In addition, securities of pharmaceutical companies often experience extreme price and volume fluctuations that are unrelated or disproportionate to the operating performance of those companies. Broad market and industry factors may negatively affect the market price of our common shares, regardless of our actual operating performance. In the past, securities class action litigation has often been instituted against pharmaceutical companies following periods of volatility in the market price of their securities. This type of litigation, if instituted against us, could result in substantial costs and a diversion of management’s attention and resources, which would harm our business, operating results or financial condition.
Raising additional capital may cause dilution to our existing shareholders, restrict our operations, or require us to relinquish rights to our technologies or drug candidates.
We will need to raise additional capital in the future in order to fully execute on our business plan. We may seek additional capital through a combination of public and private equity offerings, debt financings, and non-dilutive strategic partnerships and alliances and licensing arrangements. To the extent that we raise additional capital through the sale of equity or convertible debt securities, the ownership interests of our shareholders will be diluted, and the terms may include liquidation or other preferences that adversely affect the rights of our shareholders. We have in place an “at-the-market” sales agreement where we may issue and sell from time-to-time common shares having an aggregate offering price of up to $75,000,000. The incurrence of indebtedness by us would result in increased fixed payment obligations and could involve certain restrictive covenants, such as limitations on our ability to incur additional debt, limitations on our ability to acquire or license intellectual property rights and other operating restrictions that could adversely impact our ability to conduct our business. If we raise additional funds through strategic partnerships and alliances and licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies or drug candidates, or grant licenses on terms unfavorable to us.
The market price of our common shares could decline if our operating results fall below the expectations of investors or fluctuate.
Our net losses and expenses may fluctuate significantly and any failure to meet financial or clinical expectations may disappoint securities analysts or investors and result in a decline in the price of our common shares. Our net losses and expenses have fluctuated in the past and are likely to do so in the future. The market price of our common shares has fluctuated significantly in the past and may continue to do so. Some of the factors that could cause the market price for our common shares to fluctuate include the following:
36
If our quarterly operating results fall below the expectations of investors or securities analysts, the market price of our common shares could decline substantially. Furthermore, any quarterly fluctuations in our operating results may, in turn, cause the market price of our common shares to fluctuate substantially. We believe that quarterly comparisons of our financial results for a company at our stage of operation are not necessarily meaningful and should not be relied upon as an indication of our future performance.
There can be no assurance that an active market for our common shares will be sustained.
There can be no assurance that an active market for our common shares will be sustained. Holders of common shares may be unable to sell their investments on satisfactory terms. As a result of any risk factor discussed herein, the market price of our common shares at any given point in time may not accurately reflect our long-term value. Furthermore, responding to these risk factors could result in substantial costs and divert management’s attention and resources. Substantial and potentially permanent declines in the value of our common shares may adversely affect the liquidity of the market for our common shares.
Other factors unrelated to our performance that may have an effect on the price and liquidity of our common shares include positive or negative industry or competitor news; extent of analyst coverage; lessening in trading volume and general market interest in our common shares; the size of our public float; our access to funding; and any event resulting in a delisting of our common shares.
If we fail to meet applicable listing requirements, the NASDAQ Stock Market or the TSX Venture Exchange (“TSXV”) may delist our common shares from trading, in which case the liquidity and market price of our common shares could decline.
Our common shares are currently listed on the NASDAQ Stock Market and the TSXV, but we cannot assure you that our securities will continue to be listed on the NASDAQ Stock Market and the TSXV in the future. In the past, we have received notices from the NASDAQ Stock Market that we have not been in compliance with its continued listing standards, and we have taken responsive actions and regained compliance.
If we fail to comply with listing standards and the NASDAQ Stock Market or TSXV delists our common shares, we and our shareholders could face significant material adverse consequences, including:
We may pursue opportunities or transactions that adversely affect our business and financial condition.
Our management, in the ordinary course of our business, regularly explores potential strategic opportunities and transactions. These opportunities and transactions may include strategic joint venture relationships, significant debt or equity investments in us by third parties, the acquisition or disposition of material assets, the licensing, acquisition or disposition of material intellectual property, the development of new drug candidates, the sale of our common shares and other similar opportunities and transactions. The public announcement of any of these or similar strategic opportunities or transactions might have a significant effect on the price of our common shares. Our policy is to not publicly disclose the pursuit of a potential strategic opportunity or transaction unless we are required to do so by applicable law, including applicable securities laws relating to periodic disclosure obligations. There can be no assurance that investors who buy or sell common shares are doing so at a time when we are not pursuing a particular strategic opportunity or transaction that, when announced, would have a significant effect on the price of our common shares.
In addition, any such future corporate development may be accompanied by certain risks, including exposure to unknown liabilities of the strategic opportunities and transactions, higher than anticipated transaction costs and expenses, the difficulty and expense of integrating operations and personnel of any acquired companies, disruption of our ongoing business, diversion of management’s time and attention, and possible dilution to shareholders. We may not be able to successfully overcome these risks and other problems associated with any future acquisitions and this may adversely affect our business and financial condition.
We are a “smaller reporting company” under the SEC’s disclosure rules and have elected to comply with the reduced disclosure requirements applicable to smaller reporting companies.
We are a “smaller reporting company” under the SEC’s disclosure rules, meaning that we have either:
37
As a smaller reporting company, we are permitted to comply with scaled-back disclosure obligations in our SEC filings compared to other issuers, including with respect to disclosure obligations regarding executive compensation in our periodic reports and proxy statements. We have elected to adopt the accommodations available to smaller reporting companies. Until we cease to be a smaller reporting company, the scaled-back disclosure in our SEC filings will result in less information about our company being available than for other public companies that are not smaller reporting companies.
If investors consider our common shares less attractive as a result of our election to use the scaled-back disclosure permitted for smaller reporting companies, there may be a less active trading market for our common shares and our share price may be more volatile.
As a non-accelerated filer, we are not required to comply with the auditor attestation requirements of the Sarbanes-Oxley Act.
We are a non-accelerated filer under the Exchange Act and we are not required to comply with the auditor attestation requirements of Section 404(b) of the Sarbanes-Oxley Act of 2002. Therefore, our internal controls over financial reporting will not receive the level of review provided by the process relating to the auditor attestation included in annual reports of issuers that are subject to the auditor attestation requirements. In addition, we cannot predict if investors will find our common shares less attractive because we are not required to comply with the auditor attestation requirements. If some investors find our common shares less attractive as a result, there may be a less active trading market for our common shares and the trading price for our common shares may be negatively affected.
We are a Québec incorporated company headquartered in Canada, and U.S. investors may be unable to enforce certain judgments against us.
We are a company existing under the Business Corporations Act (Québec). Some of our directors and officers are residents of Canada, and certain of our assets are located outside the United States. As a result, it may be difficult to effect service within the United States upon us or upon some of our directors and officers. Execution by U.S. courts of any judgment obtained against us or any of our directors or officers in U.S. courts may be limited to assets located in the United States. It may also be difficult for holders of our securities who reside in the United States to realize in the United States upon judgments of U.S. courts predicated upon civil liability of us and our directors and executive officers under the U.S. federal securities laws. There may be doubt as to the enforceability in Canada against non-U.S. entities or their controlling persons, directors and officers who are not residents of the United States, in original actions or in actions for enforcement of judgments of U.S. courts, of liabilities predicated solely upon U.S. federal or state securities laws.
38
Item 1B. Unresolved Staff Comments
Not applicable.
Item 2. Properties
Our head office and operations are located at 3009 boul. de la Concorde East, Suite 102, Laval, Québec, Canada H7E 2B5 and our research and development and quality control laboratories are located at Espace Lab, 2650 Maximilien-Chagnon, Sherbrooke, Québec, Canada, J1E 0M8 and 685 US Highway One, North Brunswick, NJ 08902. We currently lease our office and laboratory space. We do not own our own manufacturing facility to produce CaPre; however, we do own the proprietary equipment for producing the related active pharmaceutical ingredient, or API, and drug product.
Item 3. Legal Proceedings
In the ordinary course of business, we are at times subject to various legal proceedings and disputes, including the proceedings specifically discussed below. We assess our liabilities and contingencies in connection with outstanding legal proceedings utilizing the latest information available. Where it is probable that we will incur a loss and the amount of the loss can be reasonably estimated, we record a liability in our consolidated financial statements. These legal reserves may be increased or decreased to reflect any relevant developments on a quarterly basis. Where a loss is not probable or the amount of loss is not estimable, we do not accrue legal reserves. While the outcome of legal proceedings is inherently uncertain, based on information currently available and available insurance coverage, our management believes that it has established appropriate legal reserves. Any incremental liabilities arising from pending legal proceedings are not expected to have a material adverse effect on our financial position, results of operations, or cash flows. However, it is possible that the ultimate resolution of these matters, if unfavorable, may be material to our financial position, results of operations, or cash flows.
Litigation Related to the Merger
In connection with the Grace merger, four stockholder lawsuits have been filed:
The Complaints generally allege that our public disclosures pertaining to the Grace merger omitted material facts in purported violation of Section 14(a) of the Exchange Act and Rule 14a-9 promulgated thereunder, and further that members of our Board of Directors are liable for those purported omissions under Section 20(a) of the Exchange Act. The relief sought in the Complaints includes, among other things to enjoin the consummation of the merger pending disclosure of sufficient information, to award damages purportedly caused by the alleged omissions, and to award plaintiffs’ attorneys’ fees and other costs.
The Dawson and Weir Complaints have been voluntarily dismissed without prejudice. The Bisel and Castaldo Complaints have been consolidated. The plaintiffs amended their Complaint in the consolidated action on October 1, 2021, to assert their claims on a class wide basis. The court appointed Plaintiff Castaldo as Lead Plaintiff for the putative class in the consolidated action. Castaldo filed an amended Complaint by February 4, 2022. Acasti filed a motion to dismiss on February 25, 2022.
It is possible that additional lawsuits asserting similar claims could be filed. We strongly believe the allegations in the Complaints are frivolous and without merit, and are vigorously defending against them.
Item 4. Mine Safety Disclosures
Not applicable.
39
PART II
Item 5. Market for Registrant’s Common Equity, Related Shareholder Matters and Issuer Purchases of Equity Securities Market Information
Our common shares are traded on The Nasdaq Capital Market and the TSX Venture Exchange under the symbol “ACST.”
Holders
As of June 21, 2022, there were 39 holders of record of our common shares. The actual number of our shareholders is greater than this number of record holders because most of our shareholders are beneficial owners whose shares are held in street name by brokers and other nominees.
Dividends
We do not anticipate paying any cash dividend on our common shares in the foreseeable future. We presently intend to retain any future earnings to finance the expansion and growth of our business. Any future determination to pay dividends will be at the discretion of our board of directors and will depend on our financial condition, results of operations, capital requirements and other factors the board of directors deems relevant. In addition, the terms of any future debt or credit facility may preclude us from paying dividends.
Taxation
The following is a summary of certain U.S. federal income tax considerations arising from and relating to the acquisition, ownership, and disposition of our common shares to a U.S. Holder (as defined below) as capital assets.
This summary provides only general information and does not purport to be a complete analysis or listing of all potential U.S. federal income tax consequences that may apply to a U.S. Holder as a result of the acquisition, ownership, and disposition of our common shares. In addition, this summary does not take into account the individual facts and circumstances of any particular U.S. Holder that may affect the U.S. federal income tax consequences applicable to that U.S. Holder. Accordingly, this summary is not intended to be, and should not be construed as, legal or U.S. federal income tax advice with respect to any U.S. Holder. Each U.S. Holder should consult its own tax advisor regarding the U.S. federal, state and local, and non-U.S. tax consequences arising from or relating to the acquisition, ownership, and disposition of our common shares.
No legal opinion from U.S. legal counsel or ruling from the IRS, has been requested, or will be obtained, regarding the U.S. federal income tax consequences to U.S. Holders of the acquisition, ownership, and disposition of our common shares. This summary is not binding on the IRS, and the IRS is not precluded from taking a position that is different from, and contrary to, the positions taken in this summary. In addition, because the authorities on which this summary is based are subject to various interpretations, the IRS and the U.S. courts could disagree with one or more of the positions taken in this summary.
Scope of this Disclosure
Authorities
This summary is based on the Code, U.S. Treasury Regulations promulgated thereunder (whether final, temporary or proposed), published IRS rulings, judicial decisions, published administrative positions of the IRS, and the Convention between Canada and the United States of America with Respect to Taxes on Income and on Capital, signed September 26, 1980, as amended (the Canada-U.S. Tax Treaty), in each case, as in effect as of the date of this report. Any of the authorities on which this summary is based could be changed in a material and adverse manner at any time, and any such change could be applied on a retroactive basis. Unless otherwise discussed, this summary does not discuss the potential effects, whether adverse or beneficial, of any proposed legislation.
U.S. Holders
For purposes of this summary, a “U.S. Holder” is a beneficial owner of common shares that, for U.S. federal income tax purposes, is (a) an individual who is a citizen or resident of the United States, (b) a corporation, or other entity classified as a corporation for U.S. federal income tax purposes, that is created or organized in or under the laws of the U.S., any state in the United States or the District of Columbia, (c) an estate if the income of such estate is subject to U.S. federal income tax regardless of the source of such income, or (d) a trust if (i) such trust has validly elected to be treated as a U.S. person for U.S. federal income tax purposes or (ii) a U.S. court is able to exercise primary supervision over the administration of such trust and one or more U.S. persons have the authority to control all substantial decisions of such trust.
U.S. Holders Subject to Special U.S. Federal Income Tax Rules Not Addressed
This summary does not address the U.S. federal income tax consequences applicable to U.S. Holders that are subject to special provisions under the Code, including, but not limited to, the following U.S. Holders: (a) U.S. Holders that are tax-exempt organizations, qualified retirement plans, individual retirement accounts, or other tax deferred accounts; (b) U.S. Holders that are financial institutions, insurance companies, real estate investment trusts, or regulated investment companies; (c) U.S. Holders that are dealers in securities or currencies or U.S. Holders that are traders in securities that elect to apply a mark-to-market accounting method; (d) U.S. Holders that have a “functional currency” other than the U.S. dollar; (e) U.S. Holders subject to the alternative minimum tax provisions of the Code; (f) U.S. Holders that own common shares as part of a straddle, hedging transaction, conversion transaction, integrated transaction, constructive sale, or other arrangement involving more than one position; (g) U.S. Holders that acquired common shares through the exercise of employee stock options or otherwise as compensation for services; (h) U.S. Holders that hold common shares other than as a capital asset within the meaning of Section 1221 of the Code; (i) U.S. Holders that beneficially own (directly, indirectly or by attribution) 10% or more of our equity securities (by vote or value); and (j) U.S. expatriates. U.S. Holders that are subject to special provisions under the Code, including U.S. Holders described above, should consult their own tax advisor regarding the U.S. federal, U.S. federal alternative minimum, U.S. federal estate and gift, U.S. state and local, and non-U.S. tax consequences arising from and relating to the acquisition, ownership, and disposition of the common shares.
If an entity or arrangement that is classified as a partnership for U.S. federal income tax purposes holds common shares, the U.S. federal income tax consequences to that partnership and the partners of that partnership generally will depend on the activities of the partnership and the status of the partners. Partners of entities that are classified as partnerships for U.S. federal income tax purposes should consult their own tax advisors regarding the U.S. federal income tax consequences arising from and relating to the acquisition, ownership and disposition of the common shares.
Tax Consequences Other than U.S. Federal Income Tax Consequences Not Addressed
This summary does not address the U.S. estate and gift, alternative minimum, state, local or non-U.S. tax consequences to U.S. Holders of the acquisition, ownership, and disposition of our common shares. Each U.S. Holder should consult its own tax advisor regarding the U.S. estate and gift, alternative minimum, state, local and non-U.S. tax consequences arising from and relating to the acquisition, ownership, and disposition of our common shares.
40
U.S. Federal Income Tax Considerations of the Acquisition, Ownership, and Disposition of Common Shares
Distributions on Common Shares
Subject to the discussion under “—Passive Foreign Investment Company Rules” below, a U.S. Holder that receives a distribution, including a constructive distribution or a taxable stock distribution, with respect to the common shares generally will be required to include the amount of that distribution in gross income as a dividend (without reduction for any Canadian income tax withheld from such distribution) to the extent of our current or accumulated “earnings and profits” (as computed for U.S. federal income tax purposes). To the extent that a distribution exceeds our current and accumulated “earnings and profits”, the excess amount will be treated (a) first, as a tax-free return of capital to the extent of a U.S. Holder’s adjusted tax basis in the common shares with respect to which the distribution is made (resulting in a corresponding reduction in the tax basis of those common shares) and, (b) thereafter, as gain from the sale or exchange of those common shares (see the more detailed discussion at “—Disposition of Common Shares” below). We do not intend to calculate our current or accumulated earnings and profits for U.S. federal income tax purposes and, therefore, will not be able to provide U.S. Holders with that information. U.S. Holders should therefore assume that any distribution by us with respect to our common shares will constitute a dividend. However, U.S. Holders should consult their own tax advisors regarding whether distributions from us should be treated as dividends for U.S. federal income tax purposes. Dividends paid on our common shares generally will not be eligible for the “dividends received deduction” allowed to corporations under the Code with respect to dividends received from U.S. corporations.
A dividend paid by us generally will be taxed at the preferential tax rates applicable to long-term capital gains if, among other requirements, (a) we are a “qualified foreign corporation” (as defined below), (b) the U.S. Holder receiving the dividend is an individual, estate, or trust, and (c) the dividend is paid on common shares that have been held by the U.S. Holder for at least 61 days during the 121-day period beginning 60 days before the “ex-dividend date” (i.e., the first date that a purchaser of the common shares will not be entitled to receive the dividend).
For purposes of the rules described in the preceding paragraph, we generally will be a “qualified foreign corporation”, or a QFC, if (a) we are eligible for the benefits of the Canada-U.S. Tax Treaty, or (b) our common shares are readily tradable on an established securities market in the United States, within the meaning provided in the Code. However, even if we satisfy one or more of the requirements, we will not be treated as a QFC if we are classified as a PFIC (as discussed below) for the taxable year during which we pay the applicable dividend or for the preceding taxable year. The dividend rules are complex, and each U.S. Holder should consult its own tax advisor regarding the application of those rules to them in their particular circumstances. Even if we satisfy one or more of the requirements, as noted below. Thus, there can be no assurance that we will qualify as a QFC.
Disposition of Common Shares
Subject to the discussion under “—Passive Foreign Investment Company Rules” below, a U.S. Holder will recognize gain or loss on the sale or other taxable disposition of common shares (that is treated as a sale or exchange for U.S. federal income tax purposes) equal to the difference, if any, between (a) the U.S. dollar value of the amount realized on the date of the sale or disposition and (b) the U.S. Holder’s adjusted tax basis (determined in U.S. dollars) in the common shares sold or otherwise disposed of. Any such gain or loss generally will be capital gain or loss, which will be long-term capital gain or loss if the common shares are held for more than one year. A U.S. Holder's initial tax basis in the common shares generally will equal the U.S. dollar cost of such common shares. Each U.S. Holder should consult its own tax advisor as to the tax treatment of dispositions of common shares in exchange for Canadian dollars.
Preferential tax rates apply to long-term capital gains of a U.S. Holder that is an individual, estate, or trust. There are currently no preferential tax rates for long-term capital gains of a U.S. Holder that is a corporation. Deductions for capital losses are subject to complex limitations.
Passive Foreign Investment Company Rules
If we are or become a PFIC, the preceding sections of this summary may not describe the U.S. federal income tax consequences to U.S. Holders of the acquisition, ownership, and disposition of our common shares.
Passive Foreign Investment Company Status.
Special, generally unfavorable, rules apply to the ownership and disposition of the stock of a PFIC. For U.S. federal income tax purposes, a non-U.S. corporation is classified as a PFIC if:
Passive income generally includes the following types of income:
In determining whether we are a PFIC, we will be required to take into account a pro rata portion of the income and assets of each corporation in which we own, directly or indirectly, at least 25% by value.
As described above, PFIC status of a non-U.S. corporation depends on the relative values of certain categories of assets and the relative amount of certain kinds of income for a taxable year. Therefore, our status as a PFIC for any given taxable year depends upon the financial results for such year and upon relative valuations, which are subject to change and beyond our ability to predict or control. Based on our most recent financial statements and projections and given uncertainty regarding the composition of our future income and assets, there is a significant risk that we may have been classified as a PFIC for the taxable year that ended on March 31, 2022 and may be classified as a PFIC for our current taxable year and possibly subsequent years. However, PFIC status is fundamentally factual in nature, depends on the application of complex U.S. federal income tax rules (which are subject to differing interpretations), generally cannot be determined until the close of the taxable year in question and is determined annually. Accordingly, there can be no assurance that we will not be a PFIC in our current taxable year or subsequent years. The PFIC rules are complex, and each U.S. Holder should consult its tax advisor regarding the application of the PFIC rules to us.
Default PFIC Rules Under Section 1291 of the Code.
Generally, if we are or have been treated as a PFIC for any taxable year during a U.S. Holder’s holding period of common shares, subject to the special rules described below applicable to a U.S. Holder who makes a Mark-to-Market Election or a QEF Election (each as defined below), any “excess distribution” with respect to the common
41
shares would be allocated ratably over the U.S. Holder’s holding period. The amounts allocated to the taxable year of the excess distribution and to any year before we became a PFIC would be taxed as ordinary income. The amount allocated to each other taxable year would be subject to tax at the highest rate in effect for individuals or corporations in that taxable year, as appropriate, and an interest charge would be imposed on the amount allocated to that taxable year. Distributions made in respect of common shares during a taxable year will be excess distributions to the extent they exceed 125% of the average of the annual distributions on common shares received by the U.S. Holder during the preceding three taxable years or the U.S. Holder’s holding period, whichever is shorter. In addition, dividends generally will not be qualified dividend income if we are a PFIC in the taxable year of payment or the preceding year.
Generally, if we are treated as a PFIC for any taxable year during which a U.S. Holder owns common shares, any gain on the disposition of the common shares would be treated as an excess distribution and would be allocated ratably over the U.S. Holder’s holding period and subject to taxation in the same manner as described in the preceding paragraph and would not be eligible for the preferential long-term capital gains rate.
Certain elections (including the Mark-to-Market Election and the QEF Election, as defined and discussed below) may sometimes be used to mitigate the adverse impact of the PFIC rules on U.S. Holders, but these elections may accelerate the recognition of taxable income and have other adverse consequences.
Each current or prospective U.S. Holder should consult its own tax advisor regarding potential status of us as a PFIC, the possible effect of the PFIC rules to such holder in his, her or its particular circumstances, information reporting required if we were treated as a PFIC and the availability of any election that may be available to the U.S. holder to mitigate adverse U.S. federal income tax consequences of holding shares in a PFIC.
QEF Election.
A U.S. Holder of common shares in a PFIC generally would not be subject to the PFIC rules discussed above if the U.S. Holder had made a timely and effective election (a “QEF Election”) to treat us as a “qualified electing fund” (a “QEF”). Instead, such U.S. Holder would be subject to U.S. federal income tax on its pro rata share of our (i) net capital gain, which would be taxed as long-term capital gain to such U.S. Holder, and (ii) ordinary earnings, which would be taxed as ordinary income to such U.S. Holder, in each case regardless of whether such amounts are actually distributed to such U.S. Holder. However, a U.S. Holder that makes a QEF Election may, subject to certain limitations, elect to defer payment of current U.S. federal income tax on such amounts, subject to an interest charge. If such U.S. Holder is not a corporation, any such interest paid will be treated as “personal interest,” which is not deductible.
A U.S. Holder that makes a timely and effective QEF Election generally (a) may receive a tax-free distribution from us to the extent that such distribution represents our “earnings and profits” that were previously included in income by such U.S. Holder because of such QEF Election and (b) will adjust such U.S. Holder’s tax basis in the common shares to reflect the amount included in income or allowed as a tax-free distribution because of such QEF Election. In addition, for U.S. federal income tax purposes, a U.S. Holder that makes a timely QEF Election generally will recognize capital gain or loss on the sale or other taxable disposition of the common shares.
A QEF Election will be treated as “timely” if such QEF Election is made for the first taxable year in the U.S. Holder’s holding period for the common shares in which we are a PFIC. A U.S. Holder may make a timely QEF Election by filing the appropriate QEF Election documents at the time such U.S. Holder files a U.S. federal income tax return for such first year. If a U.S. Holder makes a QEF Election after the first taxable year in the U.S. Holder’s holding period for the common shares in which we are a PFIC, then, in addition to filing the QEF Election documents, a U.S. Holder may elect to recognize gain (which will be taxed under the rules discussed under “—Default PFIC Rules Under Section 1291 of the Code”) as if the common shares were sold on the qualification date. The “qualification date” is the first day of the first taxable year in which we are a QEF with respect to such U.S. Holder. The election to recognize such gain can only be made if such U.S. Holder’s holding period for the common shares includes the qualification date. By electing to recognize such gain, such U.S. Holder will be deemed to have made a timely QEF Election. In addition, under very limited circumstances, it is possible that a U.S. Holder might make a retroactive QEF Election if such U.S. Holder failed to file the QEF Election documents in a timely manner. If a U.S. Holder fails to make a QEF Election for the first taxable year in the U.S. Holder’s holding period for the common shares in which we are a PFIC and does not elect to recognize gain as if the common shares were sold on the qualification date, such holder will not be treated as having made a “timely” QEF Election and will continue to be subject to the special adverse taxation rules discussed above under “—Default PFIC Rules Under Section 1291 of the Code”.
A QEF Election will apply to the taxable year for which such QEF Election is made and to all subsequent taxable years, unless such QEF Election is invalidated or terminated or the IRS consents to revocation of such QEF Election. If a U.S. Holder makes a QEF Election and, in a subsequent taxable year, we cease to be a PFIC, the QEF Election will remain in effect (although it will not be applicable) during those taxable years in which we are not a PFIC. Accordingly, if we become a PFIC in another subsequent taxable year, the QEF Election will be effective, and the U.S. Holder will be subject to the rules described above during any such subsequent taxable year in which we qualify as a PFIC.
A U.S. Holder cannot make and maintain a valid QEF Election unless we provide certain U.S. tax information necessary to make such an election. On an annual basis, we intend to use commercially reasonable efforts to make available to U.S. Holders, upon their written request (a) timely information as to our status as a PFIC, and (b) for each year in which we are a PFIC, information and documentation that a U.S. Holder making a QEF Election with respect to us is required to obtain for U.S. federal income tax purposes. Each U.S. Holder should consult its own tax advisor regarding the availability of, and procedure for making, a QEF Election with respect to us.
Mark-to-Market Election.
A U.S. Holder of common shares in a PFIC would not be subject to the PFIC rules discussed above under “—Default PFIC Rules Under Section 1291 of the Code” if the U.S. Holder had made a timely and effective election to mark the PFIC common shares to market (a “Mark-to-Market Election”).
A U.S. Holder may make a Mark-to-Market Election with respect to the common shares only if such shares are marketable stock. Such shares generally will be “marketable stock” if they are regularly traded on a “qualified exchange,” which is defined as (a) a national securities exchange that is registered with the SEC, (b) the national market system established pursuant to section 11A of the Exchange Act, or (c) a non-U.S. securities exchange that is regulated or supervised by a governmental authority of the country in which the market is located, provided that (i) such non-U.S. exchange has trading volume, listing, financial disclosure, surveillance, and other requirements, and the laws of the country in which such non-U.S. exchange is located, together with the rules of such non-U.S. exchange, ensure that such requirements are actually enforced and (ii) the rules of such non-U.S. exchange ensure active trading of listed stocks. Our common shares will generally be treated as “regularly traded” in any calendar year in which more than a de minimis quantity of common shares is traded on a qualified exchange for at least 15 days during each calendar quarter. Each U.S. Holder should consult its own tax advisor with respect to the availability of a Mark-to-Market Election with respect to the common shares.
In general, a U.S. Holder that makes a timely Mark-to-Market Election with respect to the common shares will include in ordinary income, for each taxable year in which we are a PFIC, an amount equal to the excess, if any, of (a) the fair market value of the common shares as of the close of such taxable year over (b) such U.S. Holder’s tax basis in such shares. A U.S. Holder that makes a Mark-to-Market Election will be allowed a deduction in an amount equal to the lesser of (a) the excess, if any, of (i) such U.S. Holder’s adjusted tax basis in the common shares over (ii) the fair market value of such shares as of the close of such taxable year or (b) the excess, if any, of (i) the amount included in ordinary income because of such Mark-to-Market Election for prior taxable years over (ii) the amount allowed as a deduction because of such Mark-to-Market Election for prior taxable years. If a U.S. Holder makes a Mark-to-Market Election after the first taxable year in which we are a PFIC and such U.S. Holder has not made a timely QEF Election with respect to us, the PFIC rules described above under “—Default PFIC Rules Under Section 1291 of the Code” will apply to certain dispositions of, and distributions on, the common shares, and the U.S. Holder’s mark-to-market income for the year of the election. If we were to cease being a
42
PFIC, a U.S. Holder that marked its common shares to market would not include mark-to-market gain or loss with respect to its common shares for any taxable year that we were not a PFIC.
A U.S. Holder that makes a Mark-to-Market Election generally will also adjust such U.S. Holder’s tax basis in his common shares to reflect the amount included in gross income or allowed as a deduction because of such Mark-to-Market Election. In addition, upon a sale or other taxable disposition of the common shares subject to a Mark-to-Market Election, any gain or loss on such disposition will be ordinary income or loss (to the extent that such loss does not to exceed the excess, if any, of (a) the amount included in ordinary income because of such Mark-to-Market Election for prior taxable years over (b) the amount allowed as a deduction because of such Mark-to-Market Election for prior taxable years). A Mark-to-Market Election applies to the taxable year in which such Mark-to-Market Election is made and to each subsequent taxable year unless the common shares cease to be “marketable stock” or the IRS consents to revocation of such election. Each U.S. Holder should consult its own tax advisor regarding the availability of, and procedure for making, a Mark-to-Market Election with respect to the common shares.
Reporting.
If we were to be treated as a PFIC in any taxable year, a U.S. Holder will generally be required to file an annual report with the IRS containing such information as the U.S. Treasury Department may require.
Each U.S. Holder should consult its own tax advisor regarding our potential status as a PFIC, the possible effect of the PFIC rules to such holder and information reporting required if we were a PFIC, as well as the availability of any election that may be available to the holder to mitigate adverse U.S. federal income tax consequences of holding shares in a PFIC.
Receipt of Foreign Currency
The amount of a distribution paid in Canadian dollars or Canadian dollar proceeds received on the sale or other taxable disposition of common shares will generally be equal to the U.S. dollar value of the currency on the date of receipt. If any Canadian dollars received with respect to the common shares are later converted into U.S. dollars, U.S. Holders may realize foreign currency gain or loss on the conversion. Any gain or loss generally will be treated as ordinary income or loss and generally will be from sources within the United States for U.S. foreign tax credit purposes. Each U.S. Holder should consult its own tax advisor concerning the possibility of foreign currency gain or loss if any such currency is not converted into U.S. dollars on the date of receipt.
Foreign Tax Credit
Subject to certain limitations, a U.S. Holder who pays (whether directly or through withholding) Canadian or other non-U.S. income tax with respect to the common shares may be entitled, at the election of the U.S. Holder, to receive either a deduction or a credit for Canadian or other non-U.S. income tax paid. Dividends paid on common shares generally will constitute income from sources outside the United States. Any gain from the sale or other taxable disposition of the common shares by a U.S. Holder generally will constitute U.S. source income. The foreign tax credit rules (including the limitations with respect thereto) are complex, and each U.S. Holder should consult its own tax advisor regarding the foreign tax credit rules, having regard to such holder’s particular circumstances.
Information Reporting; Backup Withholding
Generally, information reporting and backup withholding will apply to distributions on, and the payment of proceeds from the sale or other taxable disposition of, the common shares unless (i) the U.S. Holder is a corporation or other exempt entity, or (ii) in the case of backup withholding, the U.S. Holder provides a correct taxpayer identification number, certifies that the U.S. Holder is not subject to backup withholding and otherwise complies with the applicable requirements of the backup withholding rules.
Backup withholding is not an additional tax. Any amount withheld generally will be creditable against a U.S. Holder’s U.S. federal income tax liability or refundable to the extent that it exceeds such liability provided the required information is provided to the IRS in a timely manner.
In addition, certain categories of U.S. Holders must file information returns with respect to their investment in a non-U.S. corporation. For example, certain U.S. Holders must file IRS Form 8938 with respect to certain “specified foreign financial assets” (such as the common shares) with an aggregate value in excess of US$50,000 (and, in some circumstances, a higher threshold). Failure to do so could result in substantial penalties and in the extension of the statute of limitations with respect to such holder’s U.S. federal income tax returns. Each U.S. Holder should consult its own tax advisor regarding application of the information reporting and backup withholding rules to it in connection with an investment in our common shares.
Medicare Contribution Tax
U.S. Holders that are individuals, estates or certain trusts generally will be subject to a 3.8% Medicare contribution tax on, among other things, dividends on, and capital gains from the sale or other taxable disposition of, common shares, subject to certain limitations and exceptions. Each U.S. Holder should consult its own tax advisor regarding possible application of this additional tax to income earned in connection with an investment in our common shares.
Recent Sales of Unregistered Securities
None.
Issuer Repurchases of Equity Securities
None.
Item 6. Reserved
Not applicable.
43
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operation
The following discussion should be read in conjunction with our consolidated financial statements and notes thereto found elsewhere in this annual report. This annual report contains forward-looking statements within the meaning of the U.S. Private Securities Litigation Reform Act of 1995. These statements are subject to risks and uncertainties that could cause actual results and events to differ materially from those expressed or implied by such forward-looking statements. For a detailed discussion of these risks and uncertainties, see Item 1A, “Risk Factors” of this annual report. We caution readers not to place undue reliance on these forward-looking statements, which reflect management’s analysis only as of the date of this annual report. We undertake no obligation to update forward-looking statements which reflect events or circumstances occurring after the date of this annual report, unless required by applicable securities laws.
Introduction
This management’s discussion and analysis, or MD&A, is presented in order to provide the reader with an overview of the financial results and changes to our financial position as at March 31, 2022 and for the twelve-month periods then ended. This MD&A explains the material variations in our operations, financial position and cash flows for the years ended March 31, 2022 and 2021.
Market data and certain industry data and forecasts included in this MD&A were obtained from internal corporation surveys, market research, and publicly available information, reports of governmental agencies and industry publications and surveys. We have relied upon industry publications as our primary sources for third-party industry data and forecasts. Industry surveys, publications and forecasts generally state that the information they contain has been obtained from sources believed to be reliable, but that the accuracy and completeness of that information is not guaranteed. We have not independently verified any of the data from third-party sources or the underlying economic assumptions they made. Similarly, internal surveys, industry forecasts and market research, which we believe to be reliable based upon our management’s knowledge of our industry, have not been independently verified. Our estimates involve risks and uncertainties, including assumptions that may prove not to be accurate, and these estimates and certain industry data are subject to change based on various factors, including those discussed under Item 1.A “Risk Factors” in this annual report. While we believe our internal business, research is reliable and the market definitions we use in this MD&A are appropriate, neither our business research nor the definitions we use have been verified by any independent source.
This MD&A, approved by the Board of Directors on June 21, 2022, should be read in conjunction with our audited consolidated financial statements for the year ended March 31, 2022, and 2021. Our audited financial statements were prepared in accordance with generally accepted accounting principles issued by the Financial Accounting Standards Board in the United States, or GAAP. All amounts appearing in this MD&A for the period-by-period discussions are in thousands of U.S. dollars, except share and per share amounts or unless otherwise indicated.
Basis of Presentation of the Financial Statements
Our consolidated financial statements, which include the accounts of our subsidiaries AIAG and Acasti Pharma US, have been prepared in accordance with GAAP and the rules and regulations of the SEC related to annual reports filed on Form 10-K. All intercompany transactions and balances are eliminated on consolidation.
Our assets as at March 31, 2022, include cash and cash equivalents and short-term investments totalling $43.7 million and intangible assets and goodwill totalling $83.1 million. Our current liabilities total $3.3 million as at March 31, 2022 and are comprised primarily of amounts due to or accrued for creditors.
Comparative Financial Information for the years ended March 31, 2022 and 2021
|
|
Year ended |
|
|||||||||
|
|
March 31, |
|
|
March 31, |
|
|
Increase (Decrease) |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Net loss |
|
|
(9,819 |
) |
|
|
(19,678 |
) |
|
|
(9,859 |
) |
Basic and diluted loss per share |
|
|
(0.27 |
) |
|
|
(1.33 |
) |
|
|
(1.06 |
) |
Total assets |
|
|
128,620 |
|
|
|
62,458 |
|
|
|
66,162 |
|
Working capital1 |
|
|
42,271 |
|
|
|
60,793 |
|
|
|
(18,522 |
) |
Total non-current liabilities |
|
|
17,090 |
|
|
|
5,219 |
|
|
|
11,871 |
|
Total shareholders’ equity |
|
|
108,270 |
|
|
|
55,660 |
|
|
|
52,610 |
|
Results of Operations
Comparison of the year ended March 31, 2022, and 2021
The following table summarizes our results of operations for the year ended March 31, 2022 and 2021:
44
|
|
Year ended |
|
|
|
|
||||||
|
|
March 31, |
|
|
March 31, |
|
|
Increase (Decrease) |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Revenue |
|
|
— |
|
|
|
196 |
|
|
|
(196 |
) |
|
|
|
|
|
|
|
|
|
|
|||
Operating expenses |
|
|
|
|
|
|
|
|
|
|||
Cost of sales of products |
|
|
— |
|
|
|
76 |
|
|
|
(76 |
) |
Research and development expenses, net of government assistance |
|
|
5,559 |
|
|
|
4,173 |
|
|
|
1,386 |
|
General and administrative expenses |
|
|
9,263 |
|
|
|
5,521 |
|
|
|
3,742 |
|
Sales and marketing expenses |
|
|
518 |
|
|
|
1,142 |
|
|
|
(624 |
) |
Impairment of Intangible assets |
|
|
— |
|
|
|
3,706 |
|
|
|
(3,706 |
) |
Impairment of Equipment |
|
|
— |
|
|
|
1,584 |
|
|
|
(1,584 |
) |
Impairment of Other assets and prepaids |
|
|
249 |
|
|
|
413 |
|
|
|
(164 |
) |
Loss from operating activities |
|
|
(15,589 |
) |
|
|
(16,419 |
) |
|
|
(830 |
) |
|
|
|
|
|
|
|
|
|
|
|||
Financial income (expenses) |
|
|
5,122 |
|
|
|
(3,259 |
) |
|
|
8,381 |
|
Income tax recovery |
|
|
648 |
|
|
|
— |
|
|
|
648 |
|
|
|
|
|
|
|
|
|
|
|
|||
Net loss |
|
|
(9,819 |
) |
|
|
(19,678 |
) |
|
|
(9,859 |
) |
Net Loss
The net loss of $9,819 or $0.27 per share for the year ended March 31, 2022, decreased by $9,859 from the net loss of $19,678 or $1.33 per share for the year ended March 31, 2021.
Revenue and cost of sales of products
In October 2020, we entered into a short term agreement with the Centre Integre Universitaire et des services sociaux de L’Estrie – Centre hospitalier Universitaire de Sherbrooke to start producing and selling viral transport medium tubes to be utilized in testing related to the COVID-19 pandemic, for which we generated revenues of $196 for the year ended March 31, 2021. We did not engage in any production and sales under this agreement during the year ended March 31, 2022.
Research and development expenses
Research and development expenses consist primarily of:
We record research and development expenses as incurred.
Our research and development during the year ended March 31, 2022 was focused primarily on our clinical development programs GTX 104, GTX 102, and GTX 101 drug candidates, which were acquired in the Grace merger on August 27, 2021. Research and development expenses during the year ended March 31, 2021, related to the completion of our TRILOGY Phase 3 clinical program for CaPre.
The following table summarizes our research and development expenses:
Research and development expenses |
|
|
|
|
|
|
|
|
|
|||
|
|
Year ended |
|
|
|
|
||||||
|
|
March 31, |
|
|
March 31, |
|
|
Increase (Decrease) |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Third-party contract research expenses: |
|
|
|
|
|
|
|
|
|
|||
Clinical development programs: |
|
|
|
|
|
|
|
|
|
|||
GTX 104 |
|
|
1,796 |
|
|
|
— |
|
|
|
1,796 |
|
GTX 102 |
|
61 |
|
|
|
— |
|
|
|
61 |
|
|
GTX 101 |
|
|
538 |
|
|
|
— |
|
|
|
538 |
|
Other third-party contract research expenses |
|
|
724 |
|
|
|
917 |
|
|
|
(193 |
) |
Professional fees |
|
|
317 |
|
|
|
467 |
|
|
|
(150 |
) |
Other research and development costs |
|
|
236 |
|
|
|
188 |
|
|
|
48 |
|
Government grants & tax credits |
|
|
(577 |
) |
|
|
(127 |
) |
|
|
(450 |
) |
Total third-party research and development expenses1 |
|
|
3,095 |
|
|
|
1,445 |
|
|
|
1,650 |
|
Salaries and benefits |
|
|
2,017 |
|
|
|
1,459 |
|
|
|
558 |
|
Stock-based compensation |
|
|
447 |
|
|
|
353 |
|
|
|
94 |
|
Depreciation and amortization |
|
|
— |
|
|
|
916 |
|
|
|
(916 |
) |
Total |
|
|
5,559 |
|
|
|
4,173 |
|
|
|
1,386 |
|
1 Total third-party research and development expenses is calculated before salaries, depreciation, amortization and stock-based compensation. Because there is no standard method endorsed by GAAP, the results may not be comparable to similar measurements presented by other public companies.
45
Total third-party research and development expenses before salaries and benefits, depreciation, amortization and stock-based compensation expenses for the year ended March 31, 2022, totalled $3,095 compared to $1,445 for the year ended March 31, 2021. This resulted in an increase $1,650 related mostly to the initiation of clinical development programs GTX 104, GTX 102 and GTX 101, which we acquired through the merger with Grace.
Third-party contract research expenses related to GTX 104 amounted to $1,796 from the date our acquisition of Grace as our PK bridging study was initiated and progressed. Third party contract research expenses of $61 related to GTX 102 are a related to the progression of CMC phase 1 work. Third party contract research expenses of $538 related to GTX 101 were mostly related to non-clinical studies and CMC non-clinical work. The program related increases for GTX 104, GTX 102 and GTX 101 were offset by a decrease of $193, related to other third-party contract research expenses. These expenses related to non-clinical outside services and IP legal costs to support and maintain our patents for our three clinical programs GTX 104, GTX 102 and GTX 101 drug candidates. Other third-party contract research expenses for the year end March 31, 2021, related to expenses incurred through the completion and termination of the TRILOGY phase 3 clinical program.
The increase of third party-contract research expenses of were offset by a decrease of $150 of professional fees and an increase of $450 in tax research credits. Salaries and benefits increased by $558 to $2,017 for the year ended March 31, 2022, from $1,459 for the year ended March 31, 2021. The increase is related to additional R&D headcount since the date of the Grace merger, as well as the renewal of our employee incentive bonus program. Government tax credits increased by $450 due to the increased government credit eligible research activities related to our clinical programs GTX 104, GTX 102 and GTX 101.
General and administrative expenses
General and administrative expenses consisted primarily of salaries and related benefits, including share-based compensation, related to our executive, finance, legal, and support functions. Other general and administrative expenses include professional fees for auditing, tax, consulting, rent and utilities and insurance.
General and administrative expenses |
|
|
|
|
|
|
|
|
|
|||
|
|
Year ended |
|
|
|
|
||||||
|
|
March 31, |
|
|
March 31, |
|
|
Increase (Decrease) |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Salaries and benefits |
|
|
1,745 |
|
|
|
1,321 |
|
|
|
424 |
|
Professional fees |
|
|
5,199 |
|
|
|
2,337 |
|
|
|
2,862 |
|
Other |
|
|
1,477 |
|
|
|
1,027 |
|
|
|
450 |
|
General and administrative expense before stock-based compensation and depreciation 1 |
|
|
8,421 |
|
|
|
4,685 |
|
|
|
3,736 |
|
Stock-based compensation |
|
|
842 |
|
|
|
828 |
|
|
|
14 |
|
Depreciation |
|
|
— |
|
|
|
8 |
|
|
|
(8 |
) |
Total |
|
|
9,263 |
|
|
|
5,521 |
|
|
|
3,742 |
|
1 General and administrative sub-total expenses is calculated before stock-based compensation and depreciation. Because there is no standard method endorsed by GAAP, the results may not be comparable to similar measurements presented by other public companies.
General and administrative expenses totalled $8,421 before stock-based compensation and depreciation expense for the year ended March 31, 2022, and increased by $3,736 from $4,685 for the year ended March 31, 2021. This increase was a result of increased legal, tax, accounting and other professional fees related to the Grace merger, and the renewal of our at-the-market program. In addition, salaries and benefits increased by $424 due to the accruals related to the renewal of our employee incentive bonus program.
Sales and marketing
Sales and marketing expenses consist primarily of salaries and related benefits, including share-based compensation, related to our commercial functions.
Sales and marketing expenses |
|
|
|
|
|
|
|
|
|
|||
|
|
Year ended |
|
|
|
|
||||||
|
|
March 31, |
|
|
March 31, |
|
|
Increase (Decrease) |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Salaries and benefits |
|
|
271 |
|
|
|
1,050 |
|
|
|
(779 |
) |
Professional fees |
|
|
83 |
|
|
|
75 |
|
|
|
8 |
|
Other |
|
|
116 |
|
|
|
24 |
|
|
|
92 |
|
Sales and Marketing expenses before stock-based compensation1 |
|
|
470 |
|
|
|
1,149 |
|
|
|
(679 |
) |
Stock-based compensation |
|
|
48 |
|
|
|
(7 |
) |
|
|
55 |
|
Total |
|
|
518 |
|
|
|
1,142 |
|
|
|
(624 |
) |
1 Sales and marketing sub-total expenses is calculated before stock-based compensation. Because there is no standard method endorsed by GAAP, the results may not be comparable to similar measurements presented by other public companies.
Sales and marketing expenses before stock-based compensation expense were $470 for the year ended March 31, 2022, compared to $1,149 for the year ended March 31, 2021. The decrease of $679 was mostly due to a reduction in salaries of $779 due to a reduction in headcount associated with the CaPre program.
Aggregate stock-based compensation expense decreased by $163 to $1,337, for the year ended March 31, 2022, as compared to $1,174 for the year ended March 31, 2021. This increase was due to the timing of the stock options granted during the year ended March 31, 2022 and year ended March 31, 2021.
Aggregate depreciation and amortization expense decreased by $924 for the year ended March 31, 2022, to nil as compared to $924 for the year ended March 31, 2021. This decrease was due to the impact of equipment being classified as held for resale during the year ended March 31, 2021 and no subsequent additional depreciation being recognized.
46
Liquidity and Capital Resources
Share Capital Structure
Our authorized share capital consists of an unlimited number of Class A, Class B, Class C, Class D and Class E shares, without par value. Issued and outstanding fully paid shares, stock options, restricted shares units and warrants, were as follows for the periods ended (all amounts in the table below give effect to the 1-for-8 share consolidation we completed on August 31, 2021):
|
|
March 31, |
|
|
March 31, |
|
||
|
|
Number |
|
|
Number |
|
||
Class A shares, voting, participating and without par value |
|
|
44,288,183 |
|
|
|
26,046,950 |
|
Stock options granted and outstanding |
|
|
2,989,381 |
|
|
|
911,871 |
|
May 2018 Canadian public offering of warrants exercisable at CAD$10.48 until May 9, 2023 |
|
|
824,218 |
|
|
|
824,218 |
|
December 2017 U.S. public offering of warrants exercisable at US$10.08 until December 19, 2022 |
|
|
884,120 |
|
|
|
884,120 |
|
December 2017 U.S. public offering broker warrants exercisable at US$10.10 until December 27, 2022 |
|
|
32,390 |
|
|
|
32,390 |
|
February 2017 Canadian public offering of warrants exercisable at CAD$17.20 until February 21, 2022 |
|
|
— |
|
|
|
215,491 |
|
|
|
|
|
|
|
|
||
Total fully diluted shares |
|
|
49,018,292 |
|
|
|
28,915,040 |
|
Cash Flows and Financial Condition between the years ended March 31, 2022 and March 31, 2021
Summary
As at March 31, 2022, cash and cash equivalents totalled $30,339, a net decrease of $20,603 compared to cash and cash equivalents totalling $50,942 at March 31, 2021. During the year ended March 31, 2021, we received net proceeds of approximately $59.3 million from our at the market (ATM) program. During the year ended March 31, 2022, we did not have financing activities and used existing cash balances for operations purposes.
Operating activities
During the years ended March 31, 2022 and 2021, our operating activities used cash of $17,234 and $14,319 respectively.
Investing activities
During the years ended March 31, 2022 and 2021, we used cash of $3,522 and $9,858 respectively due primarily to the acquisition of investments offset by the maturity of investments.
Financing activities
During the year ended March 31, 2022, our financing activities provided cash totalling nil, compared to cash generated of $59,490 due to proceeds from the sale of shares under our ATM, program.
ATM Program
On June 29, 2020, we entered into an amended and restated sales agreement (the “Sales Agreement”) with B. Riley FBR, Inc., Oppenheimer & Co. Inc. and H.C. Wainwright & Co., LLC (collectively, the “Agents”) to amend our ATM program. Under the terms of the Sales Agreement, which has a three-year term, we may issue and sell from time-to-time common shares having an aggregate offering price of up to $75,000,000 through the Agents. Subject to the terms and conditions of the Sales Agreement, the Agents will use their commercially reasonable efforts to sell the common shares from time to time, based upon our instructions. We have no obligation to sell any of the common shares and may at any time suspend sales under the Sales Agreement. We and the Agents may terminate the Sales Agreement in accordance with its terms. Under the terms of the Sales Agreement, we have provided the Agents with customary indemnification rights and the Agents will be entitled to compensation at a commission rate equal to 3.0% of the gross proceeds from each sale of the common shares.
On November 10, 2021, we filed a prospectus supplement relating to our ATM program to restore available capacity to $75,000,000. The common shares sold under the ATM will be distributed at market prices prevailing at the time of the sale and, as a result, prices may vary between purchasers and during the period of distribution. The volume and timing of sales under the ATM program, if any, will be determined at the sole discretion of our board of directors and management.
During the year ended March 31, 2022, no common shares were sold under the ATM program. During the year ended March 31, 2021, 14.7 million common shares were sold for total net proceeds of approximately $59.3 million with related commissions, legal expenses and costs amounting to $2 million. The common shares were sold at the prevailing market prices, which resulted in an average price of $4.16 per share. Accordingly, proportional costs of $18 related to the common shares sold have been reclassified from deferred financings costs to equity. Total costs incurred relating to the ATM were initially recorded as deferred financing costs in the consolidated balance sheet. During the year ended March 31, 2021, the remaining balance of the costs incurred of $264 were written off to financing expenses.
47
Financial Position
The following table details the significant changes to the statements of financial position as at March 31, 2022, compared to the prior fiscal year end at March 31, 2021:
Accounts |
|
Increase |
|
|
Comments |
|
Cash and cash equivalents |
|
|
(20,603 |
) |
|
See cash flow statement |
Investments |
|
|
3,533 |
|
|
Increase in cash available to invest |
Receivables |
|
|
18 |
|
|
Timing of reimbursement of sales taxes |
Assets held for sale |
|
|
(166 |
) |
|
Impairment of RKO and Foreign exchange |
Prepaid expenses |
|
|
377 |
|
|
Renewal of insurance contract and other prepaid expenses (advances to US vendors) offset by impairment of prepaid RKO |
Right of use asset |
|
|
229 |
|
|
Adjustment to the net present value of lease contract for Sherbrooke |
Intangible assets |
|
|
69,810 |
|
|
Related to acquisition of Grace (IPR&D) |
Goodwill |
|
|
12,964 |
|
|
Related to acquisition of Grace |
Trade and other payables |
|
|
1,663 |
|
|
Timing of payments net of accruals |
Lease liability |
|
|
209 |
|
|
Future obligations offset by payment of lease liability |
Derivative warrant liabilities |
|
|
(5,209 |
) |
|
Change in fair value of derivative warrants |
Deferred tax liability |
|
|
16,889 |
|
|
Related to acquisition of Grace |
See the statement of changes in equity in our financial statements for details of changes to the equity accounts since March 31, 2021.
Treasury Operations
Our treasury policy is to invest cash that is not required immediately into instruments with an investment strategy based on capital preservation. Cash equivalents and marketable securities are primarily made in guaranteed investment certificates, term deposits and high-interest savings accounts, which are issued and held with Canadian chartered banks, highly rated promissory notes issued by government bodies and commercial paper. We hold cash denominated in both U.S. and Canadian dollars. Funds received in U.S. dollars from equity financings are invested as per our treasury policy in U.S. dollar investments and converted to Canadian dollars as appropriate to fulfil operational requirements and funding.
Acquisition of Grace
On August 27, 2021, we completed the acquisition of Grace Therapeutics. In connection with the share-for-share noncash transaction, Grace was merged with a new wholly owned subsidiary of Acasti and became a wholly owned subsidiary of Acasti. Grace was subsequently renamed Acasti Pharma US Inc. As a result of the merger, we acquired Grace’s entire therapeutic pipeline consisting of three unique clinical stage and multiple pre-clinical stage assets supported by an intellectual property portfolio consisting of more than 40 granted and pending patents in various jurisdictions worldwide. Under the terms of the merger, each issued and outstanding share of Grace common stock was automatically converted into the right to receive Acasti common shares equal to the equity exchange ratio set forth in the merger agreement.
Consideration for Acquisition
A total of 18,241,233 common shares of Acasti were issued to Grace stockholders as consideration for the acquisition.
|
|
|
|
|
Total common shares issued |
|
|
18,241,233 |
|
Acasti share price (closing share price on August 27, 2021) |
|
$ |
3.3344 |
|
Fair value of common shares issued |
|
$ |
60,824 |
|
Our acquisition of Grace has been accounted for as a business combination using the acquisition method of accounting. This acquisition method requires, among other things, that assets acquired, and liabilities assumed in a business combination be recognized at their fair values as of the acquisition date. The valuation of assets acquired, and liabilities assumed was finalized during the fourth quarter of the year ended March 31, 2022.
Measurement period adjustments to the preliminary purchase price allocation during 2022 included (i) an increase to intangible assets of $4,602; (ii) an increase to Goodwill of $12,964; (iii) an increase to deferred tax liability of $17,536; and (iv) other individually insignificant adjustments to identifiable net assets of $30. The adjustments primarily resulted from the completion of the valuation of the intangible assets based on facts and circumstances that existed as of the acquisition date and did not result from intervening events subsequent to such date.
The following table summarizes the final fair value of assets acquired and liabilities assumed as of the acquisition date:
|
|
$ |
|
|
Assets acquired and liabilities assumed |
|
|
|
|
Cash and equivalents |
|
|
90 |
|
Prepaid expenses and other current assets |
|
|
74 |
|
Intangible assets – in-process research and development |
|
|
69,810 |
|
Goodwill |
|
|
12,964 |
|
Accounts payable and accrued expenses |
|
|
(4,578 |
) |
Deferred tax liability |
|
|
(17,536 |
) |
Total assets acquired and liabilities assumed |
|
|
60,824 |
|
Intangible assets of $69,810 relate to the value of in-process research and development (“IPR&D”) related to Grace’s therapeutic pipeline, consisting of three unique clinical stage programs/assets. The value of which has been attributed as follows:
48
|
|
$ |
|
|
Intangible assets – in-process research and development |
|
|
|
|
GTX 104 |
|
|
27,595 |
|
GTX 102 |
|
|
31,908 |
|
GTX 101 |
|
|
10,307 |
|
Total |
|
|
69,810 |
|
Goodwill of $12,964 was calculated as the excess of the consideration transferred over the net assets recognized and represents the future economic benefits arising from the other assets acquired that could not be individually identified and separately recognized.
Acquired In-Process Research and Development
In a business combination, the fair value of IPR&D acquired is capitalized and accounted for as indefinite-lived intangible assets, and not amortized until the underlying project receives regulatory approval, at which point the intangible assets will be accounted for as a definite-lived intangible assets or discontinued. If discontinued, the intangible asset will be written off. R&D costs incurred after the acquisition are expensed as incurred.
The estimated fair values of identifiable intangible assets were determined using the multi-period excess earnings method, which is a valuation methodology that provides an estimate of the fair value of an asset based on market participant expectations of the cash flows that an asset would generate over its remaining useful life. The significant assumptions used in the valuation are the discount rate, the probability of clinical success of research and development programs, obtaining regulatory approval and forecasted net sales.
Goodwill and indefinite-lived assets are not amortized but are subject to an impairment review annually and more frequently when indicators of impairment exist. An impairment of goodwill could occur if the carrying amount of a reporting unit exceeds the fair value of that reporting unit. An impairment of indefinite-lived intangible assets would occur if the fair value of the intangible asset is less than the carrying value.
Acquisition-related expenses, which were comprised primarily of regulatory, financial advisory and legal fees, totalled $3.2 million for the year ended March 31, 2022, and were included in general and administrative expenses in the condensed consolidated interim statements of earnings. The net loss attributed to Grace in the consolidated statement of loss for the year ended March 31, 2022, since the date of acquisition is immaterial.
Pro Forma Financial Information
The following table presents the unaudited pro forma combined results of operations of Acasti and Grace for the year ended March 31, 2022, as if the acquisition of Grace had occurred on April 1, 2020:
|
|
|
|
Year ended March 31, 2022 |
|
|
|
|
|
|
$ |
|
|
Net loss |
|
|
|
|
(13,734 |
) |
Assets Held for Sale
We determined to actively market for sale Other assets and Equipment and have met the criteria for classification of assets held for sale:
|
|
|
|
|
|
|
||
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Other assets (a) |
|
|
195 |
|
|
|
387 |
|
Equipment (b) |
|
|
407 |
|
|
|
381 |
|
|
|
|
602 |
|
|
|
768 |
|
a. Other Assets
Other assets represent krill oil (RKO) held by us that was expected to be used in the conduct of R&D activities and commercial inventory scale up related to the development and commercialization of our previous drug candidate, CaPre. Given that the development of CaPre will no longer be pursued, we expect to sell this reserve. The other asset is being recorded at the fair value less costs to sell, which has resulted in an impairment loss of $249 (2021- $413). Management’s estimate of the fair value of the RKO less cost -to sell, is based primarily on estimated market prices obtained from an appraiser specialized in the krill oil market. These projections are based on Level 3 inputs of the fair value hierarchy and reflect management’s best estimate of market participants’ pricing of the assets as well as the general condition of the asset. The total impairment loss recognized, includes amounts paid for krill oil in advance, but not yet received and was recorded as a prepaid asset.
b. Equipment
March 31, 2022 |
|
Cost, net of impairment |
|
|
Accumulated |
|
|
Net book |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Furniture and office equipment |
|
|
17 |
|
|
|
(5 |
) |
|
|
12 |
|
Computer equipment |
|
|
94 |
|
|
|
(6 |
) |
|
|
88 |
|
Laboratory equipment |
|
|
585 |
|
|
|
(435 |
) |
|
|
150 |
|
Production equipment |
|
|
1,179 |
|
|
|
(1,022 |
) |
|
|
157 |
|
|
|
|
1,875 |
|
|
|
(1,468 |
) |
|
|
407 |
|
49
March 31, 2021 |
|
Cost |
|
|
Accumulated |
|
|
Impairment |
|
|
Net book |
|
||||
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Furniture and office equipment |
|
|
17 |
|
|
|
(5 |
) |
|
|
— |
|
|
|
12 |
|
Computer equipment |
|
|
148 |
|
|
|
(30 |
) |
|
|
(54 |
) |
|
|
64 |
|
Laboratory equipment |
|
|
756 |
|
|
|
(436 |
) |
|
|
(171 |
) |
|
|
149 |
|
Production equipment |
|
|
2,538 |
|
|
|
(1,023 |
) |
|
|
(1,359 |
) |
|
|
156 |
|
|
|
|
3,459 |
|
|
|
(1,494 |
) |
|
|
(1,584 |
) |
|
|
381 |
|
For the year ended March 31, 2021, depreciation expense was $143 and was included in research and development expenses. Equipment is made up of laboratory, production, computer and office equipment that was utilized in the development of CaPre. Given that the development of CaPre will no longer be pursued by the Corporation, it is expected to sell this equipment. Similar, to how the intangible assets are treated, the announcement of the outcomes of the TRILOGY clinical trials resulted in an impairment trigger for the laboratory and production equipment. The impairment loss is based on management’s estimate of the fair value of the equipment less cost -to sell, which is based primarily on estimated market prices obtained from brokers specialized in selling used equipment. These projections are based on Level 3 inputs of the fair value hierarchy and reflect the management’s best estimate of market participants’ pricing of the assets as well as the general condition of the assets.
Derivative Warrant Liabilities
A total of 1,369,937 warrants were issued as part of our May 2018 public offering in Canada and recognized as derivative warrant liabilities with a fair value at inception of $3,323. As of March 31, 2022, the derivative warrant liability for the remaining 824,218 warrants totalled $10, which represents the fair value of these warrants as at March 31, 2022. The weighted average fair value of the warrants issued in the May 2018 public offering in Canada was determined to be CAD $3.10 per warrant at inception and approximately CAD $0.02 (US $0.01) per warrant as at March 31, 2022.
On December 27, 2017, 1,225,366 warrants were issued as part of our U.S. public offering and recognized as derivative warrant liabilities with a fair value at inception of $4,548. The December 2017 warrants are derivative warrant liabilities for accounting purposes due to the currency of the exercise price (US$) being different from our Canadian dollar functional currency. As of March 31, 2022, the derivative warrant liability for the remaining 884,120warrants totalled nil, which represents the fair value of these warrants as at March 31, 2022. The weighted average fair value of the December 2017 warrants issued was determined to be CAD $4.77 per warrant at inception and approximately nil per warrant as at March 31, 2022.
The variance in the fair value of both existing derivative warrant liabilities as at March 31, 2022, is mostly due to the fluctuations in our share price and the dilution factor. During the year ended March 31, 2022, no warrants were exercised.
Contractual Obligations and Commitments
As at March 31, 2022, our contractual liabilities totalled $3,461 of which $3,260 was due within 1 year, and $10 related to derivative warrant liabilities that are expected to be settled in common shares.
A summary of our contractual obligations at March 31, 2022, is as follows:
Contractual Obligations and commitments |
|
Total |
|
|
Less than |
|
|
1-3 years |
|
|
More than |
|
||||
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Trade and other payables |
|
|
3,156 |
|
|
|
3,156 |
|
|
|
|
|
|
|
||
Operating lease obligations |
|
|
326 |
|
|
|
103 |
|
|
|
223 |
|
|
|
— |
|
RKO supply agreement |
|
|
2,800 |
|
|
|
2,800 |
|
|
|
— |
|
|
|
— |
|
Total |
|
|
6,282 |
|
|
|
6,059 |
|
|
|
223 |
|
|
|
— |
|
Research and Development Contracts and Contract Research Organizations Agreements
We utilize contract manufacturing organizations, for the development and production of clinical materials and contract research organizations to perform services related to our clinical trials. Pursuant to the agreements with these contract manufacturing organizations and contract research organizations, we have either the right to terminate the agreements without penalties or under certain penalty conditions. As such, the amount of commitments is excluded from the above table.
Leases
On March 14, 2022, we renewed the lease agreement effective April 1, 2022 for our research and development and quality control laboratory facility located in Sherbrooke, Québec, resulting in a commitment of $556 over a 24 months base lease term and 48 months additional lease renewal term. This is not reflected in table above as it is effective April 1, 2022.
On February 25, 2022, we renewed the lease agreement effective March 1, 2022, for our research and development and quality control laboratory facility located in North Brunswick, New Jersey, resulting in an obligation of $303 over a 36 months lease term. As at March 31, 2022, the remaining balance of the obligation amounted to $326.
RKO Supply Agreement
On October 25, 2019, we signed a supply agreement with Aker Biomarine Antartic. (“Aker”) to purchase raw krill oil product for a committed volume of commercial starting material for CaPre for a total fixed value of $3.1 million. As at March 31, 2022, the remaining balance of the commitment with Aker amounts to $2.8 million. As of March 31, 2022 the remaining balance of the krill oil product has not been made available for delivery by the supplier under the terms of the supply agreement, therefore no liability has been recorded. Acasti no longer has any planned use for the raw krill oil product for its own operating purposes and therefore we would seek to sell the product upon receipt. There is uncertainty whether we can recover value from the raw krill oil product and we expect we may incur a loss on this contract in the near term.
50
Off-Balance Sheet Arrangements
As of the date of this annual report, we do not have any off-balance sheet arrangements that have or are reasonably likely to have a current or future effect on our financial condition, changes in financial condition, revenues or expenses, results of operations, liquidity, capital expenditures or capital resources that are material to investors.
Use of Estimates and Measurement of Uncertainty
The preparation of our financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, income, and expenses. Actual results may differ from these estimates.
Estimates are based on management’s best knowledge of current events and actions that management may undertake in the future. Estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimates are revised and in any future periods affected.
Estimates and assumptions include the measurement of derivative warrant liabilities, stock-based compensation, assets held for sale, acquisition of Grace valuation of intangibles and the RKO supply agreement. Estimates and assumptions are also involved in measuring the accrual of services rendered with respect to research and development expenditures at each reporting date and determining which research and development expenses qualify for research and development tax credits and in what amounts. We recognize the tax credits once we have reasonable assurance that they will be realized. Recorded tax credits are subject to review and approval by tax authorities and, therefore, could be different from the amounts recorded. Estimates and assumptions are also utilized in the assessment of impairment of deferred financing costs, equipment, and intangibles.
Critical Accounting Policies
Valuation of Intangible Assets
In a business combination, the fair value of IPR&D acquired is capitalized and accounted for as indefinite-lived intangible assets, and not amortized until the underlying project receives regulatory approval, at which point the intangible assets will be accounted for as definite-lived intangible assets or discontinued. If discontinued, the intangible assets will be written off. R&D costs incurred after the acquisition are expensed as incurred.
The estimated fair values of identifiable intangible assets were determined using the multi-period excess earnings method, which is a valuation methodology that provides an estimate of the fair value of an asset based on market participant expectations of the cash flows an asset would generate over its remaining useful life. The projected discounted cash flow models used to estimate the fair value of assets of our IPR&D reflect significant assumptions and are level 3 unobservable data regarding the estimates a market participant would make in order to evaluate a drug development asset, including the following:
Based on our valuation assumptions described above, as at the date of acquisition, varying the discount rate would result in the following range in value attributable to each IPR&D intangible asset, related to Grace’s therapeutic pipeline, assuming that all other variables remain constant.
Discount assumption |
|
GTX 104 |
|
GTX 102 |
|
GTX 101 |
|
Total |
|
||||
|
|
$ |
|
$ |
|
$ |
|
$ |
|
||||
19.5% |
|
|
26,842 |
|
|
30,564 |
|
|
9,460 |
|
|
66,867 |
|
19.2% (discount rate used in valuation) |
|
|
27,595 |
|
|
31,908 |
|
|
10,307 |
|
|
69,810 |
|
19.0% |
|
|
28,371 |
|
|
33,305 |
|
|
11,009 |
|
|
72,685 |
|
The valuation of our acquired IPR&D has significant measurement uncertainty given the lack of historical data on which to base assumptions. We engaged a third party valuation firm to assist us with the valuation of the IPR&D. Assumptions are difficult to make accurately and were mainly derived from life science studies, industry data, and peer company information that our management believes represent appropriate comparable data.
Goodwill and indefinite-lived assets are not amortized but are subject to an impairment review annually and more frequently when indicators of impairment exist. An impairment of goodwill could occur if the carrying amount of a reporting unit exceeds the fair value of that reporting unit. An impairment of indefinite-lived intangible assets would occur if the fair value of the intangible asset is less than the carrying value.
We test goodwill for impairment by first assessing qualitative factors to determine whether it is more likely than not that the fair value is less than its carrying amount. If we conclude it is more likely than not that fair value of the reporting unit is less than its carrying amount, a quantitative impairment test is performed. We test indefinite-lived intangible assets for impairment by first assessing qualitative factors to determine whether it is more likely than not that the fair value is less than its carrying amount. If we conclude it is more likely than not that the fair value is less than its carrying amount, a quantitative impairment test is performed. There were no triggering events from the date of acquisition of Grace to the end of the year. Our annual impairment test will be performed in the third quarter of the fiscal year.
Measurement of Assets Held for Sale and RKO Supply Agreement
Assets that are classified as held for sale are measured at the lower of their carrying amount or fair value less expected selling costs (“estimated selling price”) with a loss recognized to the extent that the carrying amount exceeds the estimated selling price. The classification is applicable at the date upon which the sale of assets is probable, and the assets are available for immediate sale in their present condition. Assets, once classified as held for sale, are not subject to depreciation or amortization and both the assets and any liabilities directly associated with the assets held for sale are classified as current in our consolidated balance sheets. Subsequent changes to the estimated
51
selling price of assets held for sale are recorded as gains or losses to the consolidated statements of income wherein the recognition of subsequent gains is limited to the cumulative loss previously recognized.
In addition, there is judgement and potential for loss regarding the recognition and measurement of our RKO supply agreement with Aker to purchase raw krill oil product for a committed volume of commercial starting material for CaPre for a total fixed value of $3.1 million, which is described in more detail in note 20(a) of our financial statements found elsewhere in this annual report.
Financial Instruments
Credit Risk
Credit risk is the risk of a loss if a customer or counterparty to a financial asset fails to meet its contractual obligations. We have credit risk relating to cash, cash equivalents and marketable securities, which we manage by dealing only with highly rated Canadian institutions. The carrying amount of financial assets, as disclosed in the statements of financial position, represents our credit exposure at the reporting date.
Currency Risk
We are exposed to the financial risk related to the fluctuation of foreign exchange rates and the degrees of volatility of those rates. Foreign currency risk is limited to the portion of our business transactions denominated in currencies other than the Canadian dollar. Fluctuations related to foreign exchange rates could cause unforeseen fluctuations in our operating results.
A portion of our expenses, mainly related to research contracts and purchase of production equipment, is incurred in U.S. dollars, for which no financial hedging is in place. There is a financial risk related to the fluctuation in the value of the U.S. dollar in relation to the Canadian dollar. In order to minimize the financial risk related to the fluctuation in the value of the U.S. dollar in relation to the Canadian dollar, funds which were part of U.S. dollar financings continue to be invested as short-term investments in the U.S. dollar.
Furthermore, a portion of our cash and cash equivalents and marketable securities are denominated in U.S. dollars, further exposing us to fluctuations in the value of the U.S. dollar in relation to the Canadian dollar.
The following table provides an indication of our significant foreign exchange currency exposures at the following dates:
|
|
March 31, |
|
|
March 31, |
|
||||||||||
Denominated in |
|
US |
|
|
Euro |
|
|
US |
|
|
Euro |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Cash and cash equivalents |
|
|
35,079 |
|
|
|
— |
|
|
|
58,176 |
|
|
|
— |
|
Investments |
|
|
14,872 |
|
|
|
— |
|
|
|
9,475 |
|
|
|
— |
|
Trade and other payables |
|
|
(2,130 |
) |
|
|
(79 |
) |
|
|
(687 |
) |
|
|
(2,141 |
) |
|
|
|
47,821 |
|
|
|
(79 |
) |
|
|
66,964 |
|
|
|
(2,141 |
) |
The following exchange rates are those applicable to the following periods and dates:
|
|
March 31, |
|
|
March 31, |
|
||||||||||
|
|
Average |
|
|
Reporting |
|
|
Average |
|
|
Reporting |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
CAD$ per US$ |
|
|
1.2536 |
|
|
|
1.2505 |
|
|
|
1.3212 |
|
|
|
1.2562 |
|
CAD$ per Euro |
|
|
1.4569 |
|
|
|
1.3836 |
|
|
|
1.5409 |
|
|
|
1.4736 |
|
Based on our foreign currency exposures noted above, varying the above foreign exchange rates to reflect a 5% strengthening of the U.S. dollar and Euro would have an increase (decrease) in net loss as follows, assuming that all other variables remain constant:
|
|
March 31, |
|
|
March 31, |
|
||
|
|
$ |
|
|
$ |
|
||
|
|
|
|
|
|
|
||
Increase (decrease) in net loss |
|
|
3,129 |
|
|
|
4,048 |
|
An assumed 5% weakening of the foreign currencies would have an equal but opposite effect on the basis that all other variables remained constant.
Interest Rate Risk
Interest rate risk is the risk that the fair value or future cash flows of a financial instrument will fluctuate because of changes in market rates. Our exposure to interest rate risk as at March 31, 2022 and March 31, 2021 was as follows:
Cash and cash equivalents |
|
Short-term fixed interest rate |
Investments |
|
Short-term fixed interest rate |
Our capacity to reinvest the short-term amounts with equivalent return will be impacted by variations in short-term fixed interest rates available on the market. Management believes the risk we will realize a loss as a result of the decline in the fair value of our short-term investments is limited because these investments have short-term maturities and are held to maturity.
52
Liquidity risk
Liquidity risk is the risk that we will not be able to meet our financial obligations as they fall due. We manage liquidity risk through the management of our capital structure and financial leverage. We also manage liquidity risk by continuously monitoring actual and projected cash flows. The Board of Directors reviews and approves our operating budgets and reviews material transactions outside the normal course of business.
Our contractual obligations related to financial instruments and other obligations and liquidity resources are presented in the liquidity and capital resources of this MD&A.
Future Accounting Changes
We have considered recent accounting pronouncements and concluded that they are either not applicable to our business or that the effect is not expected to be material to our consolidated financial statements as a result of future adoption.
53
Item 7A. Quantitative and Qualitative Disclosure About Market Risk
Information relating to quantitative and qualitative disclosures about market risks is detailed in “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operation.”
Item 8. Financial Statements and Supplementary Data
See our consolidated financial statements beginning on page F-1 of this annual report on Form 10-K.
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None.
Item 9A. Controls and Procedures Disclosure Controls and Procedures
As of the end of the period covered by this annual report, our management, with the participation of our chief executive officer (“CEO”) and chief financial officer (“CFO”), has performed an evaluation of the effectiveness of our disclosure controls and procedures within the meaning of Rules 13a-15 (e) and 15d-15(e) of the Exchange Act. Based upon this evaluation, our management has concluded that, as of March 31, 2022, our existing disclosure controls and procedures were effective. It should be noted that while the CEO and CFO believe that our disclosure controls and procedures provide a reasonable level of assurance that they are effective, they do not expect the disclosure controls and procedures to be capable of preventing all errors and fraud. A control system, no matter how well conceived or operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met.
Management’s Report on Internal Controls over Financial Reporting
Our management, with the participation of our CEO and CFO, is responsible for establishing and maintaining adequate internal control over financial reporting. Our internal control system was designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation and fair presentation of our financial statements. All internal control systems, no matter how well designed, have inherent limitations. Therefore, even those systems determined to be effective may not prevent or detect misstatements and can provide only reasonable assurance with respect to financial statement preparation and presentation. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate. Our management conducted an assessment of the design and operation effectiveness of our internal control over financial reporting as of March 31, 2022. In making this assessment, we used the criteria established within the Internal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on this assessment, our management has concluded that, as of March 31, 2022, our internal control over financial reporting was effective.
Changes in Internal Control over Financial Reporting
No changes were made to our internal controls over financial reporting that occurred during the year ended March 31, 2022 that have materially affected, or are reasonably likely to materially affect, our internal controls over financial reporting. The merger resulted in Grace being included in our current control environment over financial reporting as at the date of the completion of the business combination.
We are a non-accelerated filer under the Exchange Act and not required to comply with the auditor attestation requirements of Section 404(b) of the Sarbanes-Oxley Act of 2002. Therefore, this annual report does not include an attestation report of our registered public accounting firm regarding our management’s assessment of internal control over financial reporting.
Item 9B. Other Information
None.
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections
None.
54
PART III
Item 10. Directors, Executive Officers and Corporate Governance
The information required by this Item is included in the Company’s 2022 Proxy Statement to be filed with the SEC within 120 days after March 31, 2022 in connection with the solicitation of proxies for the Company’s 2022 annual meeting of shareholders, and is incorporated herein by reference.
Item 11. Executive Compensation Summary of our Compensation Programs
The information required by this Item is included in the Company’s 2022 Proxy Statement to be filed with the SEC within 120 days after March 31, 2022 in connection with the solicitation of proxies for the Company’s 2022 annual meeting of shareholders, and is incorporated herein by reference.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Shareholder Matters Equity Compensation Plan Information
The information required by this Item is included in the Company’s 2022 Proxy Statement to be filed with the SEC within 120 days after March 31, 2022 in connection with the solicitation of proxies for the Company’s 2022 annual meeting of shareholders, and is incorporated herein by reference.
Item 13. Certain Relationships and Related Transactions and Director Independence Related Transactions
The information required by this Item is included in the Company’s 2022 Proxy Statement to be filed with the SEC within 120 days after March 31, 2022 in connection with the solicitation of proxies for the Company’s 2022 annual meeting of shareholders, and is incorporated herein by reference.
Item 14. Principal Accounting Fees and Services Audit Fees
The information required by this Item is included in the Company’s 2022 Proxy Statement to be filed with the SEC within 120 days after March 31, 2022 in connection with the solicitation of proxies for the Company’s 2022 annual meeting of shareholders, and is incorporated herein by reference.
55
PART IV
Item 15. Exhibits, Financial Statement Schedules
(a)(1) Financial Statements—The financial statements included in Item 8 are filed as part of this annual report on Form 10-K.
(a)(2) Financial Statement Schedules—All schedules have been omitted because they are not applicable or required, or the information required to be set forth therein is included in the consolidated Financial Statements or notes thereto included in Item 8 of this annual report on Form 10-K.
(a)(3) Exhibits—The exhibits required by Item 601 of Regulation S-K are listed in paragraph (b) below.
(b) Exhibits—The exhibits listed on the Exhibit Index below are filed herewith or are incorporated by reference to exhibits previously filed with the SEC.
Item 16. Form 10-K Summary
None.
56
EXHIBITS INDEX
Exhibit No. |
|
Description |
|
|
|
2.1 |
|
Agreement and Plan of Merger dated as of May 7, 2021 among Acasti Pharma Inc., Acasti Pharma U.S., Inc. and Grace Therapeutics Inc. (incorporated by reference to Exhibit 2.1 from Form 8-K filed with the SEC on May 7, 2021) |
|
|
|
3.1 |
|
|
|
|
|
3.2 |
|
Articles of Amendment (incorporated by reference to Exhibit 3.1 from Form 8-K filed with the SEC on August 27, 2021) |
|
|
|
3.2 |
|
|
|
|
|
3.3 |
|
|
|
|
|
4.1 |
|
|
|
|
|
4.2 |
|
|
|
|
|
4.3 |
|
|
|
|
|
4.4 |
|
|
|
|
|
4.5 |
|
|
|
|
|
4.6 |
|
|
|
|
|
10.1 |
|
|
|
|
|
10.2 |
|
Acasti Pharma Inc., Equity Incentive Plan, as amended August 27, 2020. |
|
|
|
10.3 |
|
Acasti Pharma Inc., Stock Option Plan, as amended June 24, 2021. |
|
|
|
10.4 |
|
|
|
|
|
10.5 |
|
|
|
|
|
10.6 |
|
Employment Agreement with Brian Ford dated September 23, 2021. |
|
|
|
23.1 |
|
Consent of KPMG LLP, an Independent Registered Public Accounting Firm. |
|
|
|
31.1 |
|
|
|
|
|
31.2 |
|
|
|
|
|
32.1 |
|
|
|
|
|
32.2 |
|
|
|
|
|
101.INS |
|
Inline XBRL Instance Document |
|
|
|
101.SCH |
|
Inline XBRL Taxonomy Extension Schema Document |
|
|
|
101.CAL |
|
Inline XBRL Taxonomy Extension Calculation Linkbase Document |
|
|
|
101.DEF |
|
Inline XBRL Taxonomy Extension Definition Linkbase Document |
|
|
|
101.LAB |
|
Inline XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
57
101.PRE |
|
Inline XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
104 |
|
Cover Page Interactive Data File (formatted as Inline XBRL and contained in Exhibit 101) |
58
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
Dated: June 21, 2022 |
|
|
|
ACASTI PHARMA INC. |
|
|
|
|
|
By: |
/s/ Janelle D’Alvise |
|
Name: |
Janelle D’Alvise |
|
|
Title: President and Chief Executive Officer and |
|
|
Director (Principal Executive Officer) |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Signature |
|
Title |
|
Date |
|
|
|
|
|
/s/ Janelle D’Alvise |
|
President and Chief Executive Officer and Director |
|
June 21, 2022 |
Janelle D’Alvise |
|
(Principal Executive Officer) |
|
|
|
|
|
|
|
/s/ Brian Ford |
|
Chief Financial Officer |
|
June 21, 2022 |
Brian Ford |
|
(Principal Financial Officer and Principal Accounting Officer)
|
|
|
/s/ Dr. Roderick N. Carter |
|
Director |
|
June 21, 2022 |
Dr. Roderick N. Carter |
|
|
|
|
|
|
|
|
|
/s/ Jean-Marie (John) Canan |
|
Director |
|
June 21, 2022 |
Jean-Marie (John) Canan |
|
|
|
|
|
|
|
|
|
/s/ Donald Olds |
|
Director |
|
June 21, 2022 |
Donald Olds |
|
|
|
|
|
|
|
|
|
/s/Vimal Kavuru |
|
Director |
|
June 21, 2022 |
Vimal Kavuru |
|
|
|
|
|
|
|
|
|
/s/William Haseltine |
|
Director |
|
June 21, 2022 |
William Haseltine |
|
|
|
|
|
|
|
|
|
/s/Michael L.Derby |
|
Director |
|
June 21, 2022 |
Michael L.Derby |
|
|
|
|
59
ACASTI PHARMA INC.
Consolidated Financial Statements
For the years ended March 31, 2022 and 2021
F-4 |
|
F-5 |
|
F-6 |
|
F-7 |
|
F-8 |
F-1

REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Report of Independent Registered Public Accounting Firm
To the Shareholders and Board of Directors of Acasti Pharma Inc.:
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheets of Acasti Pharma Inc. (the "Company") as of March 31, 2022 and 2021, the related consolidated statements of loss and comprehensive loss, changes in shareholders’ equity, and cash flows for the years ended March 31, 2022 and 2021, and the related notes (collectively, the "consolidated financial statements"). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company as of March 31, 2022 and 2021, and the results of its operations and its cash flows for the years ended March 31, 2022 and 2021, in conformity with U.S. generally accepted accounting principles.
Basis for Opinion
These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) ("PCAOB") and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matter
The critical audit matter communicated below is a matter arising from the current period audit of the consolidated financial statements that was communicated or required to be communicated to the audit committee and that: (1) relates to accounts or disclosures that are material to the consolidated financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of a critical audit matter does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing a separate opinion on the critical audit matter or on the accounts or disclosures to which it relates.
KPMG LLP, an Ontario limited liability partnership and member firm of the KPMG global organization of independent
member firms affiliated with KPMG International Limited, a private English company limited by guarantee. KPMG
Canada provides services to KPMG LLP.
F-2
Page 2
Valuation of in-process research and development intangible assets
As discussed in Note 4 to the consolidated financial statements, on August 27, 2021, the Corporation completed its acquisition of all outstanding equity interests in Grace Therapeutics Inc. The acquisition has been accounted for as a business combination using the acquisition method of accounting. The fair value of the purchase price was allocated to the assets acquired and liabilities assumed at their respective fair values. Intangible assets of $69,810 relate to the value of in-process research and development (“IPR&D”). Management estimated the fair value of the IPR&D intangible assets using a multi-period excess earnings method. The significant assumptions used in the valuation are the discount rate, the probability of clinical success of research and development programs and obtaining regulatory approval, and forecasted net sales.
We identified the assessment of the fair value of the IPR&D intangible assets as a critical audit matter. This required a high degree of auditor judgment and an increased extent of effort when performing procedures due to the measurement uncertainty related to the significant assumptions and the selection of the valuation methodology.
The following are the primary procedures we performed to address this critical audit matter. We evaluated the design of an internal control related to the valuation of IPR&D intangible assets process including the significant assumptions used in the valuation. We compared the assumptions related to probability of clinical success of research and development programs and obtaining regulatory approval to third-party data regarding clinical trial success rates. We assessed the forecasted net sales by comparing them to certain peer companies and/or industry data. We involved valuation professionals with specialized skills and knowledge, who assisted in:
We have served as the Company’s auditor since 2009.
Montréal, Québec
June 21, 2022
F-3
ACASTI PHARMA INC.
Consolidated Balance Sheets
|
|
|
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
|||
(Expressed in thousands of U.S. dollars except share data) |
|
Notes |
|
|
$ |
|
|
$ |
|
|||
Assets |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Current assets: |
|
|
|
|
|
|
|
|
|
|||
Cash and cash equivalents |
|
|
|
|
|
|
|
|
|
|||
Short- term investments |
|
|
6 |
|
|
|
|
|
|
|
||
Receivables |
|
|
5 |
|
|
|
|
|
|
|
||
Assets held for sale |
|
|
8 |
|
|
|
|
|
|
|
||
Prepaid expenses |
|
|
|
|
|
|
|
|
|
|||
Total current assets |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Right of Use Asset |
|
|
|
|
|
|
|
|
|
|||
Intangible assets |
|
|
4 |
|
|
|
|
|
|
|
||
Goodwill |
|
|
4 |
|
|
|
|
|
|
|
||
Total assets |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Liabilities and Shareholders’ equity |
|
|
|
|
|
|
|
|
|
|||
Current liabilities: |
|
|
|
|
|
|
|
|
|
|||
Trade and other payables |
|
|
10 |
|
|
|
|
|
|
|
||
Lease liability |
|
|
|
|
|
|
|
|
|
|||
Total current liabilities |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Derivative warrant liabilities |
|
11, 12(b) |
|
|
|
|
|
|
|
|||
Lease Liability |
|
|
|
|
|
|
|
|
|
|||
Deferred tax liability |
|
4 |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Total liabilities |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Shareholders’ Equity: |
|
|
|
|
|
|
|
|
|
|||
Common shares |
|
|
12 |
|
|
|
|
|
|
|
||
Additional paid-in capital |
|
|
12 |
|
|
|
|
|
|
|
||
Accumulated other comprehensive loss |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
Accumulated deficit |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
Total Shareholder’s equity |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
|
|
20 |
|
|
|
|
|
|
|
|||
Total liabilities and shareholders’ equity |
|
|
|
|
|
|
|
|
|
|||
The accompanying notes are an integral part of these consolidated financial statements
F-4
ACASTI PHARMA INC.
Consolidated Statements of Loss and Comprehensive Loss
|
|
|
|
|
Year ended March 31, 2022 |
|
|
Year ended March 31, 2021 |
|
|||
(Expressed in thousands of U.S. dollars except share data) |
|
Notes |
|
|
$ |
|
|
$ |
|
|||
Revenues |
|
|
|
|
|
|
|
|
|
|||
Revenues from product sales |
|
|
13 |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
Operating Expenses |
|
|
|
|
|
|
|
|
|
|||
Cost of sales of products |
|
|
|
|
|
|
|
|
( |
) |
||
Research and development expenses, net of government assistance |
|
|
9 |
|
|
|
( |
) |
|
|
( |
) |
General and administrative expenses |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
Sales and marketing |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
Impairment of Intangible assets |
|
|
7 |
|
|
|
|
|
|
( |
) |
|
Impairment of Equipment |
|
|
8 |
|
|
|
|
|
|
( |
) |
|
Impairment of Other assets and prepaid |
|
|
8 |
|
|
|
( |
) |
|
|
( |
) |
Loss from operating activities |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
Financial income (expenses) |
|
|
14 |
|
|
|
|
|
|
( |
) |
|
Loss before income tax recovery |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|||
Income tax recovery |
|
|
18 |
|
|
|
|
|
|
|
||
Net loss and total comprehensive loss |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|||
Basic and diluted loss per share |
|
|
16 |
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|||
Weighted average number of shares outstanding |
|
|
|
|
|
|
|
|
|
|||
The accompanying notes are an integral part of these consolidated financial statements
F-5
ACASTI PHARMA INC.
(Expressed in thousands of U.S. dollars except share data)
|
|
Common Shares |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
Notes |
|
|
Number |
|
|
Dollar |
|
|
Additional |
|
|
Accumulated |
|
|
Deficit |
|
|
Total |
|
|||||||
|
|
|
|
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
|||||||
Balance, March 31, 2021 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|||||
Net loss and total comprehensive loss for the period |
|
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
( |
) |
|
|
( |
) |
|
Cumulative translation adjustment |
|
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
|||
Stock based compensation |
|
|
15 |
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
||
Common shares issued in relation to merger with Grace via share-for-share, net |
|
|
4 |
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|||
Balance at March 31, 2022 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|||||
|
|
Common Shares |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
Notes |
|
Number |
|
|
Dollar |
|
|
Additional |
|
|
Accumulated |
|
|
Deficit |
|
|
Total |
|
||||||
|
|
|
|
|
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||||
Balance, March 31, 2020 |
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
||||
Net loss and total comprehensive loss for the period |
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
( |
) |
|
|
( |
) |
Cumulative translation adjustment |
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|
|
— |
|
|
|
|
||
Warrants exercised |
|
11, 12 |
|
|
|
|
|
|
|
|
( |
) |
|
|
— |
|
|
|
— |
|
|
|
|
|||
Net proceeds from shares issued under the at-the-market (ATM) program |
|
12(b) |
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
— |
|
|
|
|
|||
Stock based compensation |
|
|
|
|
|
|
|
|
|
|
|
|
|
— |
|
|
|
— |
|
|
|
|
||||
Balance at March 31, 2021 |
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
||||
The accompanying notes are an integral part of these consolidated financial statements
F-6
ACASTI PHARMA INC.
Consolidated Statements of Cash Flows
|
|
|
|
Year ended March 31, 2022 |
|
|
Year ended March 31, 2021 |
|
||
|
|
Notes |
|
$ |
|
|
$ |
|
||
Cash flows used in operating activities: |
|
|
|
|
|
|
|
|
||
Net loss for the year |
|
|
|
|
( |
) |
|
|
( |
) |
Adjustments: |
|
|
|
|
|
|
|
|
||
Amortization of intangible assets |
|
7 |
|
|
|
|
|
|
||
Depreciation of equipment |
|
8 |
|
|
|
|
|
|
||
Impairment of intangible assets |
|
7 |
|
|
|
|
|
|
||
Impairment of Equipment |
|
8 |
|
|
|
|
|
|
||
Impairment of other assets and prepaids |
|
8 |
|
|
|
|
|
|
||
Stock-based compensation expense |
|
15 |
|
|
|
|
|
|
||
Change in fair value of warrant liabilities |
|
11 |
|
|
( |
) |
|
|
|
|
Write off-of deferred financing costs of at-the-market (ATM) program |
|
|
|
|
|
|
|
|
||
Income tax recovery |
|
18 |
|
|
( |
) |
|
|
|
|
Unrealized foreign exchange loss |
|
|
|
|
( |
) |
|
|
|
|
Changes in non-cash working capital items |
|
17 |
|
|
( |
) |
|
|
( |
) |
Net cash used in operating activities |
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
||
Cash flows from (used in) investing activities: |
|
|
|
|
|
|
|
|
||
Acquisition of equipment |
|
6 |
|
|
|
|
|
( |
) |
|
Acquisition of short-term investments |
|
|
|
|
( |
) |
|
|
( |
) |
Maturity of short-term investments |
|
|
|
|
|
|
|
|
||
Net cash used in investing activities |
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
||
Cash flows from (used in) financing activities: |
|
|
|
|
|
|
|
|
||
Net proceeds from shares issued under the at-the-market (ATM) program |
|
|
|
|
|
|
|
|
||
Deferred financing costs |
|
|
|
|
|
|
|
( |
) |
|
Proceeds from exercise of warrants |
|
|
|
|
|
|
|
|
||
Proceeds from exercise of stock options |
|
|
|
|
|
|
|
|
||
Net cash from financing activities |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
Effect of exchange rate fluctuations on cash and cash equivalents |
|
|
|
|
|
|
|
|
||
Translation effect on cash and cash equivalents related to reporting currency |
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
||
Net (decrease) increase in cash and cash equivalents |
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Cash and cash equivalents, beginning of year |
|
|
|
|
|
|
|
|
||
Cash and cash equivalents, end of year |
|
|
|
|
|
|
|
|
||
Cash and cash equivalents are comprised of: |
|
|
|
|
|
|
|
|
||
Cash |
|
|
|
|
|
|
|
|
||
Cash equivalents |
|
|
|
|
|
|
|
|
||
F-7
ACASTI PHARMA INC.
Notes to the Consolidated Financial Statements
(Expressed in thousands of U.S. dollars except share data)
1.
Acasti Pharma Inc. (“Acasti” or the “Corporation”) is incorporated under the Business Corporations Act (Québec) (formerly Part 1A of the Companies Act (Québec)). The Corporation is domiciled in Canada and its registered office is located at 3009 boul. de la Concorde East, Suite 102, Laval, Québec, Canada H7E 2B5.
In January 2020 and August 2020, the Corporation released Phase 3 TRILOGY clinical study results for the Corporation’s lead drug candidate, CaPre. The TRILOGY studies did not meet the primary endpoint which resulted in the Corporation’s Board of Directors deciding not to proceed with a filing of an NDA with the FDA. With the completion of the TRILOGY studies beginning in the second half of fiscal 2021, marketing and research and development activities and expenses were reduced while management undertook a strategic review, and some CaPre related equipment and other assets were and continue to be classified as held for sale as they are expected to be sold.
In August 2021, the Corporation completed the acquisition via a share-for-share merger of Grace Therapeutics, Inc. (“Grace”) a privately held emerging biopharmaceutical company focused on developing innovative drug delivery technologies for the treatment of rare and orphan diseases. The post-merger Corporation is focused on building a late-stage specialty pharmaceutical company specializing in rare and orphan diseases and focused on developing and commercializing products that improve the standard of care using novel drug delivery technologies. The Corporation seeks to apply new proprietary formulations to existing pharmaceutical compounds to achieve enhanced efficacy, faster onset of action, reduced side effects, more convenient delivery and increased patient compliance; all of which could result in improved patient outcomes. The active pharmaceutical ingredients chosen by the Corporation for further development may be already approved in the target indication or could be repurposed for use in new indications.
The Corporation has incurred operating losses and negative cash flows from operations in each year since its inception. The Corporation expects to incur significant expenses and continued operating losses for the foreseeable future. The Corporation expects its expenses will increase substantially in connection with its ongoing activities, particularly as it advances clinical development for the first three drug candidates in the Corporation’s pipeline; continues to engage contract manufacturing organizations (“CMOs”) to manufacture its clinical study materials and to ultimately develop large-scale manufacturing capabilities in preparation for commercial launch; seeks regulatory approval for its product candidates; and adds personnel to support its product development and future product launch and commercialization.
The Corporation does not expect to generate revenue from product sales unless and until it successfully completes drug development and obtains regulatory approval, which the Corporation expects will take several years and is subject to significant uncertainty. To date, the Corporation has financed its operations primarily through public offerings and private placements of its common shares, warrants and convertible debt and the proceeds from research tax credits. Until such time that the Corporation can generate significant revenue from product sales if ever, it will require additional financing, which is expected to be sourced from a combination of public or private equity or debt financings or other non-dilutive sources, which may include fees, milestone payments and royalties from collaborations with third parties. Arrangements with collaborators or others may require the Corporation to relinquish certain rights related to its technologies or drug product candidates. Adequate additional financing may not be available to the Corporation on acceptable terms, or at all. The Corporation’s inability to raise capital as and when needed would have a negative impact on its financial condition and its ability to pursue its business strategy.
The Corporation remains subject to risks similar to other development stage companies in the biopharmaceutical industry, including compliance with government regulations, protection of proprietary technology, dependence on third party contractors and consultants and potential product liability, among others.
Reverse stock split
On August 26, 2021, the shareholders of the Corporation approved a resolution to undertake a reverse split of the common stock within a range of 1-6 to 1-8 with such specific ratio to be approved by the Acasti Board. All references in these financial statements to number of common shares, warrants and options, price per share and weighted average number of shares outstanding prior to the reverse split have been adjusted to reflect the approved reverse stock split of 1-
2.
Basis of presentation
These consolidated financial statements of Acasti Pharma Inc., which include the accounts of its subsidiary have been prepared in accordance with U.S. GAAP. All intercompany transactions and balances are eliminated on consolidation.
Use of estimates
The preparation of the financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, income, and expenses. Actual results may differ from these estimates.
Estimates are based on management’s best knowledge of current events and actions that management may undertake in the future. Estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimates are revised and in any future periods affected.
Estimates and assumptions include the measurement of derivative warrant liabilities (note 11) stock-based compensation (note 15)) assets held for sale (notes 8) the supply contract (note 20(a)) and acquisition of Grace and valuation of intangibles (note 4). Estimates and assumptions are also involved in measuring the accrual of services rendered with respect to research and developments expenditures at each reporting date, are determining which research and development expenses qualify for research and development tax credits and in what amounts. The Corporation recognizes the tax credits once it has reasonable assurance that they will be realized. Recorded tax credits are subject to review and approval by tax authorities and, therefore, could be different from the amounts recorded.
Functional and reporting currency
The Corporation’s functional currency is the Canadian dollar. The effects of exchange rate fluctuations on translating foreign currency monetary assets and liabilities into Canadian dollars are included in the statement of loss and comprehensive loss as foreign exchange gain/loss. Expense transactions are translated into the U.S. dollar reporting currency at the average exchange rate during the period, and assets and liabilities are translated at end of period exchange rates, except for equity transactions, which are translated at historical exchange rates.
F-8
Cash and Cash Equivalents
Investments
The Corporation’s investments consist of term deposits and are classified as held-to-maturity securities. These investments are recorded at amortized cost. Investments with original maturities exceeding three months and less than one year are categorized as short-term.
Receivables
Receivables are classified at amortized cost and recorded at the outstanding amount net of any provisions for uncollectible amount.
Deferred Financing Costs
Deferred financing costs consists of fees charged by underwriters, attorneys, accountants, and other fees directly attributable to future issuances of shares. Provided these costs are determined to be recoverable, these costs are deferred and charged subsequently against the gross proceeds of the related equity transaction when it occurs. If at such time, the Corporation deems that these costs are no longer recoverable, they will be expensed as a component of finance expenses.
Assets held for sale
Assets that are classified as held for sale are measured at the lower of their carrying amount or fair value less expected selling costs (“estimated selling price”) with a loss recognized to the extent that the carrying amount exceeds the estimated selling price. The classification is applicable at the date upon which the sale of assets is probable, and the assets are available for immediate sale in their present condition. Assets once classified as held for sale, are not subject to depreciation or amortization and both the assets and any liabilities directly associated with the assets held for sale are classified as current in the Corporation’s Consolidated Balance Sheets. Subsequent changes to the estimated selling price of assets held for sale are recorded as gains or losses to the Consolidated Statements of Income wherein the recognition of subsequent gains is limited to the cumulative loss previously recognized.
Equipment
Equipment is measured at cost less accumulated depreciation and accumulated impairment losses, if any.
Cost includes expenditures that are directly attributable to the acquisition of the asset, including all costs incurred in bringing the asset to its present location and condition. Purchased software that is integral to the functionality of the related equipment is capitalized as part of that equipment. Gains and losses on disposal of equipment are determined by comparing the proceeds from disposal with the carrying amount of equipment and are recognized net within operating expenses in the Consolidated Statement of Loss and Comprehensive Loss.
The costs of the day-to-day servicing of equipment are recognized in profit or loss as incurred.
Depreciation is recognized in profit or loss on either a straight-line basis or a declining basis over the estimated useful lives of each part of an item of equipment, since this most closely reflects the expected pattern of consumption of the future economic benefits embodied in the asset. Items of equipment are depreciated from the date that they are available for use or, in respect of assets not yet in service, from the date they are ready for their intended use.
The estimated useful lives and rates for the current and comparative periods are as follows:
Assets |
|
Method |
|
|
|
|
Rate |
|
|
|
|
|||
Furniture and office equipment |
|
Declining balance |
|
|
% |
|
to |
|
|
|
% |
|||
Computer equipment |
|
Declining balance |
|
|
|
|
|
% |
|
|
|
|||
Laboratory equipment |
|
Declining balance |
|
|
|
|
|
% |
|
|
|
|||
Production equipment |
|
Declining balance |
|
|
% |
|
to |
|
|
|
% |
|||
Depreciation methods, useful lives and residual values are reviewed periodically and adjusted prospectively if appropriate.
Goodwill and Intangible assets - acquired in-process research and development
In a business combination, the fair value of in-process research and development (“IPR&D”) acquired is capitalized and accounted for as indefinite-lived intangible assets, and not amortized until the underlying project receives regulatory approval, at which point the intangible assets will be accounted for as definite-lived intangible assets and amortized over the remaining useful life or discontinued. If discontinued, the intangible asset will be written off. Research and development (“R&D”) costs incurred after the acquisition are expensed as incurred.
The estimated fair values of identifiable intangible assets were determined using the multi-period excess earnings method, which is a valuation methodology that provides an estimate of the fair value of an asset based on market participant expectations of the cash flows an asset would generate over its remaining useful life. The significant assumptions used in the valuation are the discount rate, the probability of clinical success of research and development programs, obtaining regulatory approval and forecasted net sales.
Goodwill and indefinite-lived assets are not amortized but are subject to an impairment review annually and more frequently when indicators of impairment exist. An impairment of goodwill could occur if the carrying amount of a reporting unit exceeds the fair value of that reporting unit. An impairment of indefinite-lived intangible assets would occur if the fair value of the intangible asset is less than the carrying value.
F-9
The Corporation tests its goodwill for impairment by first assessing qualitative factors to determine whether it is more likely than not that the fair value is less than its carrying amount. If the Corporation concludes it is more likely than not that fair value of the reporting unit is less than its carrying amount, a quantitative impairment test is performed.
The Corporation tests indefinite-lived intangible assets for impairment by first assessing qualitative factors to determine whether it is more likely than not that the fair value is less than its carrying amount. If the Corporation concludes it is more likely than not that the fair value is less than it's carrying amount, a quantitative impairment test is performed. There were no triggering events from the date of acquisition of Grace to the end of the year with respect to goodwill and indefinite-lived intangible assets. The Corporation's annual impairment test will be performed in the third quarter of the fiscal year.
An impairment of $
Amortization group
Amortization is calculated over the cost of the intangible asset less its residual value. Amortization is recognized in profit or loss on a straight-line basis over the estimated useful lives of intangible assets from the date that they are available for use, since this most closely reflects the expected pattern of consumption of the future economic benefits embodied in the asset. T
Assets |
|
Period (years) |
|
|
Patents |
|
|
|
|
License |
|
|
||
Subsequent expenditure:
Subsequent expenditure is capitalized only when it increases the future economic benefits embodied in the specific asset to which it relates. All other expenditures, including expenditure on internally generated goodwill and brands, are recognized in profit or loss as incurred.
Impairment of Long-Lived Assets
The Corporation reviews the recoverability of its long-lived assets whenever events or changes in circumstances indicate that it is carrying amount may not be recoverable. The carrying amount is first compared with the undiscounted cash flows. If the carrying amount is higher than the sum of undiscounted cash flows, then the Corporation determines the fair value of the underlying asset group. Any impairment loss to be recognized is measured as the difference by which the carrying amount of the asset group exceeds the estimated fair value of the asset group. An impairment of $
Research and Development Costs
Research and developments expenditures are expensed as incurred. These costs primarily consist of employees’ salaries and benefits related to research and development activities, contractors and consultants that conduct the Corporation’s clinical trials, independent auditors and consultants to perform investigation activities on behalf of the Corporation, laboratory material and small equipment, clinical trial materials, stock-based compensation expense, and other non-clinical costs and regulatory fees. Advance payments for goods and services that will be used in future research and development are recognized in prepaids or other assets and are expensed when the services are performed, or the goods are used.
Stock based compensation
The Corporation has in place a stock option plan for directors, officers, employees, and consultants of the Corporation, with grants under the stock option plan approved by the Corporation’s Board of Directors. The plan provides for the granting of options to purchase Common Shares and the exercise price of each option equals the closing trading price of Common Shares on the day prior to the grant. The terms and conditions for acquiring and exercising options are set by the Corporation’s Board of Directors in accordance with and subject to the terms and conditions of the stock option plan. The Corporation measures the cost of such awards based on the fair value of the award at grant date, net of estimated forfeiture, and recognizes stock-based compensation expense in the Consolidated Statements of Loss and Comprehensive Loss on a graded vesting basis over the requisite service period. The requisite service period equals the vesting periods of the awards. The fair value of options is estimated for each tranche of an award that vests on a graded basis. The fair value of options is estimated using the Black-Scholes option pricing model, which uses various inputs including estimated fair value of the Common Shares at the grant date, expected term, estimated volatility, risk-free interest rate and expected dividend yields of the Common Shares. The Corporation applies an estimated forfeiture rate derived from historical employee termination behaviour. If the actual forfeitures differ from those estimated by management, adjustment to compensation expense may be required in future periods.
Non-employee stock-based compensation transactions in which the Corporation receives goods or services as consideration for its own equity instruments are accounted for as stock-based compensation transactions. The Corporation establishes the fair value at the grant date for non-employee awards and measures the fair value based on the fair value of equity instruments issued. The fair value of a non-employee award is estimated using the Black-Scholes option pricing model, which uses various inputs including estimated fair value of the Common Shares at the grant date, contractual term, estimated volatility, risk-free interest rate and expected dividend yields of the Common Shares.
Government grants
Government grants are recorded as a reduction of the related expense or cost of the asset acquired. Government grants are recognized when there is reasonable assurance that the Corporation has met the requirements of the approved grant program and there is reasonable assurance that the grant will be received.
Grants that compensate the Corporation for expenses incurred are recognized in profit or loss in reduction thereof on a systematic basis in the same years in which the expenses are recognized. Grants that compensate the Corporation for the cost of an asset are recognized in profit or loss on a systematic basis over the useful life of the asset.
Leases
At the inception of an arrangement, the Corporation determines whether the arrangement is or contains a lease based on the unique facts and circumstances present in the arrangement. Operating lease liabilities and their corresponding right-of-use assets are initially recorded based on the present value of lease payments over the expected remaining lease term. Certain adjustments to the right-of-use asset may be required for items such as incentives received. The interest rate implicit in lease contracts is typically not readily determinable. As a result, the Corporation utilizes its incremental borrowing rate to discount lease payments, which reflects the fixed rate at which the Corporation could borrow on a collateralized basis the amount of the lease payments in the same currency, for a similar term, in a similar economic environment. .
F-10
The Corporation has elected not to recognize leases with an original term of one year or less on the balance sheet. The Corporation typically only includes an initial lease term in its assessment of a lease arrangement. Options to renew a lease are not included in the Corporation’s assessment unless there is reasonable certainty that the Corporation will renew. The Corporation’s lease expense is recognized in research and development expenses. The Corporation does not have financing leases.
Income tax
Income tax expense comprises current and deferred taxes. Current and deferred taxes are recognized in profit or loss except to the extent that they relate to items recognized directly in equity or in other comprehensive income.
Current tax is the expected tax payable or receivable on the taxable income or loss for the year, using tax rates enacted at the reporting date, and any adjustment to tax payable in respect of previous years.
Deferred tax is recognized in respect of temporary differences between the carrying amounts (tax base) of assets and liabilities for financial reporting purposes and the amounts used for taxation purposes. Deferred tax assets and liabilities are measured at the tax rate expected to apply when the underlying asset or liability is realised (settled) based on the rates that are enacted at the reporting date. Deferred tax assets and liabilities are offset if the Corporation has the right to set off the amount owed by with the amount owed by the other party, the Corporation intends to set off and the offset right is enforceable at law. A deferred tax asset is recognized for unused tax losses and tax credits, reduced by a valuation allowance to the extent that it is more likely than not that some portion or all of the deferred tax asset will not be realized.
Earnings per share
The Corporation presents basic and diluted earnings per share (EPS) data for its Common Shares. Basic EPS is calculated by dividing the profit or loss attributable to the holders of Common Shares by the weighted average number of Common Shares outstanding during the year. Diluted EPS is determined by adjusting the profit or loss attributable to the holders of Common Shares and the weighted average number of Common Shares outstanding adjusted for the effects of all dilutive potential Common Shares, which comprise warrants and share options granted to employees.
Segment reporting
An operating segment is a component of the Corporation that engages in business activities from which it may earn revenues and incur expenses. The Corporation has
Derivative financial instruments
The Corporation has issued warrants of which some are accounted for as liability-classified derivatives over its own equity. Derivatives are recognized initially at fair value; attributable transaction costs are recognized in profit and loss as incurred. Subsequent to initial recognition, derivatives are measured at fair value, and all changes in their fair value are recognized immediately in profit or loss as a component of financial expenses.
Other equity instruments
Warrants that do not meet the definition of a liability instrument are recognized in equity as additional paid in capital.
Fair Value Measurements
Certain of the Corporation’s accounting policies and disclosures require the determination of fair value, for both financial assets and liabilities. Fair values have been determined for measurement and/or disclosure purposes based on the following methods.
Financial assets and liabilities
In establishing fair value, the Corporation uses a fair value hierarchy based on levels as defined below:
The Corporation has determined that the carrying values of its short-term financial assets and liabilities (cash and cash equivalents, short-term investments and trade and other payables) approximate their fair value given the short-term nature of these instruments. The Corporation measured its derivative warrant liabilities at fair value on a recurring basis using level 3 inputs.
3. Recent Accounting Pronouncements
The Corporation has considered recent accounting pronouncements and concluded that they are either not applicable to the business or that the effect is not expected to be material to the consolidated financial statements as a result of future adoption.
4. Acquisition of Grace
On August 27, 2021, the Corporation completed its acquisition of all outstanding equity interests in Grace Therapeutics Inc, via a merger. Grace, based in New Jersey and organized under the laws of Delaware, was a rare and orphan disease specialty pharmaceutical company.
In connection with the share-for-share noncash transaction, Grace was merged with a new wholly owned subsidiary of Acasti and became a subsidiary of Acasti. As a result, Acasti acquired Grace’s entire therapeutic pipeline consisting of three unique clinical stage and multiple pre-clinical stage assets supported by an intellectual property portfolio consisting of various granted and pending patents in various jurisdictions worldwide. Under the terms of the acquisition, each issued and outstanding share of Grace common stock was automatically converted into the right to receive Acasti common shares equal to the equity exchange ratio set forth in the merger agreement.
F-11
Consideration for acquisition
A total of
|
|
|
|
|
Total common shares issued |
|
|
|
|
Acasti share price (closing share price on August 27, 2021) |
|
$ |
|
|
Fair value of common shares issued |
|
$ |
|
|
The acquisition of Grace has been accounted for as a business combination using the acquisition method of accounting. The fair value of the purchase price was allocated to the assets acquired and liabilities assumed at their respective fair values. Management estimated the fair value of the IPR&D intangible assets using a multi-period excess earnings method. The significant assumptions used in the valuation are the discount rate, the probability of clinical success of research and development programs, obtaining regulatory approval and forecasted net sales. This acquisition method requires, among other things, that assets acquired, and liabilities assumed in a business combination be recognized at their fair values as of the acquisition date. The valuation of assets acquired, and liabilities assumed has been finalized during the fourth quarter of 2022.
Measurement period adjustments to the preliminary purchase price allocation during 2022 included (i) an increase to intangible assets of $
The following table summarizes the final fair value of assets acquired and liabilities assumed as of the acquisition date:
|
|
$ |
|
|
Assets acquired and liabilities assumed |
|
|
|
|
Cash and equivalents |
|
|
|
|
Prepaid expenses and other current assets |
|
|
|
|
Intangible assets – in-process research and development |
|
|
|
|
Goodwill |
|
|
|
|
Accounts payable and accrued expenses |
|
|
( |
) |
Deferred tax liability |
|
|
( |
) |
Total assets acquired and liabilities assumed |
|
|
|
|
Intangible assets of $
|
|
$ |
|
|
Intangible assets – in-process research and development |
|
|
|
|
GTX 104 |
|
|
|
|
GTX 102 |
|
|
|
|
GTX 101 |
|
|
|
|
Total |
|
|
|
|
Management estimated the fair value of the IPR&D intangible assets using a multi-period excess earnings method. The significant assumptions used in the valuation are the discount rate, the probability of clinical success of research and development programs, obtaining regulatory approval and forecasted net sales.
Goodwill of $
Acquisition-related expenses, which were comprised primarily of regulatory, financial advisory and legal fees, totalled $
Pro forma financial information
The following table presents the unaudited pro forma combined results of Acasti and Grace for the year ended March 31, 2022, as if the acquisition of Grace had occurred on April 1, 2020:
|
|
|
|
Year ended March 31, 2022 |
|
|
|
|
|
|
$ |
|
|
Net loss |
|
|
|
|
( |
) |
The unaudited pro forma condensed combined financial information was prepared using the acquisition method of accounting and was based on the historical financial information of Acasti and Grace. The unaudited pro forma financial information is not necessarily indicative of what the consolidated results of operations would have been had the acquisition been completed on April 1, 2020. In addition, the unaudited pro forma financial information is not a projection of future results of operations of the combined company, nor does it reflect the realization of any synergies or cost savings associated with the acquisition.
F-12
5. Receivables
|
|
|
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
|||
|
|
Notes |
|
|
$ |
|
|
$ |
|
|||
Sales tax receivables |
|
|
|
|
|
|
|
|
|
|||
Government assistance |
|
|
9 |
|
|
|
|
|
|
|
||
Interest receivable |
|
|
|
|
|
|
|
|
|
|||
Other receivables |
|
|
|
|
|
|
|
|
|
|||
Total receivables |
|
|
|
|
|
|
|
|
|
|||
6. Short-term Investments
The Corporation holds various short term investments with maturities greater than 3 months at the time of purchase as follows:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Term deposits issued in US currency earning interest at |
|
|
|
|
|
|
||
Term deposits issued in CAD currency earning interest at ranges between |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
Total short-term investments |
|
|
|
|
|
|
||
7. Impairment loss Intangible assets
In prior years, the Corporation entered into agreements with Neptune Wellness Solutions Inc. ("Neptune") pursuant to which the Corporation obtained a license and exercised its option under the license agreement to pay in advance future royalties payable to Neptune. This license allowed the Corporation to exploit the intellectual property rights in order to conduct clinical trials for its CaPre drug candidate. During the second quarter of fiscal 2021, the Corporation released its Phase 3 clinical programs data and its failure to meet its primary endpoints, and the resulting decision to not file an NDA to obtain FDA approval for CaPre and therefore undertook an analysis to determine the fair value of the intangible asset.
In assessing the magnitude of any impairment of the license the Corporation considered all available evidence, including (i) significant adverse impact from business climate due to the Phase 3 clinical program’s failure to meet its primary endpoints, and the resulting decision to not file an NDA to obtain FDA approval for CaPre, and the resulting internal forecasts that no cash flows from the use of the license was possible, and (ii) management’s estimate that a market place participant would place minimal to no value on the license if it were to be sold on its own or in combination with other assets, recognized or not, which is a level 3 measurement in the fair value hierarchy which included unobservable inputs. Accordingly, an impairment loss of $
8. Assets held for sale
During the period the Corporation committed to a plan and is actively marketing for sale Other assets and Equipment and has met the criteria for classification of assets held for sale:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Other assets (a) |
|
|
|
|
|
|
||
Equipment (b) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
a. Other assets
Other assets represent krill oil (RKO) held by the Corporation that was expected to be used in the conduct of R&D activities and commercial inventory scale up related to the development and commercialization of the CaPre drug. Given that the development of CaPre will no longer be pursued, the Corporation is expected to sell this reserve. The other asset is being recorded at the fair value less costs to sell, which has resulted in an impairment loss of $
b. Equipment
March 31, 2022 |
|
Cost, net of impairment |
|
|
Accumulated |
|
|
Net book |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Furniture and office equipment |
|
|
|
|
|
( |
) |
|
|
|
||
Computer equipment |
|
|
|
|
|
( |
) |
|
|
|
||
Laboratory equipment |
|
|
|
|
|
( |
) |
|
|
|
||
Production equipment |
|
|
|
|
|
( |
) |
|
|
|
||
|
|
|
|
|
|
( |
) |
|
|
|
||
F-13
March 31, 2021 |
|
Cost |
|
|
Accumulated |
|
|
Impairment |
|
|
Net book |
|
||||
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Furniture and office equipment |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|||
Computer equipment |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
||
Laboratory equipment |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
||
Production equipment |
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
||
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
||
For the year ended March 31, 2021, depreciation expense was $
9. Government assistance
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Investment tax credit |
|
|
|
|
|
|
||
Government assistance is comprised of a government grant from the Canadian federal government and research and development investment tax credits receivable from the Quebec provincial government which relate to qualifiable research and development expenditures under the applicable tax laws. The amounts recorded as receivables are subject to a government tax audit and the final amounts received may differ from those recorded. For the years ended March 31, 2022 and 2021, the Corporation recorded $
The amounts recorded as receivables are subject to a government tax audit and the final amounts received may differ from those recorded. Unrecognized Canadian federal tax credits may be used to reduce future Canadian federal income tax and expire as follows:
|
|
$ |
|
|
2029 |
|
|
|
|
2030 |
|
|
|
|
2031 |
|
|
|
|
2032 |
|
|
|
|
2033 |
|
|
|
|
2034 |
|
|
|
|
2035 |
|
|
|
|
2036 |
|
|
|
|
2037 |
|
|
|
|
2038 |
|
|
|
|
2039 |
|
|
|
|
2040 |
|
|
|
|
2041 |
|
|
|
|
2042 |
|
|
|
|
|
|
|
|
|
In September 2019, the Corporation was awarded up to CAD $
In October 2020, the Corporation received correspondence from the NRC IRAP that the eligible amount awarded to the Corporation for non-dilutive and non-repayable funding was reduced from up to CAD $
10. Trade and other payables
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Trade payables |
|
|
|
|
|
|
||
Accrued liabilities and other payables |
|
|
|
|
|
|
||
Employee salaries and benefits payable |
|
|
|
|
|
|
||
Total trade and other payables |
|
|
|
|
|
|
||
11. Derivative warrant liabilities
In connection with the Canadian public offering of units consisting of common shares and warrants that closed on May 9, 2018, the Corporation issued a total of
In connection with the U.S. public offering units consisting of common shares and warrants that closed on December 27, 2017, the Corporation issued a total of
F-14
The derivative warrant liabilities are measured at fair value at each reporting period and the reconciliation of changes in fair value is presented in the following tables:
|
|
Warrants issued May 2018 |
|
|
Warrants issued December 27, 2017 |
|
||||||||||
|
|
March 31, |
|
|
March 31, |
|
|
March 31, |
|
|
March 31, |
|
||||
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Balance – beginning of year |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Change in fair value |
|
|
( |
) |
|
|
|
|
|
( |
) |
|
|
|
||
Translation effect |
|
|
( |
) |
|
|
|
|
|
— |
|
|
|
|
||
Balance – end of year |
|
|
|
|
|
|
|
|
— |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Fair value per warrant issuable |
|
|
|
|
|
|
|
|
— |
|
|
|
|
|||
The fair value of the derivative warrant liabilities was estimated using the Black-Scholes option pricing model and based on the following assumptions:
|
|
Warrant liabilities issued |
|
|
Warrant liabilities issued |
|
||||||||||
|
|
March 31, |
|
|
March 31, |
|
|
March 31, |
|
|
March 31, |
|
||||
|
|
$ |
|
|
$ |
|
|
$ |
|
|
$ |
|
||||
Exercise price |
|
CAD $ |
|
|
CAD $ |
|
|
USD $ |
|
|
USD $ |
|
||||
Share price |
|
CAD $ |
|
|
CAD $ |
|
|
USD $ |
|
|
USD $ |
|
||||
Risk-free interest |
|
|
% |
|
|
% |
|
|
% |
|
|
% |
||||
Contractual life (years) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Expected volatility |
|
|
% |
|
|
% |
|
|
% |
|
|
% |
||||
The Corporation measured its derivative warrant liabilities at fair value on a recurring basis. These financial liabilities were measured using level 3 inputs (see Note 11).
As at March 31, 2022, the effect of an increase or a decrease of 5% of the volatility used, which is the significant unobservable input in the fair value estimate, would have a nominal impact.
12. Capital and other components of equity
a. Common Shares
Authorized capital stock
Unlimited number of shares
“At-the-market” sales agreement
On February 14, 2019, the Corporation entered into an “at-the-market” (ATM) sales agreement with B. Riley FBR, Inc. (“B. Riley”) pursuant to which the Common Shares may be sold from time to time for aggregate gross proceeds of up to $
On June 29, 2020, the Corporation entered into an amended and restated sales agreement (the Sales Agreement) with B. Riley, Oppenheimer& Co. Inc. and H.C. Wainwright & Co., LLC (collectively, the “Agents”) to amend the existing ATM program. Under the terms of the Sales Agreement, which has a three-year term, the Corporation may issue and sell from time to time its common shares (the Shares) having an aggregate offering price of up to US $
On November 10, 2021, the Corporation filed a prospectus supplement relating to its at-the-market program with B. Riley, Oppenheimer& Co. Inc. and H.C. Wainwright & Co., LLC acting as agents. Under the terms of the ATM Sales Agreement and the prospectus supplement, the Corporation may issue and sell from time-to-time common shares having an aggregate offering price of up to $
F-15
in General and administrative expenses. For the year ended March 31, 2022,
For the year ended March 31, 2021, $
b. Warrants
The warrants of the Corporation are composed of the following:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||||||||||
|
|
Number |
|
|
Amount |
|
|
Number |
|
|
Amount |
|
||||
|
|
|
|
|
$ |
|
|
|
|
|
$ |
|
||||
Liability |
|
|
|
|
|
|
|
|
|
|
|
|
||||
May 2018 public offering warrants 2018 (i) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Series December 2017 U.S. public offering warrants 2017 (ii) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Equity |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Public offering warrants |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Public offering U.S. broker warrants December 2017 (iii) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Public offering warrants February 2017 (iv) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
(i)
(ii)
(iii)
(iv)
During the year ended March 31, 2022, no warrants were exercised. During the year ending March 31, 2021,
13. Revenues
In October 2020, the Corporation entered into an agreement with the Centre Integre Universitaire et des services sociaux de L’Estrie - Centre hospitalier Universitaire de Sherbrooke to start producing and selling Viral transport medium tubes to be utilized in testing related to the Covid-19 pandemic. Revenue is recognized when the product is received by the customer.
14. Net financial income (expenses)
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Foreign exchange gain (loss) |
|
|
( |
) |
|
|
( |
) |
Write-off of deferred financing fees related to at-the-market (ATM) program |
|
|
|
|
|
( |
) |
|
Interest income |
|
|
|
|
|
|
||
Other income |
|
|
|
|
|
|
||
Change in fair value of warrant liabilities |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
||
Financial income (expenses) |
|
|
|
|
|
( |
) |
|
15. Stock based compensation
At March 31, 2021, the Corporation has the following stock-based compensation arrangement:
a. Corporation stock option plan
The Corporation has in place a stock option plan for directors, officers, employees, and consultants of the Corporation. An amendment of the stock option plan was approved by shareholders on August 26, 2021. The amendment provides for an change to the existing limits for Common Shares reserved for issuance under the Stock Option Plan.
The Stock Option Plan continues to provide for the granting of options to purchase common shares. The exercise price of the stock options granted under this amended plan is not lower than the closing price of the common shares on the TSXV at the close of markets the day preceding the grant. The maximum number of common shares that may be issued upon exercise of options granted under the amended Stock Option Plan shall not exceed 10% of the aggregate number of issued and outstanding shares of the Corporation. This resulted in an increase from
The total number of shares issued to any one consultant within any twelve-month period cannot exceed
F-16
Shares (on a non-diluted basis) on the date an option is granted, or (b) any one eligible person in a twelve-month period exceeding
The following tables summarize information about activities within the stock option plan:
|
|
Number of |
|
|
Weighted average |
|
|
Weighted average |
|
|||
|
|
|
|
|
CAD $ |
|
|
CAD $ |
|
|||
Outstanding, March 31, 2020 |
|
|
|
|
|
|
|
|
|
|||
Granted |
|
|
|
|
|
|
|
|
|
|||
Exercised |
|
|
( |
) |
|
|
|
|
|
|
||
Forfeited |
|
|
( |
) |
|
|
|
|
|
|
||
Expired |
|
|
|
|
|
|
|
|
|
|||
Outstanding, March 31, 2021 |
|
|
|
|
|
|
|
|
|
|||
Granted |
|
|
|
|
|
|
|
|
|
|||
Exercised |
|
|
|
|
|
|
|
|
|
|||
Forfeited |
|
|
( |
) |
|
|
|
|
|
|
||
Expired |
|
|
|
|
|
|
|
|
|
|||
Outstanding, March 31, 2022 |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Exercisable at end of year |
|
|
|
|
|
|
|
|
|
|||
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
Weighted average fair value of the options granted to employees and directors of the Corporation- |
|
|
|
|
|
|
||
Compensation expense recognized under the stock option plan is summarized as follows:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Research and development expenses |
|
|
|
|
|
|
||
General and administrative expenses |
|
|
|
|
|
|
||
Sales and marketing expenses |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
||
As of March 31, 2022, there was CAD $
A summary of the non-vested stock option activity and related information for the Corporation’s stock options granted is as follows:
|
|
Number of |
|
|
Weighted average |
|
||
Non- vested, March 31, 2021 |
|
|
|
|
|
|
||
Options granted |
|
|
|
|
|
|
||
Options vested |
|
|
( |
) |
|
|
|
|
Options forfeited and cancelled |
|
|
( |
) |
|
|
|
|
Non- vested, March 31, 2022 |
|
|
|
|
|
|
||
The fair value of options granted was estimated using the Black-Scholes option pricing model, resulting in the following weighted average assumptions for options granted during the periods ended:
|
|
March 31, 2022 |
|
|
|
|
Weighted average- CAD |
|
|
Exercise price |
|
$ |
|
|
Share price |
|
$ |
|
|
Dividend |
|
|
|
|
Risk-free interest |
|
|
% |
|
Estimated life (years) |
|
|
% |
|
Expected volatility |
|
|
% |
|
F-17
The following tables summarize information about activities within the stock option plan:
March 31, 2022 |
|
|||||||||||||||||||||
Exercise |
|
|
|
|
|
|
|
|
Weighted average |
|
|
Number of options |
|
|
Number of options |
|
||||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
$ |
|
|
|
— |
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Stock-based compensation payment transactions and broker warrants
The fair value of stock-based compensation transactions is measured using the Black-Scholes option pricing model. Measurement inputs include share price on measurement date, exercise price of the instrument, expected volatility (based on weighted average historic volatility for a duration equal to the weighted average life of the instruments, life based on the average of the vesting and contractual periods for employee awards as minimal prior exercises of options in which to establish historical exercise experience; contractual life for broker warrants), and the risk-free interest rate (based on government bonds). Service and performance conditions attached to the transactions, if any, are not considered in determining fair value. The expected life of the stock options is not necessarily indicative of exercise patterns that may occur. The expected volatility reflects the assumption that the historical volatility over a period similar to the life of the options is indicative of future trends, which may also not necessarily be the actual outcome.
b. Corporation equity incentive plan
The Corporation established an equity incentive plan for employees, directors and consultants. The plan provides for the issuance of restricted share units (RSUs), performance share units, restricted shares, deferred share units and other stock-based awards, subject to restricted conditions as may be determined by the Board of Directors. There were
16. Loss per share
Diluted loss per share was the same amount as basic loss per share, as the effect of options, RSUs and warrants would have been anti-dilutive, as the Corporation has incurred losses in each of the periods presented. All outstanding options, RSUs and warrants could potentially be dilutive in the future.
17. Supplemental cash flow disclosure
a. Changes in working capital items:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Receivables |
|
|
( |
) |
|
|
|
|
Prepaid expenses |
|
|
( |
) |
|
|
|
|
Trade and other payables |
|
|
( |
) |
|
|
( |
) |
Other assets |
|
|
|
|
|
|
||
Total changes in working capital items |
|
|
( |
) |
|
|
( |
) |
18. Income taxes
Income tax (recovery) expense:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Current tax (recovery) expense |
|
|
|
|
|
|
||
Deferred tax (recovery) expense |
|
|
( |
) |
|
|
|
|
Income tax (recovery) expense |
|
|
( |
) |
|
|
|
|
F-18
Reconciliation of effective tax rate:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Loss before income taxes |
|
|
( |
) |
|
|
( |
) |
Basic combined Canadian statutory income tax rate 1 |
|
|
% |
|
|
% |
||
Computed income tax recovery |
|
|
( |
) |
|
|
( |
) |
Increase resulting from: |
|
|
|
|
|
|
||
Difference in foreign tax rates |
|
|
( |
) |
|
|
|
|
Non-deductible stock-based compensation |
|
|
|
|
|
|
||
Non-deductible change in fair value of warrants |
|
|
( |
) |
|
|
|
|
Non-deductible transaction costs |
|
|
|
|
|
|
||
Non-refundable Federal ITC |
|
|
( |
) |
|
|
|
|
Change in valuation allowance |
|
|
|
|
|
|
||
Other – Foreign exchange |
|
|
|
|
|
( |
) |
|
Other |
|
|
|
|
|
|
||
Total tax (recovery) expense |
|
|
( |
) |
|
|
|
|
1 The Canadian combined statutory income tax rate has decreased due to a reduction in the provincial statutory income tax rate.
Net deferred income tax assets as of March 31, 2022, and 2021 were comprised of the following:
|
|
March 31, 2022 |
|
|
March 31, 2021 |
|
||
|
|
$ |
|
|
$ |
|
||
Deferred tax assets |
|
|
|
|
|
|
||
Tax losses carried forward |
|
|
|
|
|
|
||
Research and development expenses |
|
|
|
|
|
|
||
Property, plan and equipment |
|
|
|
|
|
|
||
Financing expenses |
|
|
|
|
|
|
||
Licenses |
|
|
|
|
|
|
||
Tax credit carry forwards |
|
|
|
|
|
|
||
Other temporary differences |
|
|
|
|
|
|
||
Deferred tax assets |
|
|
|
|
|
39,331 |
|
|
Deferred tax liabilities |
|
|
|
|
|
|
||
Property, plan and equipment and intangible assets |
|
|
( |
) |
|
|
|
|
Deferred tax liabilities |
|
|
( |
) |
|
|
|
|
Valuation allowance |
|
|
( |
) |
|
|
( |
) |
Net deferred tax liabilities |
|
|
( |
) |
|
|
|
|
As at March 31, 2022, the amounts and expiry dates of tax attributes and temporary differences, which are available to reduce future years’ taxable income, were as follows:
|
|
|
|
|
|
|
|
March 31, 2022 |
|
|||
|
|
Federal |
|
|
Provincial |
|
|
United States |
|
|||
|
|
$ |
|
|
$ |
|
|
$ |
|
|||
Tax losses carried forward |
|
|
|
|
|
|
|
|
|
|||
2028 |
|
|
|
|
|
|
|
|
|
|||
2029 |
|
|
|
|
|
|
|
|
|
|||
2030 |
|
|
|
|
|
|
|
|
|
|||
2031 |
|
|
|
|
|
|
|
|
|
|||
2032 |
|
|
|
|
|
|
|
|
|
|||
2033 |
|
|
|
|
|
|
|
|
|
|||
2034 |
|
|
|
|
|
|
|
|
|
|||
2035 |
|
|
|
|
|
|
|
|
|
|||
2036 |
|
|
|
|
|
|
|
|
|
|||
2037 |
|
|
|
|
|
|
|
|
|
|||
2038 |
|
|
|
|
|
|
|
|
|
|||
2039 |
|
|
|
|
|
|
|
|
|
|||
2040 |
|
|
|
|
|
|
|
|
|
|||
2041 |
|
|
|
|
|
|
|
|
|
|||
2042 |
|
|
|
|
|
|
|
|
|
|||
No expiry |
|
|
|
|
|
|
|
|
|
|||
Total |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Research and development expenses, without time limitation |
|
|
|
|
|
|
|
|
|
|||
Unrecognized tax benefits
The Corporation does not expect a significant change to the amount of unrecognized tax benefits over the next 12 months. However, any adjustments arising from certain ongoing examinations by tax authorities could alter the timing or amount of taxable income or deductions, of the allocation of income among tax jurisdictions, and these adjustments could differ from the amount accrued. The Corporation’s federal and provincial income tax returns filed for all years remain subject to examination by the taxation authorities.
F-19
19. Financial instruments
a. Concentration of credit risk
Financial instruments that potentially subject the Corporation to a concentration of credit risk consist primarily of cash and cash equivalents and investments. Cash and cash equivalents and investments are all invested in accordance with the Corporation’s Investment Policy with the primary objective being the preservation of capital and the maintenance of liquidity, which is managed by dealing only with highly rated Canadian institutions. The carrying amount of financial assets, as disclosed in the statements of financial position, represents the Corporation’s credit exposure at the reporting date.
b. Foreign currency risk
The Corporation is exposed to the financial risk related to the fluctuation of foreign exchange rates and the degrees of volatility of those rates. Foreign currency risk is limited to the portion of the Corporation's business transactions denominated in currencies other than the Corporations functional currency of the Canadian dollar. Fluctuations related to foreign exchange rates could cause unforeseen fluctuations in the Corporation's operating results. The Corporation does not use derivative instruments to hedge exposure to foreign exchange risk. The fluctuation of the U.S. dollar in relation to the Canadian dollar and other foreign currencies will consequently have an impact upon the Corporation’s net loss.
The operating results and financial position of the Corporation are reported in U.S. dollars (reporting currency) in the Corporation’s financial statements.
c. Liquidity risk
Liquidity risk is the risk that the Corporation will encounter difficulty in meeting the obligations associated with its financial liabilities that are settled by delivering cash or another financial asset. The Corporation manages liquidity risk through the management of its capital structure and financial leverage. It also manages liquidity risk by continuously monitoring actual and projected cash flows. The Board of Directors reviews and approves the Corporation's operating budgets, and reviews material transactions outside the normal course of business. The Corporation currently does not have long-term debt nor arranged committed sources of financing and is operating via use of existing cash and short-term investment balances. Refer to Note 1 – Nature of Operations.
The Corporation’s financial liabilities obligations include trade and other payables, which fall due within the next 12 months in addition to the warrant derivatives that fall due beyond 12 months and are likely to be settled by the Corporation’s equity.
20. Commitments and contingencies
Research and development contracts and contract research organizations agreements
We utilize contract manufacturing organizations, for the development and production of clinical materials and contract research organizations to perform services related to our clinical trials. Pursuant to the agreements with these contract manufacturing organizations and contract research organizations, we have either the right to terminate the agreements without penalties or under certain penalty conditions.
Supply contract
On October 25, 2019, the Corporation signed a supply agreement with Aker Biomarine Antartic. (“Aker”) to purchase raw krill oil product for a committed volume of commercial starting material for CaPre for a total fixed value of $
Sherbrook Lease
On March 14, 2022, we renewed the lease agreement effective April 1, 2022, for our research and development and quality control laboratory facility located in Sherbrooke, Québec, resulting in a commitment of $
Legal proceedings and disputes
In the ordinary course of business, the Corporation is at times subject to various legal proceedings and disputes. The Corporation assesses its liabilities and contingencies in connection with outstanding legal proceedings utilizing the latest information available. Where it is probable that the Corporation will incur a loss and the amount of the loss can be reasonably estimated, the Corporation records a liability in its consolidated financial statements. These legal contingencies may be adjusted to reflect any relevant developments. Where a loss is not probable or the amount of loss is not estimable, the Corporation does not accrue legal contingencies. While the outcome of legal proceedings is inherently uncertain, based on information currently available, management believes that it has established appropriate legal reserves. Any incremental liabilities arising from pending legal proceedings are not expected to have a material adverse effect on the Corporation’s financial position, results of operations, or cash flows. However, it is possible that the ultimate resolution of these matters, if unfavorable, may be material to the Corporation’s financial position, results of operations, or cash flows. No reserves or liabilities have been accrued as at March 31, 2022.
21. Subsequent events
Functional currency
On April 1, 2022, the Corporation’s functional currency was changed from the Canadian dollar to the US dollar. This change will be reflected prospectively in the Corporation’s financial statements beginning with the first quarter of fiscal 2023.
Common shares
Subsequent to March 31, 2022, the Corporation sold an additional
F-20